Download presentation
Presentation is loading. Please wait.

1
Dialyzer Selection Sirirat Reungjui, MD. Khon Kaen University

2
Add your text in here Content 1. 1. Type of dialyzer and membrane 2. Selection of dialyzer Effect on outcomes 3.

3
Evolution of dialyzer Kolff Rotating Drum, Ca. 1943 Kolff Rotating Drum, Ca. 1943 Skeggs Leonards Plate, Ca. 1948 Skeggs Leonards Plate, Ca. 1948 Travenol-Kolff Coil, Ca. 1956 Travenol-Kolff Coil, Ca. 1956 Kiil Plate Dialyzer, Ca. 1960 Kiil Plate Dialyzer, Ca. 1960 Stewart Capillary Cordis Dow CDAKs First Hollow Fiber Dialyzers, Ca. 1964 - 1967 Stewart Capillary Cordis Dow CDAKs First Hollow Fiber Dialyzers, Ca. 1964 - 1967 Gambro Plate Dialyzers, Ca. 1967 - 1979 Gambro Plate Dialyzers, Ca. 1967 - 1979 Baxter CA170 High Efficiency Baxter CA170 High Efficiency Baxter CT190G High Flux Baxter CT190G High Flux FMC F80 High Flux FMC F80 High Flux

4
Structure Blood inlet Blood outlet Fiber Header Jecket Solution inlet Solution outlet

5
Ideal dialyzer Remove small and large solutes Reliable convective and UF properties Biocompatible / Safety Protect blood from dialysate contaminants (backfiltration) Remove small and large solutes Reliable convective and UF properties Biocompatible / Safety Protect blood from dialysate contaminants (backfiltration)
 Remove small and large solutes Reliable convective and UF properties Biocompatible / Safety Protect blood from dialysate contaminants (backfiltration)")
6
Retention of solutes Uremic syndrome Deterioration of multiple biochemical & physiological functions Deterioration of multiple biochemical & physiological functions Progressive renal failure Uremic toxins

7
Larger, middle-molecules ( > 500 D) Larger, middle-molecules ( > 500 D) Lipid-soluble and/or protein-bound Uremic toxins Small, water-soluble, non-protein-bound ( < 500 D) European Uremic Toxin Work Group. JASN, 2012.

8
Diffusion Concentration gradient, small molecule

9
Movement of water (ultrafiltration), middle mol. Convection
, middle mol. Convection")
10
Complementactivation Hydroxylgroups CytokineROS Neutophil,Monocyte Contaminant dialysate

11
Type A (anaphylactic type) Ethylene oxide, AN-69 (ACEI), contaminant dialysate, heparin, complement release ?, eosinophilia Type B (nonspecific) Complement activation Type A (anaphylactic type) Ethylene oxide, AN-69 (ACEI), contaminant dialysate, heparin, complement release ?, eosinophilia Type B (nonspecific) Complement activation Dialyzer reactions
 Ethylene oxide, AN-69 (ACEI), contaminant dialysate, heparin, complement release , eosinophilia Type B (nonspecific) Complement activation Type A (anaphylactic type) Ethylene oxide, AN-69 (ACEI), contaminant dialysate, heparin, complement release , eosinophilia Type B (nonspecific) Complement activation Dialyzer reactions")
12
Bioincompatibility Amyloidosis – β 2 microglobulin Immune depression Loss of residual renal function Catabolism and malnutrition Inflammation/ Atherosclerosis Amyloidosis – β 2 microglobulin Immune depression Loss of residual renal function Catabolism and malnutrition Inflammation/ Atherosclerosis

13
Dialyzer length Pressure positive TMP negative Pressure Blood Dialysate Blood

14
Definitions EfficiencyKoA (ml/min) High< 500 Moderate500 – 700 Low> 700 KoA; Mass transfer area coefficient (maximum theoretical Cl at infinite BFR, DFR)
 High< 500 Moderate500 – 700 Low> 700 KoA; Mass transfer area coefficient (maximum theoretical Cl at infinite BFR, DFR)")
15
Kuf; Ultrafiltration coefficient Definitions Flux Kuf (ml/h/mmHg) High< 10 Low> 20 Permeability β 2 -microglobulin clearance (ml/min) High< 10 Low> 20
 High< 10 Low> 20 Permeability β 2 -microglobulin clearance (ml/min) High< 10 Low> 20")
16
Definitions Super-flux; Pressure drop Pore size Homogenous pores High performance; High flux Biocompatible Super-flux; Pressure drop Pore size Homogenous pores High performance; High flux Biocompatible

17
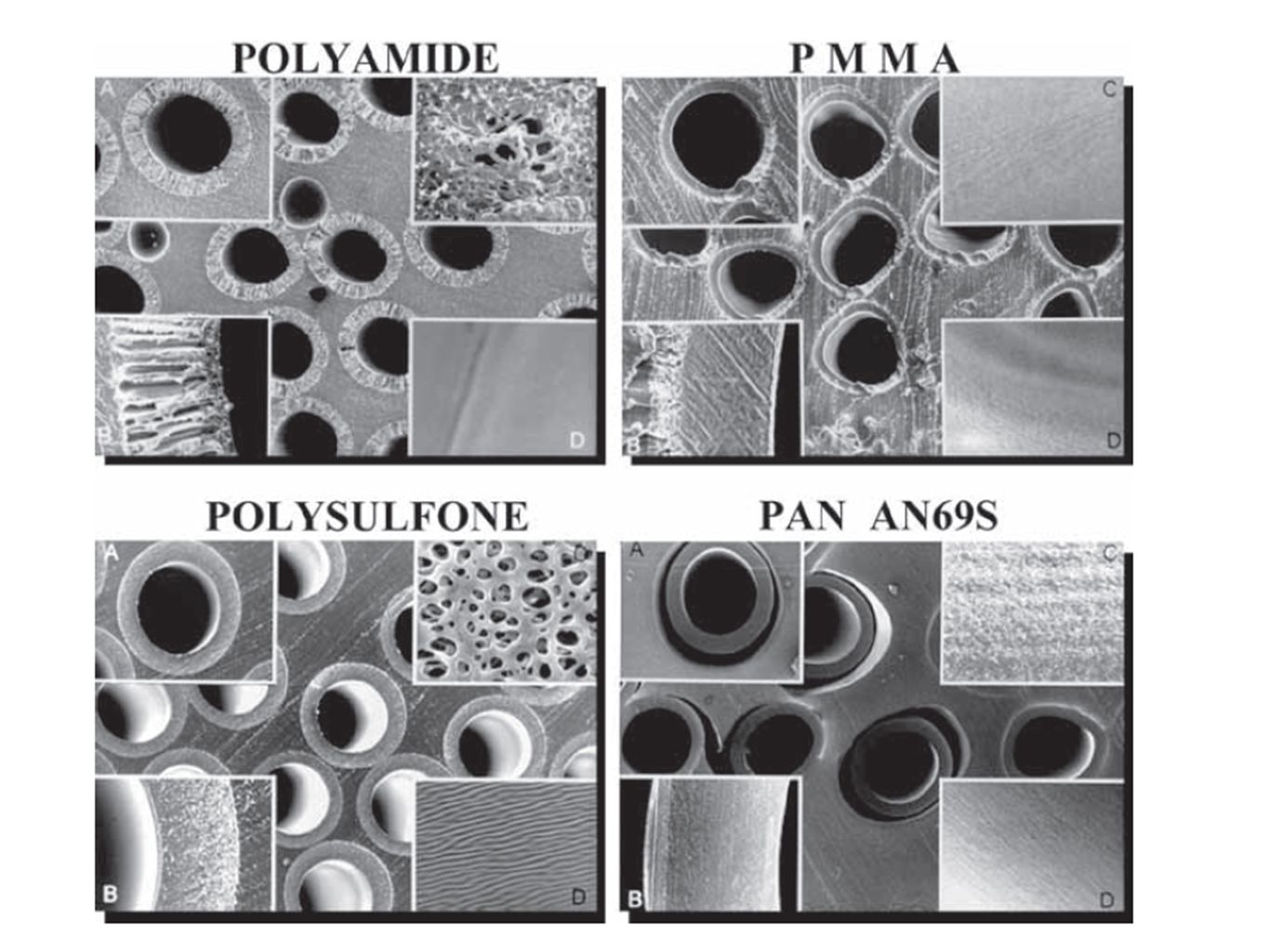
Type of membrane Unmodified cellulose Substituted cellulose Cellulosynthetic membrane Synthetic membrane

18
Substituted Cellulose Cuprophan - Good for small solutes - Bioincompatible - Low flux Cuprophan - Good for small solutes - Bioincompatible - Low flux Unmodified Cellulose Cellulose acetate/diacetate - Low / middle Kuf Cellulose triacetate - Middle / high Kuf - More biocompatible Cellulose acetate/diacetate - Low / middle Kuf Cellulose triacetate - Middle / high Kuf - More biocompatible

20
Synthetic membrane Cellulose membrane

21
LF-BILF-BC cell LF-BC syn HF- cell HF- syn Low complement activation -++ +++ Reflect dialysate impurities --++- Adsorption--+/--+ MM removal---++

22
RR 0.96, p = 0.53 single-pool Kt/V 1.32 vs 1.71 HEMO study group. N Engl J Med. 2002;347(25):2010-9. Standard High dose
: Standard High dose.")
23
HEMO study group. N Engl J Med. 2002;347(25):2010-9. RR 0.92, P = 0.23 C β2 microglobulin 3 vs 34 ml/min RR 0.68, pt on HD > 3.7 years Low flux High flux

24
< 27.5 mg/L Predialysis serum β 2 M (mg/L) HEMO study group. J Am Soc Nephrol 17: 546–555, 2006. Serum β-2 M Levels Predict Mortality 50 Relative risk

25
Diabetic patients, p = 0.039 Alb ≤ 4 g/dl, p = 0.032 Diabetic patients, p = 0.039 Alb ≤ 4 g/dl, p = 0.032 Survival probability of patients High-flux membrane Low-flux membrane No. at risk High-flux 83 67 55 46 27 14 7 3 Low-flux 74 59 40 29 19 11 3 0 0 12 24 36 48 60 72 84 Months Membrane Permeability Outcome (MPO) Study Locatelli F, et al. J ASN; 20: 645–54, 2009
 Study Locatelli F, et al. J ASN; 20: 645–54,")
26
EGE Study group. J Am Soc Nephrol 24: 1014–23, 2013 cardiovascular event-free survival HR 0.73 P = 0.12 AVF group; HR 0.61, p = 0.03 DM group; HR 0.49, p = 0.03 AVF group; HR 0.61, p = 0.03 DM group; HR 0.49, p = 0.03 p = 0.03 Hi Flux / Ultrapure

27
Conclusion RCTs.. no difference in mortality Suggestion; synthetic high flux membrane - Duration > 3.7 yr, DM, Alb ≤ 4 g/dl, AVF Highest survival..high flux + ultrapure AKI (KDIGO 2012)…Biocompatible
…Biocompatible.")
28
Thank you! Contact Address: Prof. Somchai Doe Tel: Email: www.kku.ac.th

Similar presentations














.>")




