Download presentation
Presentation is loading. Please wait.

1
Detection of Effort and Malingering: State of the Art Jason Gravano, M.S. 6/30/14

2
Speaking euphemistically? ‘‘cognitive effort,’’ ‘‘mental effort,’’ ‘‘insufficient effort,’’ ‘‘poor effort,’’ ‘‘invalid effort,’’ or even ‘‘faked effort.’’ response bias, disingenuous, dissimulation, non-credible, malingered, or non- or sub-optimal effort Bigler, 2012

3
Outline Introduction to Symptom Validity testing Definitional Issues Assumptions Measures of cognitive “Effort” Measures of validity on self report “Diagnosing” malingering

4
Validity of the Evaluation: the crux of the issue? We do not measure cognition or symptoms directly, rather the behavioral output of cognition (test scores, performances, self reports etc.) NP tests require the participant's best effort/cooperation for our inferences about their cognition to be valid Likewise, self-report of symptoms may not be taken at face value Thus, in instances where the evaluation informs clinical or legal decision making (arguably, all cases), validity checks become necessary Bigler, 2012
 NP tests require the participant s best effort/cooperation for our inferences about their cognition to be valid Likewise, self-report of symptoms may not be taken at face value Thus, in instances where the evaluation informs clinical or legal decision making (arguably, all cases), validity checks become necessary Bigler,")
5
Validity of the Evaluation: the crux of the issue? Especially because research has shown repeatedly that experienced experts are inaccurate in identifying valid versus invalid ability performances from mere observation of behavior or test scores E.g.: Ekman, O’Sullivan, & Frank, 1999 Faust, 1995 Faust, Hart, Guilmette, & Arkes, 1988 AACN 2010

6
Symptom Validity Testing: Methods and instruments designed to detect exaggeration or fabrication of neuropsychological dysfunction, as well as somatic and psychological symptom complaints. AACN 2010

7
Detection Symptom validity tests “effort measures” Any measure that is normally performed (and in some cases, perfectly performed) by a wide range of patients who have bona fide neurologic, psychiatric, or developmental problems Have to try to perform poorly? Performance validity/Response validity Negative response bias AACN 2010

8
Keep it consistent, people. Invalid performances/report should manifest as inconsistencies: In ability Consistency within a measure (hard vs. easy) Consistency within a cognitive domain Consistency within a battery Consistency between two or more testing sessions Consistency of NP results with real-world performances Consistency with expected profile of disorder (& severity) In self report of sys More on this later…
 Consistency within a cognitive domain Consistency within a battery Consistency between two or more testing sessions Consistency of NP results with real-world performances Consistency with expected profile of disorder (& severity) In self report of sys More on this later….")
9
“Effort” Measures …now with more political correctness!

10
Effort measures Typically rely on extremely low ceilings Measures that are so easy, “anyone can do them” Inference: If they don’t do well, they must not be “trying” If performance is poor, raises questions about the validity of your examination Can be used as supporting evidence for malingering, especially when performance is below chance

11
Effort measures Embedded measures (usually found after publication to have utility) Examples: CVLTii forced choice; Reliable Digit Span; WMS Faces; WCST “other categories”; TMT time. PROS- Face valid, don’t take extra time, relevant to the validity of the specific measure, hard(er) to coach Stand alone measures (designed purposefully for eval of effort) Examples: TOMM (Test of Memory Malingering); Word Memory test; Portland Digit) PROS- Created for this reason, likely better research base AACN 2010
 to coach Stand alone measures (designed purposefully for eval of effort) Examples: TOMM (Test of Memory Malingering); Word Memory test; Portland Digit) PROS- Created for this reason, likely better research base AACN")
12
Embedded measures can take advantage of floor effects: Use an alpha of.05 from a distribution of Severe TBI on a case of Mild TBI

13
Stand-alone cognitive effort tests Forced-choice Significantly below chance is direct evidence of deliberate underperformance “invalid performance can be identified using thresholds that are well above a level that is significantly below chance” Non-forced-choice evaluate random responding unrealistically slow or erroneous responding inconsistency of response patterns AACN 2010

14
Bimodal distribution? Cut Scores=/= chance performance Based on validation studies Bigler, 2012

15
Effort testing studies Rogers (2008) (a) simulation; (b) criterion groups (‘‘known’’ groups); (c) differential prevalence designs AACN 2010
 (a) simulation; (b) criterion groups (‘‘known’’ groups); (c) differential prevalence designs AACN 2010")
16
Differential prevalence design Assumes that response bias varies as a function of context (forensic, clinical, incentives offered, etc.) Useful in initial validation studies Lacks objective accuracy standards (base rates are not 100%) AACN 2010
 Useful in initial validation studies Lacks objective accuracy standards (base rates are not 100%) AACN 2010")
17
Simulation Random assignment of non-clinical participants to simulate or fake Control Often first, proof of concept studies Lacks generalizability AACN 2010

18
Criterion “known groups” Apriori criteria (often an “established” or “gold standard” measure + Slick criteria for malingering) to define groups Criteria chosen to have low false positive rate Occasionally take out individuals with “borderline” performance on the gold standard test……. So how does it perform across the board? AACN 2010

19
Issues Bigler (2012) raises about SVT research: Most SVT studies do not have IRB approval No Systematic Study Lesion/Localization Studies of SVT performance Implication: there may be some lesions that disrupt SVT performance Neurogenic drive & motivation problems? Psychological/Psychiatric factors may influence SVT performance Cut scores will misclassify Is type 1 or type 2 error worse? Is the entire eval invalid? Bigler, 2012

20
Resources for effort measures & embedded validity measures Sweet, 2009 Boone, 2007; Hom & Denney, 2002; Larrabee, 2007 Vickery, Berry, Inman, Harris, & Orey, 2001 Babikian, Boone, Lu, & Arnold, 2006; Heinly, Greve, Bianchini, Love, & Brennan, 2005; Iverson & Tulsky, 2003 + the other readings from this week AACN 2010

21
Consensus Recs: Effort Use tools designed (or re-designed) to detect sub-optimal effort Use both stand alone and embedded measures Use multiple measures, across the eval to account for varying effort Encourage optimal effort (through rapport)? Make sure the normative samples are appropriate Not all effort measures are created equal. Do some homework to see which ones perform best with your population.

22
Symptom Reporting

23
Self-Report Disorder-specific inventories; symptom inventories E.g., ptsd, depression, etc. When evaluating the validity of self-report, if possible, clinicians include measures that possess an internal means of assessing response bias. In general, disorder-specific inventories and symptom checklists that do not contain effective means for determining response bias and possible response invalidity should not be used in isolation. AACN 2010

24
Self-Report General personality inventories Strong validity research & design Keep up with research, appropriate populations Don’t “interpret” clinical scales when validity is at issue Be conservative in assuming intentionality (without supporting evidence) AACN 2010
 AACN 2010")
25
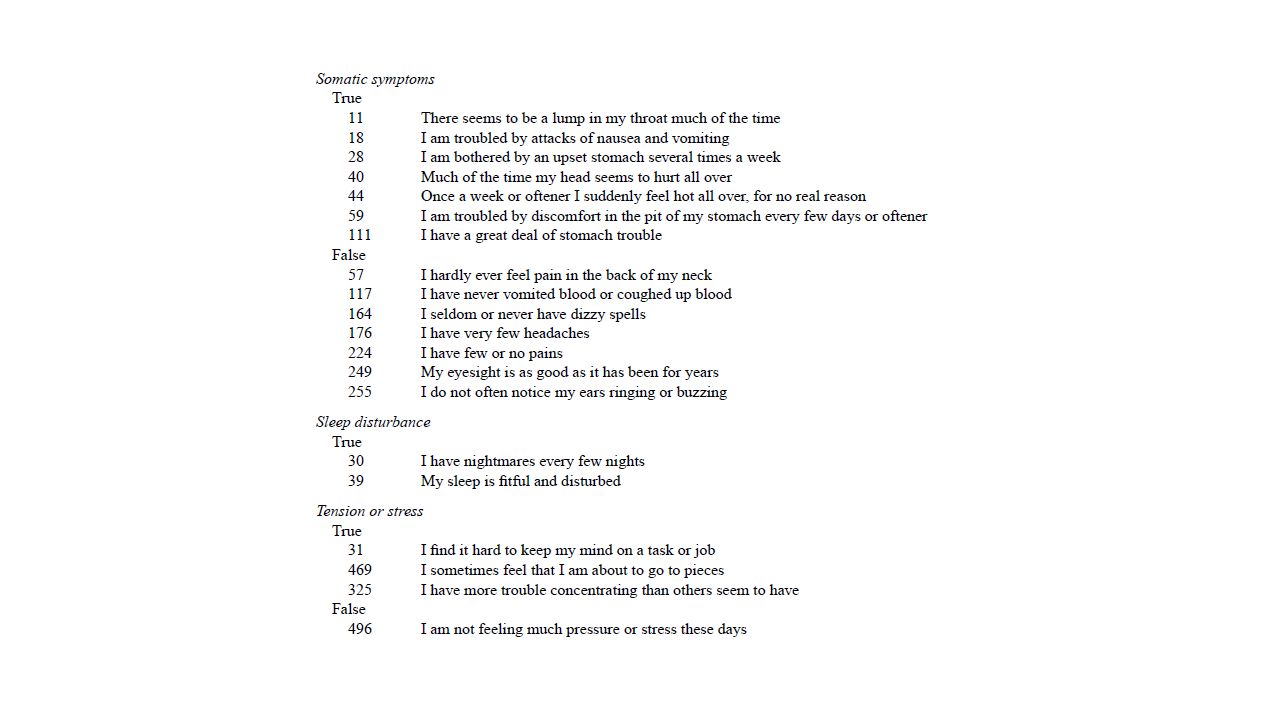
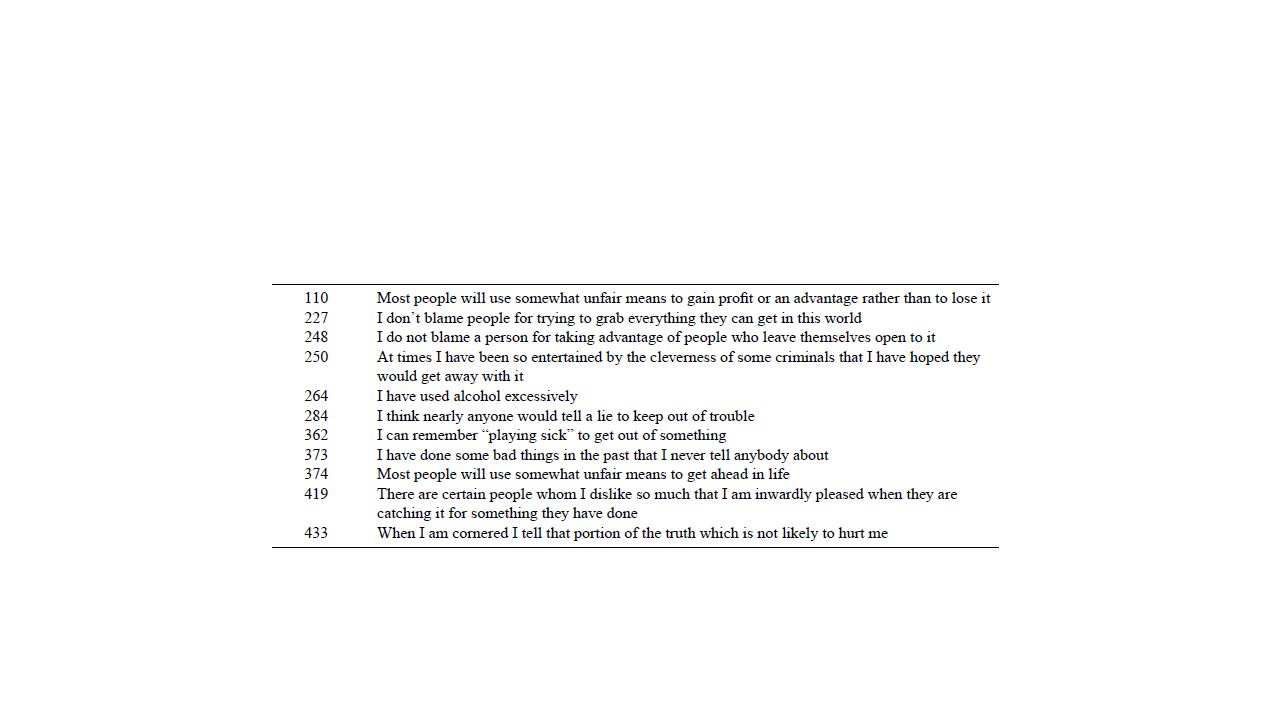
Review: Validity Scales on the MMPI-2 Traditional validity scales L – “Lie” present favorably F- “Faking good or Faking Bad” K – “defensiveness” Fb- Infrequent items at the end of the test; Random responding at the end of the exam? VRIN- Consistency TRIN- Consistency Other Infrequency Psychopathology scale (Fp; Arbisi & Ben-Porath, 1995) F-K (Gough, 1950) Obvious minus Subtle Scale (O-S; Greene, 1991; Wiener, 1948) Dissimulation scale (Gough,c1954, 1957) for the MMPI-2 (Ds2; Dsr2)
 F-K (Gough, 1950) Obvious minus Subtle Scale (O-S; Greene, 1991; Wiener, 1948) Dissimulation scale (Gough,c1954, 1957) for the MMPI-2 (Ds2; Dsr2).")
26
MMPI-2 Other, newer scales that may be important: FBS-r on MMPI-2-rf RBS- Response Bias Scale- predict insufficient effort on neuropsychological evaluation (Gervais et al., 2007a) HHI- Henry Heilbronner Index- exaggeration of somatic or ‘‘pseudoneurological’’ symptoms (Henry et al., 2006, 2008).
 HHI- Henry Heilbronner Index- exaggeration of somatic or ‘‘pseudoneurological’’ symptoms (Henry et al., 2006, 2008).")
27
Butcher 2003 on FBS Originally termed “Fake Bad Scale” The FBS was developed by identifying items rationally on a content basis utilizing unpublished frequency counts of malingerers’ MMPI responses and the authors’ subjective observations of personal injury (Lees- Haley et al., 1991). Item pool contains 43 items that include somatic symptoms, unusual beliefs, and deviant attitudes. Scores for the FBS were then compared between 20 personal injury claimants who appeared “notably credible,” A group of 25 personal injury claimants who appeared clearly to be malingering 16 medical outpatients asked to simulate emotional distress caused by a motor vehicle accident, 15 medical outpatients asked to simulate emotional distress caused by a toxic exposure, 36 medical outpatients asked to simulate emotional distress caused by stress on the job (Lees-Haley et al., 1991).
..")
28
FBS The cumulative FBS literature suggests that the scale continues to differentiate groups (“malingerers” or “over reporters” vs. valid) as well as, and under certain conditions superior to, other MMPI-2 validity scales (including all of the F-family scales). In particular, two factors that are particularly relevant to practicing neuropsychologists, effort status and TBI, substantially moderated FBS magnitudes. Nelson, 2010
 as well as, and under certain conditions superior to, other MMPI-2 validity scales (including all of the F-family scales). In particular, two factors that are particularly relevant to practicing neuropsychologists, effort status and TBI, substantially moderated FBS magnitudes. Nelson,")
31
FBS Early criticisms of FBS The basis for assigning individuals to the notably credible group and the malingered group was not explained. Original norming was questionable (private practice) No T scores, just mean data Cutoffs were not intended for mental health arenas FBS may not measure a single dimension Items contained on the FBS are generally not those that are rare or infrequently endorsed Low cross over with other validity scales FBS does correlate with psychopathology… Gender specific cutoffs? Butcher 2003
 No T scores, just mean data Cutoffs were not intended for mental health arenas FBS may not measure a single dimension Items contained on the FBS are generally not those that are rare or infrequently endorsed Low cross over with other validity scales FBS does correlate with psychopathology… Gender specific cutoffs. Butcher")
35
Psychological/Somatic Inference: Symptom exaggeration, symptom promotion, fabrication Evaluation: In depth diagnostic eval Onset, course, symptom picture, comorbidities, treatment efforts, response to treatment Inconsistent, contradictory data noted & Documented AACN 2010

36
Onset What is the typical age of onset When was the first symptom (e.g., after the arrest?) Personal history (abuse, neglect, etc.) Family history AACN 2010
 Personal history (abuse, neglect, etc.) Family history AACN 2010")
37
Symptom Presentation Keep an eye out for atypical symptoms Layman’s understanding of the disorder Atypical combo of symptoms **Distinct clinical presentations and/or prevalence of psychopathology may differ among some cultures and ethnic groups (Draguns & Tanaka-Matsumi, 2003). AACN 2010

38
Course Consistency of symptoms Expected trajectory AACN 2010

39
Response to Treatment Have they responded to treatment? Why or why not? When? Prior to litigation/compensation? AACN 2010

40
Consensus Recs: Symptom Reporting Use self reports with validity measurements Make sure the normative samples are appropriate Evaluate ability and disorder response bias separately

41
Malingering

42
In considering the diagnosis of malingering, the clinician is explicitly making a determination of intent: more specifically, a determination of intentionally exaggerated symptoms and/or intentionally diminished capability with the goal of obtaining an external reward. To do this: the context of the evaluation overall presentation of the examinee background information history information gathered during interview observations, neuropsychological tests, and measures of response bias AACN 2010

43
Effort Malingering Failed Effort measure =/= malingering, just as passing one =/= not malingering Assessing effort is one dimension of the evaluation of Malingering equating ‘‘poor effort’’ with malingering is an oversimplification It takes effort to fake! The process of detecting malingering is one in which consideration is given to multiple dimensions of behavior that differentiate malingering from other entities factitious disorder conversion disorder cogniform disorder somatoform disorder. AACN 2010

44
Diagnostic classifications for Malingering DSM NP operationalized systems Bianchini et al., 2005 Slick, Sherman, & Iverson, 1999 Reliable classification indices; operationalized Guidelines recommend incorporation of multiple sources of data/information: AACN Practice Guidelines for Neuropsychological Assessment and Consultation; AACN, 2007 Specialty Guidelines for Forensic Psychologists; Committee on Ethical Guidelines for Forensic Psychologists, 1991 AACN 2010

45
“Diagnosing” malingering Context of the evaluation Clinical vs. forensic Gain, secondary gain, external gain, financial gain ***MUST HAVE SOMETHING TO GAIN*** Necessary, but far from sufficient Examples: financial reward, compensated time away from work, avoidance of military duty, relief from legal consequences, and obtaining medications/narcotics AACN 2010

46
Assessing intent? The best way to assess intent is by ruling out other possible conditions (e.g., psychological, neurological, developmental) that might otherwise explain the suspicious behavioral presentation and by requiring the presence of multiple improbable performances and/or atypical symptomatic complaints. The differential diagnosis of malingering is a clinical process that: (1) requires careful analysis on the part of the examiner, (2) is based on objective criteria; (3) incorporates indicators that have established classification accuracy, (4) combines clinical judgment with the results of scientifically validated measures in this process. AACN 2010
 that might otherwise explain the suspicious behavioral presentation and by requiring the presence of multiple improbable performances and/or atypical symptomatic complaints. The differential diagnosis of malingering is a clinical process that: (1) requires careful analysis on the part of the examiner, (2) is based on objective criteria; (3) incorporates indicators that have established classification accuracy, (4) combines clinical judgment with the results of scientifically validated measures in this process. AACN")
47
The possibility of malingering (1) disparity between real-world observations and either test performance or self-report, (2) inconsistency between type or severity of injury and test performances, (3) inconsistency between an individual’s behavior when he/she is aware of being evaluated versus when not aware of not being evaluated, and (4) inconsistency across serial testings that cannot be explained by an underlying neurological process or known psychiatric condition. AACN 2010

48
The assessment (1) review of records; (2) psychosocial history obtained by interviewing; (3) observations of the claimant’s behavior during the assessment period; (4) consideration of information from collateral sources, such as significant others, employers, etc., when available and appropriate; (5) formal psychological/neuropsychological testing; (6) response validity assessment procedures; and (7) surveillance video/audio, when available. ‘‘Does what I am learning about this claimant make sense in light of the putative claim, the diagnosis, history and totality of the presentation?’’ AACN 2010

49
Unlike psychometric indicators of invalid performance, objective standards for the evaluation of inconsistencies between the clinical presentation and evidence of capacities outside the clinical setting may not exist. In the absence of such standards, a determination that an inconsistency indicates invalidity should be cautious and conservative and in some cases may be left to the trier-of-fact. AACN 2010

50
Consensus Recs: Malingering Consider & investigate “real world” performance Be aware of potential litigation cases Be aware of discrepancy between test results and known-group performances Evidence for/against malingering should be considered incrementally

51
Consensus recs: Practice List SVIs in reports, but be cautious of test security Consider serial evaluations to discriminate unrealistic performances (e.g., lack of practice effects) Use collateral informants (when appropriate) Don’t rely on the manuals and cut scores: use up-to-date research AACN 2010
 Use collateral informants (when appropriate) Don’t rely on the manuals and cut scores: use up-to-date research AACN 2010")
52
Questions for the Class! If you see invalid performance in testing, how should you address it? Could we use and interpret effort measures in looking at intentional disorders (e.g., subcortical disorders)? What do you do if you suspect there is genuine neurological disorder & malingering?
. What do you do if you suspect there is genuine neurological disorder & malingering .")
53
Consensus recs: Research How to interpret multiple effort measurements Populations that “fail” effort measures despite effort Deliberate intent to feign Future ability tests should have validity indicators Pediatric samples? Rule out or rule in? AACN 2010

54
The end

Similar presentations