Download presentation
Presentation is loading. Please wait.

1
YAY! Its potassium!

2
Why is it important Major intracellular ion (98%) Major determinant of resting membrane potential. (arrhythmia’s etc) Long term = kidneys Short term = intra-extra movement (serum K+ doesn’t reflect total Its distrabution is affected by many factors
 Long term = kidneys Short term = intra-extra movement (serum K+ doesn’t reflect total Its distrabution is affected by many factors.")
3
In the Kidney 60-80% is passively reabsorbed in the PCT LOH 10-30% reabsorbed DCT and collecting duct SECRETION IS CONTROLLED HERE!!!! Aldosterone controls the amount secreted back into the collecting tubule to be excreted! Normally around 95% is secreted back into the tubule.

4
RAAS

5
2K+ Na/K ATPase 3Na+ Renal interstitial fluid (reabsorbed into blood) Tubular lumen (urine) Na2+ into cell K+ out ENaC 1)Aldosterone increases ENaC Channel expresion. More sodium is reabsorbed from the tubular lumen 2) Sodium is transported across the membrane in exchange for potassium 3) Potassium exits the cell and enters the tubular lumen by osmosis through channel proteins. ALDOSTERONE EFFECT In the KIDNEY
 Sodium is transported across the membrane in exchange for potassium 3) Potassium exits the cell and enters the tubular lumen by osmosis through channel proteins. ALDOSTERONE EFFECT In the KIDNEY.")
6
Things that move K+ into cells decreasing blood potassium concentration) Insulin Aldosterone B adrenergic stimulation Alkalosis Tubular flow rate Ahh but how?
 Insulin Aldosterone B adrenergic stimulation Alkalosis Tubular flow rate Ahh but how")
7
Insulin and B adrenergic effects Insulin activates sodium-potassium ATPases in many cells, causing a flux of potassium into cells. Under certain circumstances, injection of insulin can kill patients because of its ability to acutely suppress plasma potassium concentrations. Ingested K + is absorbed rapidly and enters the portal circulation, where it stimulates insulin secretion. Insulin increases Na +,K + -ATPase activity and facilitates potassium entry into cells, thereby averting hyperkalemia. β 2 -Adrenergic stimulation also promotes entry of K + into cells through increased cyclic adenosine monophosphate (cAMP) activation of Na +,K + -ATPase.
 activation of Na +,K + -ATPase..")
8
2K+ Na/K ATPase 3Na+ Insulin Increases the activity ok Na+ K+ ATPase. Reducing serum K+. Insulin overdose can cause hypokalaemia! B2 adrenergic activation Increases cAMP which in turn increases Na+K+ATPase. Im a normal cell!!!

9
Cell lysis (K+ is the main intracellular ion!) Hypoaldosteronism (ADDISONS DISEASE) Acidosis Decreased insulin Increased fluid osmolarity (dehydrates the cell causing K+ to leave to regain balance) Things that move K+ out cells (increasing blood potassium concentration)
 Hypoaldosteronism (ADDISONS DISEASE) Acidosis Decreased insulin Increased fluid osmolarity (dehydrates the cell causing K+ to leave to regain balance) Things that move K+ out cells (increasing blood potassium concentration)")
10
ACIDOSIS Renal interstitial fluid (reabsorbed into blood) Tubular lumen (urine) H+ K+ HCO3 Cl- High H+ concentration causes H+ to be secreted into the tubular lumen in exchange for potassium. This increases potassium reabsorption and increases its serum concentration. ALSO decreases H+ K+ATPase activity

12
HYPOKALAEMIA below 3.5 mmol/L (refers to extracellular concentration, not total!) Symptoms = symptomless until under 2.5mmol/L. Can cause arrhythmias as it lowers the action potential threshold. causes = Alkalosis, insulin excess, B adrenercic activity, diarrhoea, renal disease. Treatment = bananas, infuse potassium, STOP diuretics.

14
HYPERKALAEMIA More than 5.3mmol/L Symptoms = muscle weakness, palpitations, arrhythmias. Causes = Acidosis, NSAIDS, Insulin deficiency, cell lysis, hypoaldosteronism, ACE inhibiters, CKD. Treatment = Calcium gluconate (stabalises myocardium. Insulin (pushes it into cells) (give dextrose at the same time) Salbutamol Fluids and dialysis.
 (give dextrose at the same time) Salbutamol Fluids and dialysis..")
15
Some questions for you. Are these referring to hyper or Hypokalaemia * Can be caused by ACE inhibiters * Can be caused by alkalosis * Can be caused by B adrenergic activity * Can be caused by cell lysis, * Can be caused by diarrhea * Can be caused by hypoaldosteronism * Can be caused by INSULIN DEFICIENCY * Can be caused by insulin excess * Can be caused by NSAIDs * Can be treated with Bananas (high potassium diet) * Can be treated with Calcium Gluconate * Can be treated with Insulin (what should you give with it) * Can be treated with Salbutamol * Can cause arrhythmias
 * Can be treated with Calcium Gluconate * Can be treated with Insulin (what should you give with it) * Can be treated with Salbutamol * Can cause arrhythmias.")
16
Answers Can be caused by ACE inhibiters Hyperkalaemia Can be caused by alkalosis Hypokalaemia Can be caused by B adrenergic activity Hypokalaemia Can be caused by cell lysis, Hyperkalaemia Can be caused by diarrhea Hypokalaemia Can be caused by hypoaldosteronism Hyperkalaemia Can be caused by INSULIN DEFICIENCY Hyperkalaemia Can be caused by insulin excess Hypokalaemia Can be caused by NSAIDs Hyperkalaemia Can be treated with Bananas (high potassium diet) Hypokalaemia Can be treated with Calcium Gluconate Hyperkalaemia Can be treated with Insulin (what should you give with it) Hyperkalaemia IM dextrose to avoid hypoglycemia (cant IM glucose) Can be treated with Salbutamol Hyperkalaemia Can cause arrhythmias Hypokalaemia Hyperkalaemia
 Hypokalaemia Can be treated with Calcium Gluconate Hyperkalaemia Can be treated with Insulin (what should you give with it) Hyperkalaemia IM dextrose to avoid hypoglycemia (cant IM glucose) Can be treated with Salbutamol Hyperkalaemia Can cause arrhythmias Hypokalaemia Hyperkalaemia")
18
Juxtaglomerular apparatus is the part of the nephron where the distal tubule is closely associated with the glomerulus At this point the distal tubule has special cells called macula densa cells These sense NaCl concentration in the filtrate Low BP, then low NaCl in the filtrate Macula densa cells signal to the juxtaglomerular (granular) cells of the afferent arteriole to make them release RENIN
 cells of the afferent arteriole to make them release RENIN")
19
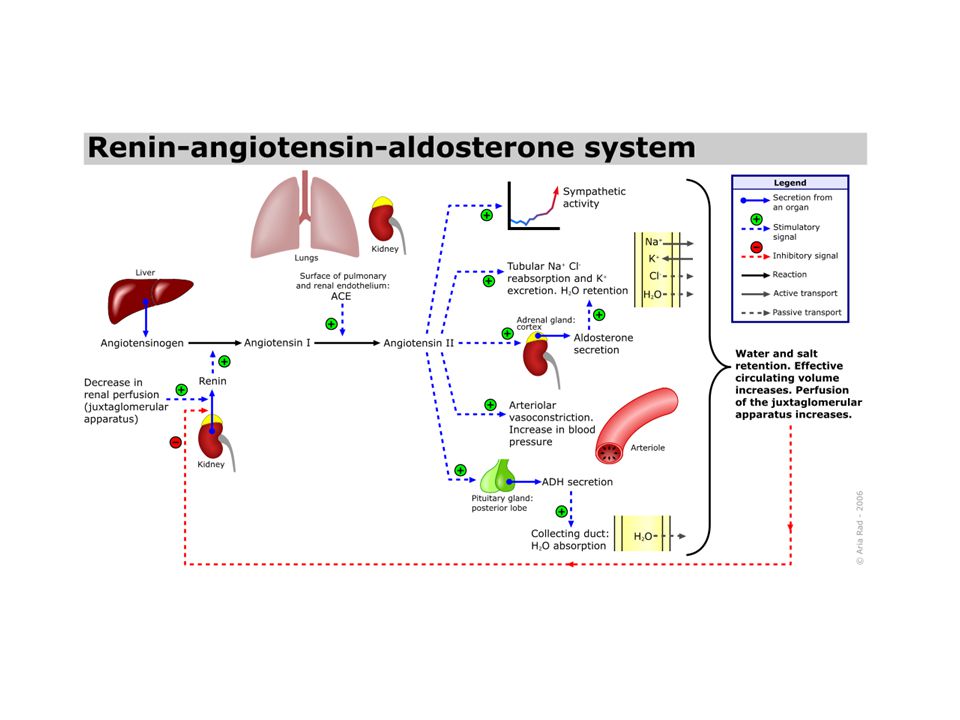
RENIN AngiotensinogenAngiotensin 1 Angiotensin 2 Angiotensin converting enzyme (ACE) Aldosterone release (adrenals) Vasoconstriction Thirst ADH release Renin is an enzyme Catalyses angiotensinogen to Ang 1 ACE found mainly in lungs but also the kidney Catalyses Ang 1 to Ang 2 Ang 2 has the main effects for increasing blood pressure ACE also catalyses breakdown of bradykinin in the lungs Some patients on ACEi may find they develop a cough because bradykinin isn’t broken down Expression of aquaporins in the collecting duct – reabsorption of water
 Aldosterone release (adrenals) Vasoconstriction Thirst ADH release Renin is an enzyme Catalyses angiotensinogen to Ang 1 ACE found mainly in lungs but also the kidney Catalyses Ang 1 to Ang 2 Ang 2 has the main effects for increasing blood pressure ACE also catalyses breakdown of bradykinin in the lungs Some patients on ACEi may find they develop a cough because bradykinin isn’t broken down Expression of aquaporins in the collecting duct – reabsorption of water")
22
Juxtaglomerular apparatus is the part of the nephron where the distal tubule is closely associated with the glomerulus At this point the distal tubule has special cells called macula densa cells These sense NaCl concentration in the filtrate Low BP, then low NaCl in the filtrate Macula densa cells signal to the juxtaglomerular (granular) cells of the afferent arteriole to make them release RENIN
 cells of the afferent arteriole to make them release RENIN")
23
RENIN AngiotensinogenAngiotensin 1 Angiotensin 2 Angiotensin converting enzyme (ACE) Aldosterone release (adrenals) Vasoconstriction Thirst ADH release Renin is an enzyme Catalyses angiotensinogen to Ang 1 ACE found mainly in lungs but also the kidney Catalyses Ang 1 to Ang 2 Ang 2 has the main effects for increasing blood pressure ACE also catalyses breakdown of bradykinin in the lungs Some patients on ACEi may find they develop a cough because bradykinin isn’t broken down Expression of aquaporins in the collecting duct – reabsorption of water
 Aldosterone release (adrenals) Vasoconstriction Thirst ADH release Renin is an enzyme Catalyses angiotensinogen to Ang 1 ACE found mainly in lungs but also the kidney Catalyses Ang 1 to Ang 2 Ang 2 has the main effects for increasing blood pressure ACE also catalyses breakdown of bradykinin in the lungs Some patients on ACEi may find they develop a cough because bradykinin isn’t broken down Expression of aquaporins in the collecting duct – reabsorption of water")
Similar presentations













 Newborn (77%) Adult male (60%) Adult female (54%) Elderly (45%) Adipose.>")






. Other excretory.>")
 response How the anterior and posterior pituitary.>")

 System>")
