Download presentation
Presentation is loading. Please wait.

1
Atopic Dermatitis, Eczema, and Noninfectious Immunodeficiency Disorders
Adam Wray, D.O. August 10, 2004

2
Atopic Dermatitis Aka atopic eczema Aka infantile eczema
Aka flexural eczema Aka disseminated neurodermatitis Aka prurigo diathsique

3
Atopic Dermatitis Pruritis is the hallmark of AD “Itch that rashes”
Eczematous eruption leads to lichenified dermatitis Itching precedes the appearance of lesions

4
Atopic Dermatitis High level of IgE antibodies to House dust mites
IgE bound to Langerhans cells in atopic skin Food exacerbates symptoms in some patients: eggs, peanuts, cow’s milk represent up to 75% of positive test.

5
Atopic Dermatitis Triggering Factors Temperature change Sweating
Excessive washing Contact with irritating substances (wool, soaps, detergents, cigarette smoke Contact allergy Aeroallergens Microbial agents Food Stress

7
AD – 3 Stages Infantile 2 months to 2 years Childhood
2 years to 10 years Adult adolescence to adulthood

8
Infantile Atopic Dermatitis
60% of AD present in the first year of life, after 2 months of age Begin as itchy erythema of the cheeks Distribution include scalp, neck, forehead, wrist, and extensors May desquamate leading to erythroderma. Buttocks and diaper area frequently spared

9
Infantile Atopic Dermatitis
Partial or even complete remission in summer and relapse in winter are the rule Worsening observed after immunizations and viral infections

10
Infantile Atopic Dermatitis
Most cases the symptoms will disappear toward the end of the second year. Egg, peanut, milk, wheat, fish, soy, and chicken may exacerbate infantile AD

11
Involvement of the cheeks is characteristic of the infantile pattern of AD.

12
Childhood Atopic Dermatitis
Characterized by less acute lesions Distribution: antecubital and popliteal fossae, flexor wrist, eyelids, and face. Severe atopic dermatitis involving more than 50% of body surface area is associated with growth retardation.

14
Adult Atopic Dermatitis
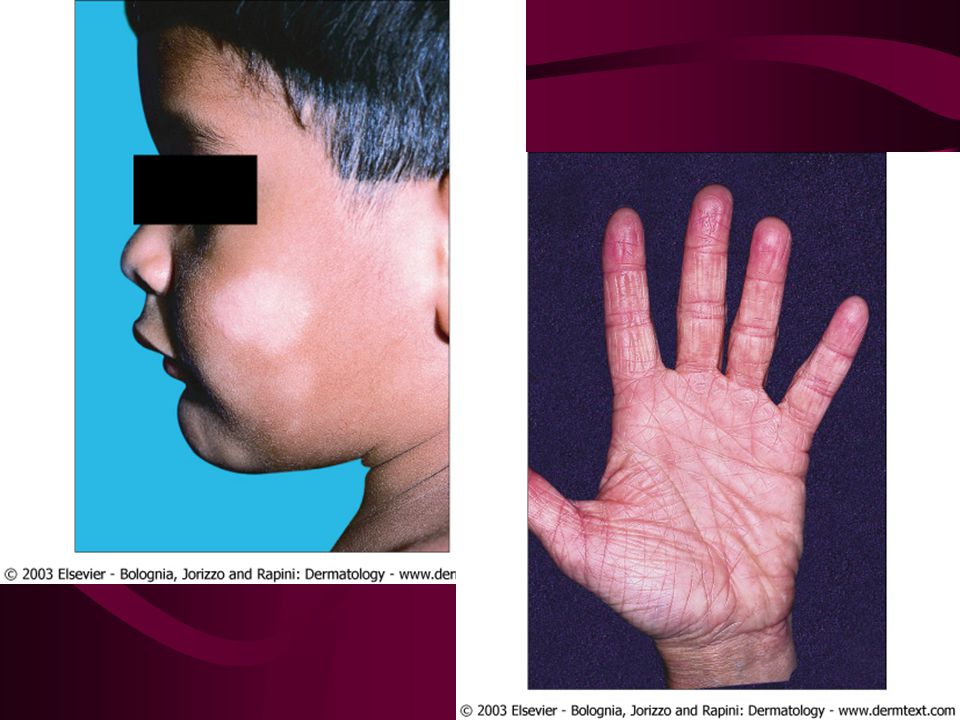
Distribution: antecubital and popliteal fossae, the front side of the neck, the forehead, and area around the eyes. Atopic individuals are at greater risk of developing hand dermatitis than are the rest of the population 70% develop hand dermatitis sometime in their lives Common in women after birth of their 1st child, when increased exposure to soaps and water trigger disease

16
Adult with atopic dermatitis that favors the face and neck

17
Cutaneous stigmata Dennie-Morgan fold Pityriasis alba
Keratosis pilaris Hertoghe’s sign – thinning of the lateral eyebrows Keratosis punctata palmaris et plantaris

18
Note the Dennie–Morgan lines and central facial pallor.

21
AD and Ichthysosis vulgaris
Up to 50% of AD will have Ichthysosis vulgaris Autosomal dominant Excessive scaling most prominent on shins White, translucent, quadrangular scales on the extensor aspects of the arms and legs common with atopy

22
Vascular Stigmata Headlight sign – perinasal and periorbital pallor
White dermographism – blanching of the skin at the site of stroking with a blunt instrument – cause edema and obscure color of underlying vessels.

23
Infection Staph aureus – 90% of chronic lesions
Eczema herpeticum – generalized herpes simplex infection. Young children usually. Secondary to reduced cell-mediated immunity Vaccination against smallpox is contraindicated in person with atopic dermatitis. Even when condition is in remission, widespread and even fatal vaccinia can occur.

24
Eczema herpeticum: typical vesicular lesions on the hand, around the eye, and on the face

25
Immunology T helper cell type 2 (Th2) dominance
Th2 produces IL-4, 5, and 10 IL-4 and IL-5 produce elevated IgE and eosinophilia IL-10 inhibits delayed type hypersensitivity Th2 may be sensitive to house mites or grass pollen

27
Immunology Monocytes produces elevated amount of prostaglandin E2 (PGE2) PGE2 reduces gamma-interferon production, but not IL-4 from helper cells thereby enhancing the Th2 dominance PGE2 also directly enhances IgE production from B cells

29
Immunology Langerhans cells of AD patient stimulate helper T cells into Th2 phenotype without the presence of antigen Langerhans cells have IgE bound to their suface receptors. These IgE are associated with atopic antigens, such as house dust mites

31
Differential Diagnosis
Seb Derm Contact dermatitis Nummular eczema Scabies Psoriasis

33
Histology Spongiotic dermatitis Lichen simplex chronicus
Eosinophiles may be seen

35
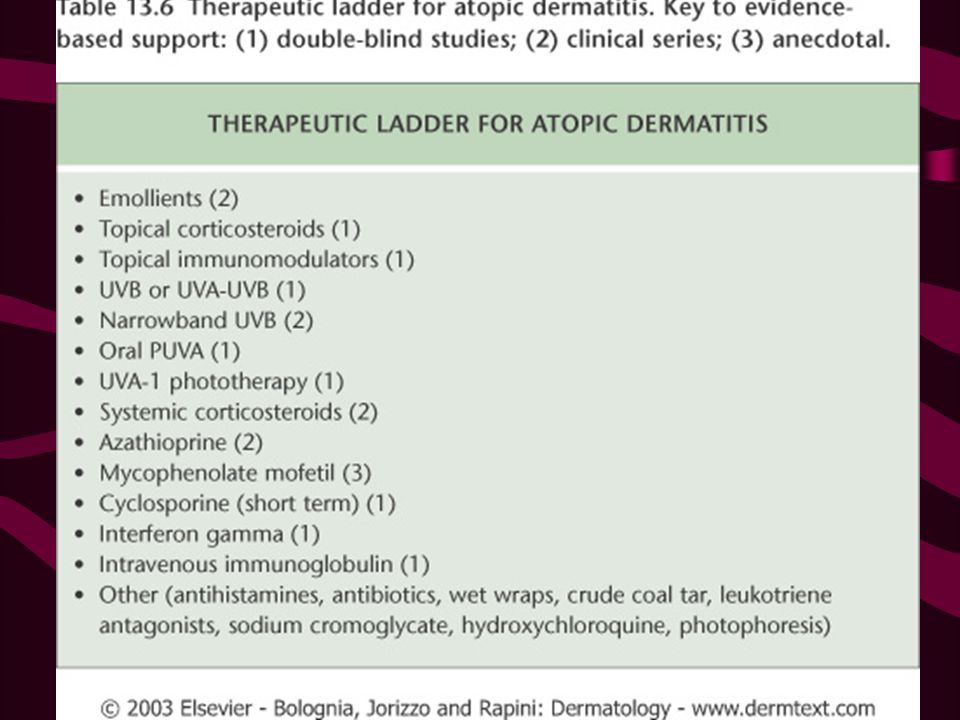
Management Protect from scratching
Adequate cleansing but not over bathing or rubbing Gentle cleanser Anti-histamines, especially at night Bathing protocol Food allergy identification and dietary restrictions. Hydrate skin daily with moisturizers

36
Management Topical steroid
Wet compress of Burow’s solution such as Domeboro. Crude coal tar/liquor corbonis detergens (LCD) PUVA Cyclosporine
 PUVA. Cyclosporine.")
37
Management “Topical FK506 (Tacrolimus) is dramatically beneficial in SEVERE atopic dermatitis” 95% showed good improvement in Alaiti and Rusicka study in JAAD 1998, Archive 1999

38
Elidel vs. Protopic Elidel good for mild cases
Elidel doesn’t cause initial increase pruritus Elidel good for “return eczema” Protopic good for severe cases Protopic can cause initial increase pruritus

40
Regional Eczema Ear eczema Eyelid dermatitis Nipple eczema Hand eczema
Diaper dermatitis Infectious eczematoid dermatitis Juvenile plantar dermatosis

41
Ear Eczema Most frequently caused by seborrheic or atopic dermatitis
Staph, Strep, or Psoeudomonas Earlobe is pathognomonic of nickel allergy

43
Eyelid dermatitis When on one eye only, it is most frequently caused by nail polish, and usually affects the upper eyelid When both eyes are involved, consider mascara, eye shadow, eyelash cement, eyeline, etc In contrast, atopic dermatitis affects both upper and lower eyelid.

44
Nipple eczema Painful fissuring, seen especially in nursing mothers
Maybe an isolated manifestation of atopic dermatitis If persist more than 3 months, and/or unilateral, biopsy is mandatory to rule out Paget’s

47
Hand eczema Spongiosis histologically
Irritant hand dermatitis- seen in homemakers, nurses. Resulting from excessive exposure to soaps Pompholyx- tapioca vesicles, on sides of fingers, palms, and soles Differentials – Bullous tinea, id, allergic contact dermatitis

48
Smoking as in palmoplantar pustulosis, may be a cofactor

50
Treatment Barrier Moisturizer Systemic Corticosteroids
Phototherapy – UVA, PUVA, Radiotherapy (Grenz Ray) New research suggests use of oral retinoids for severe recalcitrant hand eczema
 New research suggests use of oral retinoids for severe recalcitrant hand eczema.")
51
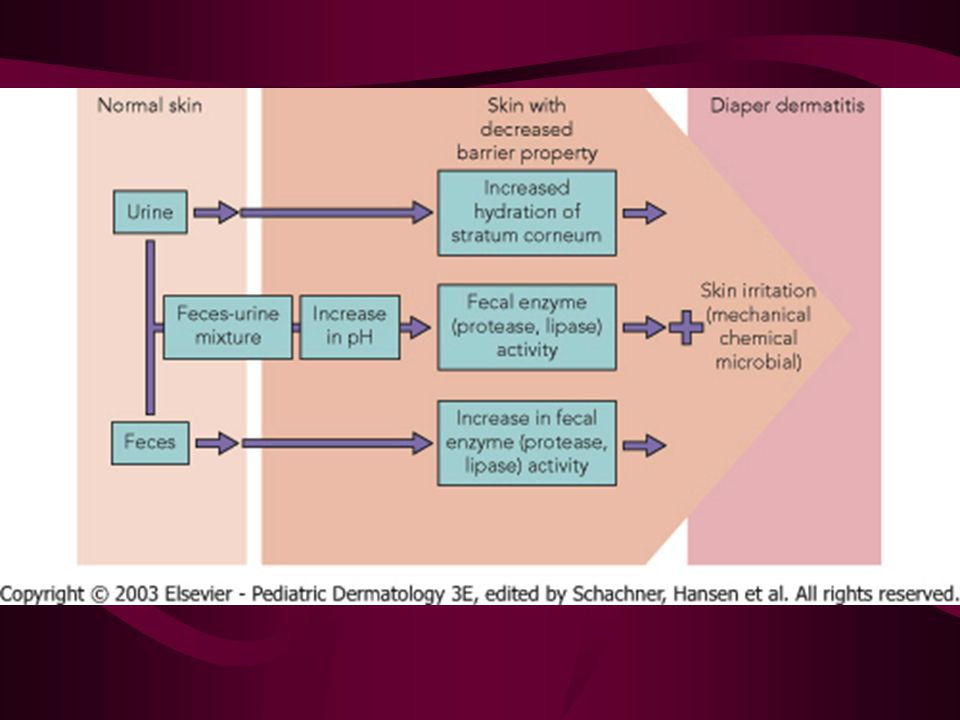
Diaper (Napkin) Dermatitis
Erythematous, papulovesicular dermatitis distributed over the lower abdomen, genitals, thighs, and the convex surfaces of the buttocks Irritation caused by bacteria, change in the environment (moisture, lower PH, feces) Candida albicans secondary infection.
 Candida albicans secondary infection.")
54
Diaper dermatitis - complications
Jacquet’s erosive diaper dermatitis Punched out ulcers/erosions with elevated borders Pseudoverrucous papule and nodules Granuloma gluteal infantum

55
Jacquet’s diaper dermatitis with eroded nodules on the labia

56
Granuloma gluteale infantum

57
Diaper Dermatitis Ddx: Napkin psoriasis, seborrheic dermatitis, atopic dermatitis, langerhans cell histiocytosis, tinea cruris, allergic contact dermatitis, acrodermatitis enteropathica, biotin deficiency, congenital syphillis Treatment: prevention

58
Juvenile plantar dermatosis
Begins as a patchy symmetrical, smooth, red, glazed macules on the base of the great toes Affect age 3 to puberty. Symmetrical lesions on weight bearing area “toxic sock syndrome” – caused by repeated maceration of the feet by occlusive shoes and nonabsorbent synthetic socks Virtually always resolve after puberty

59
Juvenile plantar dermatosis

61
Xerotic Eczema Aka winter itch, nummular eczema, eczema craquele, and asteototic eczema. Anterior shins, extensor arms, and flank Elderly person predisposed. Use of bath oils in bath water is recommended to prevent water loss Moisturizers – urea or lactic acid.

63
Hormone Induced Dermatoses
Autoimmune progesterone dermatitis – urticaria, urticarial paplues, papulovesicular lesion, or eythema multiforme. Appear 5-10 days before menses. Oophorectomy, danazol, and tamoxifen are treatment modalities Autoimmune estrogen dermatitis – a cyclic skin disorder with variable morphologies. Exacerbate premenstrually or occur only immediately before the menses. Treatment with tamoxifen maybe effective.

64
Immunodeficiency Syndromes
X-Linked Agammaglobulinemia Isolated IgA Deficiency Common Variable Immunodificiency Isolated Primary IgM Deficiency Immunodificiency with Hyper-IgM Thymic Hypoplasia Thymic Dysplasia with Normal Immunoglobulins (Nezelof Syndrome)
")
65
Immunodeficiency Syndromes
Purine Nucleoside Phosphorylase Deficiency Miscellaneous T-Cell Deficiencies Severe Combined Immunodeficiency Disease (SCID) Thymoma with Immunodeficiency Ataxia-Telangiectasia (Louis-Bar’s S.) Wiskott-Aldrich Syndrome
 Thymoma with Immunodeficiency. Ataxia-Telangiectasia (Louis-Bar’s S.) Wiskott-Aldrich Syndrome.")
66
Immunodeficiency Syndromes
X-Linked Lymphoproliferative Syndrome Chronic Granulomatous Disease Myeloperoxidase Deficiency Leukocyte Adhesion Molecule Deficiency Chediak-Higashi Syndrome Hyperimmunoglobulinemia E Syndrome Complement Deficiency Graft-Versus-Host Disease

67
X-Linked Agammaglobulinemia
Aka Bruton’s syndrome, sex-linked agammaglobulinemia. Appears after 3-6 month of life Frequent Strep and staph infection. Viral resistance intact. IgA, IgM, IgD, and IgE are absent in the serum. IgG present in small amount Cell-mediated immunity intact. T lymphocytes are normal, B cells are completely lacking

68
X-Linked Agammaglobulinemia
Defect lies in the maturation block in pre-B-cell to B-cell differentiation Protein tyrosine kinase (PTK) gene deletion and point mutation May develop leukemia, lymphoma, fatal encephalitis, pulmonary fibrosis Tx: gamma globulin
 gene deletion and point mutation. May develop leukemia, lymphoma, fatal encephalitis, pulmonary fibrosis. Tx: gamma globulin.")
69
Selective IgA Deficiency
Most common immunoglobulin deficiency Usually asymptomatic Clinical manifestations 10-15% Sinopulmonary bacterial infections Giardia gastroenteritis 1/3 with clinical disease develop autoimmune disorders SLE, Vitiligo, chronic mucocutaneous candidiasis, lipodystrophia centrifugalis abdominalis, ITP No sexual predilection

70
Isolated IgA Deficiency
Absence or marked reduction of serum IgA 1:600 in white population, most are entirely well. Malignancy is increased in adult with IgA deficiency.

71
Common Variable Immunodificiency
Aka acquired hypogammaglobulinemia HLA marker B8 and DR3 are affected Recurrent sinopulmonary infections B cells present but not terminally differentiated T cell dysfunction evident

72
Common Variable Immunodeficiency
Increased risk of autoimmune disorders Vitiligo, alopecia areata, vasculitis Increased incidence of lymphoma 400 fold increase risk in female patients

73
Leukocytoclastic vasculitis on the legs of a girl with common variable immunodeficiency . Autoimmune disorders show a significant increase in frequency.

74
Isolated Primary IgM Deficiency
Eczematous dermatitis presents in 1/5 of patients with this condition Predisposition to bacterial infection Defect in maturation of IgM producing plasma cell.

75
Immunodificiency with Hyper-IgM
Low or absent IgG, IgE, and IgA level. Normal or elevated IgM and IgD X-linked form caused by mutation or deletion of Xq region, which encodes a ligand of CD40, gp39 Gp39-CD40 interaction signals for Ig isotype switching. Tx: IVGG, and allogenic bone marrow transplant

76
Extensive, recalcitrant warts in an adult with hyperimmunoglobulinemia M syndrome.

77
Painful oral ulceration in a patient with hyperimmunoglobulinemia M syndrome

78
Thymic Hypoplasia DiGeorge anomaly, aka III and IV pharyngeal pouch syndrome Facies: notched and low-set ears, micrognathia, shorten philtrum, hypertelorism Congenital absence of the parathyroid, thymus, and abnormal aorta Hpocalcemia is the first sign Aortic and cardiac defects are the most common cause of death Deletions within proximal long arm of chromosone 22

79
Noninfectious, persistant cutaneous granulomas in a patient with DiGeorge Syndrome. The granulomas are indistinguishable clinically from cutaneous granulomas associated with other immunodeficiencies.

80
Thymic Dysplasia with Normal Immunoglobulins (Nezelof Syndrome)
Faulty development of thymus gland Autosomal recessive Thymus is present but underdeveloped; no cardiac abnormalities Contrast to DiGeorge syndrome

81
Purine Nucleoside Phosphorylase Deficiency
Greatly reduced T-Cell counts, depressed cell mediated immunity B cells and antibody formation intact Mutation on 14q13 Usually died of overwhelming viral infection

82
Miscellaneous T-Cell Deficiencies
Cartilage-hair hypoplasia syndrome AR, patient with short-limbed dwarfism, fine sparse, hypopigmented hair, defective cell mediated immunity. Most common in Amish and Finns May have “doughy” skin secondary to degenerated elastic tissue Increased risk of non-Hodgkin’s lymphoma and basal cell carcinomas

83
Miscellaneous T-Cell Deficiencies
Omenn’s syndrome AR Mimics GVHD exfoliative erythroderma, eosinophilia, recurrent infection, hypogammaglobulinema, diarrhea, hepatosplenomegly, alopecia Early death by 6 months Inefficient and abnormal generation of T-Cell receptor.

86
SCID: Severe Combined Immunodeficiency Disease
Severe impairment of humoral and cellular immunity Triad of Moniliasis of the oropharynx and skin, intractable diarrhea, and pneumonia. Overwhelming viral infection is the cause of death. Deficiency or total absence of circulating lymphocytes

87
Thymoma with Immunodeficiency
Good’s syndrome Deficient in cell mediated immunity and benign thymoma occurring simultaneously Deficiency of B and pre-B cells is striking Thymectomy does not affect the immunodeficiency

88
Ataxia-Telangiectasia (Louis-Bar’s S.)
Distinctive telangiectasia in bulbar conjuctiva and flexural suraces of the arm developing during the 5th year of age Telangiectasia occurs on butterfly area of the face, palate, ear, and exposed skin. Café au lait patches, and graying hair also present. Cerebellar ataxia is the first sign of this syndrome, beginning in the second year of life. Choreic and athetoid movement present.

90
Ataxia-Telangiectasia
Progeric changes seen in 90% Subcutaneous fat is lost Facial skin becomes atrophic and sclerotic early on Poikiloderma Sinopulmonary infections in 80% Defects in cell mediated immunity Most common cause of death is bronchiectasis with respiratory failure

91
Persistent granulomatous plaques on the leg of child with ataxia–telangiectasia.

92
Wiskott-Aldrich Syndrome
Exclusively in boys Triad: chronic eczematous dermatitis resemble AD, increase suseptibility to infections (OM), and thrombocytopenia purpura/hepatosplenomegly Death by age 6 Accelerated IgA, IgM and IgE synthesis T-cell decline in numbers and activity Xp11 gene mutation. Codes for WASP protein which reorganize cytoskeleton Bone marrow transplant is tx of choice
, and thrombocytopenia purpura/hepatosplenomegly. Death by age 6. Accelerated IgA, IgM and IgE synthesis. T-cell decline in numbers and activity. Xp11 gene mutation. Codes for WASP protein which reorganize cytoskeleton. Bone marrow transplant is tx of choice.")
93
The boy was successfully treated with bone marrow transplantation, and his dermatitis virtually cleared owing to the T-cell engraftment

94
Petechiae and ecchymoses in a young boy with WAS

95
X-Linked Lymphoproliferative Syndrome
Aka Duncan’s disease Inability to control Epstein-Barr virus infection. Pt normal until develop infectious Mono. Necrotic hepatitis and exanthem are common Xq26 abnormailty B-cell lymphoproliferative disease with acquired hypoglobulinemia.

96
Chronic Granulomatous Disease
Recurring purulent and granulomatous infections involving long bones, lymphatic tissue, liver, skin, and lung. Deficient in one of the component of NADPH-oxidase complex, which generates superoxide. Leads to inability to destroy bacteria per radical mechanism Patients develop granulomas as a compensatory effort to confine organisms

97
Chronic Granulomatous Disease
65% of cases are the X-linked form, lacks the subunit of cytochrome b 558(gp91-phox) Female carrier has mixed, normal and abnormal cells thus shows an intermediate phenotype.
 Female carrier has mixed, normal and abnormal cells thus shows an intermediate phenotype.")
98
Chronic Granulomatous Disease
Myeloperoxidase producing bacteria characteristically cause infections because their destruction requires generation of oxygen free radicals Staph. Aureus Serratia

99
Chronic Granulomatous Disease
Screening test: Nitroblue tetrazolium (NBT) reduction assay NBT is normally yellow 80-90% of normal leukocytes reduce NBT during phagocytosis to insoluble precipitate, turning it blue Only 5-10% of leukocytes from patients with CGD are able to reduce NBT during phagocytosis
 reduction assay. NBT is normally yellow % of normal leukocytes reduce NBT during phagocytosis to insoluble precipitate, turning it blue. Only 5-10% of leukocytes from patients with CGD are able to reduce NBT during phagocytosis.")
100
Swollen, erythematous draining inguinal lymphadenopathy related to Staphylococcus aureus infection in a boy with chronic granulomatous disorder

101
Leukocyte Adhesion Molecule Deficiency
Autosomal recessive Necrotic ulcerations resembling pyoderma gangrenosum Frequent skin infections, mucositis, and otitis Poor wound healing Delayed separation of the umbilical cord Faulty complexing of the CD11 and CD18 integrins Death occurs by 2 years of life unless bone marrow transplant is undertaken.

102
A minor scratch from his sister evolved during the subsequent weeks into a large ulcer on the arm of a boy with leukocyte adhesion disorder.

103
Chediak-Higashi Syndrome
Autosomal recessive Abnormal pigmentation with silvery hair Photophobia Partial oculocutaneous albinism, cutaneous and intestinal infections early in childhood Ocular albinism is accompanied by nystagmus and photophobia. Parental consanguinity common

104
Chediak-Higashi Syndrome
Defect in the gene LYST, resulting in defective vesicular transport to and from the lysosome and melanosome Causes the “giant” intracytoplasmic granules found within leukocytes, melanocytes, hair shafts, renal tubular cells, CNS neurons, and other tissues

105
Light microscopic examination of hair shows giant melanosomes in patients with Chédiak–Higashi syndrome.

106
Hyperimmunoglobulinemia E Syndrome
Autosomal dominant with variable expressivity Consists of atopic-like eczematous dermatitis, recurrent pyogenic infection, high level of IgE, elevated IgD, IgE antistaph antibodies, and eosinophilia. Face is consistently involved. Begin early in life (2 month to 2 years) Lesions resemble prurigo Keratoderma of the palms and soles
 Lesions resemble prurigo. Keratoderma of the palms and soles.")
107
Coarse faces with scattered small staphylococcal pustules on a 9-year-old boy with hyperimmunoglobulin E syndrome.

108
Job’s syndrome AKA Buckley Syndrome Subset of HIE.
Mainly affect girls with red hair, freckles, and blue eyes. Hyperextensible joints Cold abscesses occur.

109
Infant with hyperimmunoglobulin E syndrome shows several erythematous, slightly purulent ‘cold’ abscesses on the forehead and scalp.

110
Graft-Versus-Host Disease
Immunocompetent cells are introduced as graft or blood transfusion to host who is unable to reject the graft cell. Most commonly after bone marrow transplant. Begins between 4-5th weeks after transplant. Result in exfoliative erythroderma.

111
Early, chronic graft-versus-host reaction with widespread, almost confluent hyperpigmented lichenoid papules and toxic epidermal necrosis-like appearance on knee

112
Late, chronic graft-versus -host reaction with hyperpigmented sclerotic plaques on the back

113
Acute graft-versus-host reaction with vivid palmar erythema

114
Graft-versus-host reaction with early, chronic, diffuse, widespread lichenoid changes of lips

115
Acute erosions of the buccal mucosa in graft-versus-host reaction

116
Graft-versus-host reaction; acute basal cell hydropic degeneration with interepidermal necrotic keratinocytes

117
Graft-versus-host reaction; early chronic hyperkeratosis and hypergranulosis, irregular acanthosis, cytoid body and basal cell hydropic degeneration reminiscent of lichen planus

118
Screening laboratory tests for a patient with recurrent cutaneous infections (including staphylococcal) where there is suspicion of a primary immunodeficiency
 where there is suspicion of a primary immunodeficiency")
119
End of Lecture…

Similar presentations