Download presentation
Presentation is loading. Please wait.

2
Breech Management By Dr. Khattab KAEO Prof & Head of Obstetrics and Gynaecology Department Faculty of Medicine, Al-Azhar University, Damietta

3
Breech delivery is not just a vertex delivery in reverse. The principal options are: * A trial of vaginal delivery. * Elective CS. * External cephalic version.

4
Mode of delivery: CS is not a routine. The fear of litigation, how- ever, greatly contributed to CS shift. More than half of breech presentations can be delivered vaginally.

5
Vaginal delivery is associated with in- creased perinatal mortality& morbidity, while CS is associated with increased maternal morbidity and is more costly. However, the increase in perinatal mortality &morbidity is not only related to the mode of delivery; prematurity, congenital malformations, PPROM and cord prolapse, all are more common with breech presentations. The rate of cerebral palsy is high regardless of the mode of delivery. The perinatal morbidity rate depends on the quality of birth management and criteria for admission to a trial of vaginal breech delivery (selection).
..")
6
Modified Zatuchni-Andros score for vaginal breech delivery. Modified Zatuchni-Andros score for vaginal breech delivery.

7
Selection criteria: Not completely reliable. Type of breech, EFW and pelvic dimensions are important factors. Parity is less important. Pelvimetry is not a routine. CS is offered for EFWs of 3.75 kg. With a frank or complete breech, normal pelvis and EFW between 1.5 & 3.8 kg, assisted breech delivery is probably as safe as a CS.

8
Exclusion criteria: EFW 3800 g. It should be noted that the error margins in fetal weight estimations may be higher with breech presentations (1 kg). Macrocephaly. Hyperextended head. Footling presentation. Others like placenta praevia and feto-pelvic disproportion. Ultrasound examination will diagnose head extension (a clear indication for CS).
. Macrocephaly. Hyperextended head. Footling presentation. Others like placenta praevia and feto-pelvic disproportion. Ultrasound examination will diagnose head extension (a clear indication for CS)..")
9
Vaginal delivery requirements ~ Anaesthesia is immediately available; ~ Ready access to CS. ~ Continuous electronic fetal monitoring. ~ Two obstetricians experienced with breech delivery. ~ Two paediatricians.

10
Technique - Induction & augmentation are allowed in selected cases - Fetal bl samples from buttocks provide an accurate assessment of the A-B status when FHR is suspect. - Membranes should be kept intact and pushing should be delayed as long as possible. - No interference before delivery of the umbilicus. The buttocks, legs and abdomen should be allowed to deliver spontaneously. - Episiotomy is considered when crowning occurs. - Forefingers in the groins and thumbs on the sacrum to keep the back always anterior. Rest of the fetal body should be delivered promptly. - When the scapulae appear, fingers should be placed over the shoulders from the back. The humerus should be followed down, and each arm rotated across the chest and out (Lovsett's manoeuvre). To deliver the right arm, the fetus is rotated in anti-clockwise direction; to deliver the left arm, the fetus is rotated in a clockwise direction. A gentle steady downward traction should be kept during rotation.
. To deliver the right arm, the fetus is rotated in anti-clockwise direction; to deliver the left arm, the fetus is rotated in a clockwise direction. A gentle steady downward traction should be kept during rotation..")
11
- Delivery of the head by 1 of the following methods: * Burns-Marshall technique: The body of the fetus, while supported to avoid sudden slipping, is left hanging down from the edge of the table. When the suboccipital region appears below the symphysis pubis, the fetus's ankles are grasped and the fetus is moved towards the mother's abdomen to deliver the head in flexion. * Burns-Marshall technique: The body of the fetus, while supported to avoid sudden slipping, is left hanging down from the edge of the table. When the suboccipital region appears below the symphysis pubis, the fetus's ankles are grasped and the fetus is moved towards the mother's abdomen to deliver the head in flexion. * Mauriceau-Smellie-Veit technique (Jaw flexion – shoulder traction): While the fetus is riding over the obstetrician's Lt forearm, its head is maintained in flexion by the obstetrician's Lt index& middle fingers that apply pressure on the fetus's low or upper jaw. 2 fingers of the Rt hand are hooked over the fetal neck grasping the shoulders, and traction is applied downwards and backwards until the suboccipital region appears below the symphysis pubis, then the fetus is moved towards the mother's abdomen to deliver the head in flexion. * Mauriceau-Smellie-Veit technique (Jaw flexion – shoulder traction): While the fetus is riding over the obstetrician's Lt forearm, its head is maintained in flexion by the obstetrician's Lt index& middle fingers that apply pressure on the fetus's low or upper jaw. 2 fingers of the Rt hand are hooked over the fetal neck grasping the shoulders, and traction is applied downwards and backwards until the suboccipital region appears below the symphysis pubis, then the fetus is moved towards the mother's abdomen to deliver the head in flexion. The operator uses both hands simultaneously to exert continuous downward gentle traction bilaterally on the fetal neck & on the maxilla. Suprapubic pressure by an assistant maintains flexion of the head.
: While the fetus is riding over the obstetrician s Lt forearm, its head is maintained in flexion by the obstetrician s Lt index& middle fingers that apply pressure on the fetus s low or upper jaw. 2 fingers of the Rt hand are hooked over the fetal neck grasping the shoulders, and traction is applied downwards and backwards until the suboccipital region appears below the symphysis pubis, then the fetus is moved towards the mother s abdomen to deliver the head in flexion. * Mauriceau-Smellie-Veit technique (Jaw flexion – shoulder traction): While the fetus is riding over the obstetrician s Lt forearm, its head is maintained in flexion by the obstetrician s Lt index& middle fingers that apply pressure on the fetus s low or upper jaw. 2 fingers of the Rt hand are hooked over the fetal neck grasping the shoulders, and traction is applied downwards and backwards until the suboccipital region appears below the symphysis pubis, then the fetus is moved towards the mother s abdomen to deliver the head in flexion. The operator uses both hands simultaneously to exert continuous downward gentle traction bilaterally on the fetal neck & on the maxilla. Suprapubic pressure by an assistant maintains flexion of the head..")
13
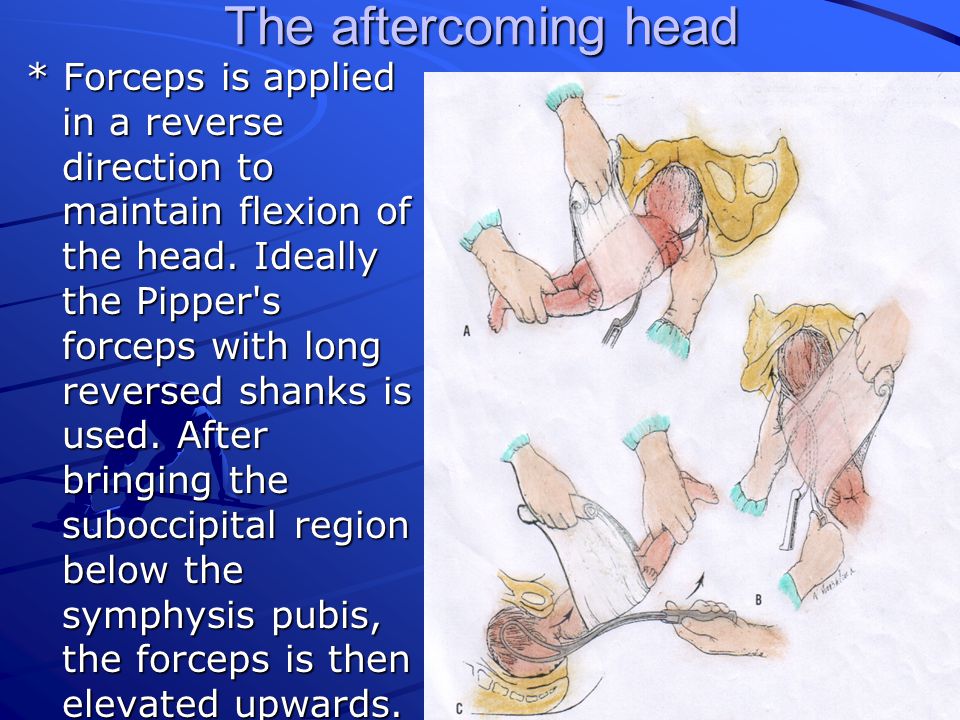
The aftercoming head * Forceps is applied in a reverse direction to maintain flexion of the head. Ideally the Pipper's forceps with long reversed shanks is used. After bringing the suboccipital region below the symphysis pubis, the forceps is then elevated upwards.

14
Breech extraction It is mainly indicated to deliver the 2nd twin & in case of prolapsed pulsating cord with the breech engaged & the cervix is fully dilated. It can be accomplished by moderate traction by a finger in each groin (or the anter. groin alone, but not the post. groin alone). If moderate traction does not effect delivery, breech de- composition i.e. converting the frank breech into footling. 2 fingers are carried up along the anterior thigh to the knee to push it away from the midline by pressing on the popliteal fossa. Spontaneous flexion usually follows, and the foot is grasped & brought down (Pinard manov If we bring the posterior leg, the anter buttock may override the symphysis pubis. This is contrary to extended arms where we can bring the posterior arm first (introducing the hand along concavity of the sacrum is easier). If the anterior arm overrides the symphysis pubis, there is no great problem because we can hold the trunk and rotate it 180 to bring the anter. arm posteriorly then delivering it.
. If moderate traction does not effect delivery, breech de- composition i.e. converting the frank breech into footling. 2 fingers are carried up along the anterior thigh to the knee to push it away from the midline by pressing on the popliteal fossa. Spontaneous flexion usually follows, and the foot is grasped & brought down (Pinard manov If we bring the posterior leg, the anter buttock may override the symphysis pubis. This is contrary to extended arms where we can bring the posterior arm first (introducing the hand along concavity of the sacrum is easier). If the anterior arm overrides the symphysis pubis, there is no great problem because we can hold the trunk and rotate it 180 to bring the anter. arm posteriorly then delivering it..")
16
Breech extraction (Cont.) The ankles are held with the 2nd finger lying between them & gentle downward traction is exerted. As the legs emerge, successively higher portions are grasped. A cardinal rule is to employ steady, gentle, downward rotational traction until the lower 1/2 of the scapulas are delivered outside the vulva - making no attempt at delivery of the shoulders and arms before that. The anter shoulder & arm are released & delivered first The body of the fetus is then rotated in the reverse direction to deliver the other shoulder and arm. The body of the fetus is then rotated in the reverse direction to deliver the other shoulder and arm. If trunk rotation is unsuccessful, the posterior shoulder must be delivered first. The feet are grasped and drawn upward over the inner thigh of the mother toward which the ventral surface of the fetus is directed. Then, by depressing the body of the fetus, the anterior shoulder emerges beneath the pubic arch, thereafter, the back tends to rotate spontaneously in the direction of the symphysis.

18
Complicated vaginal breech delivery

19
Arrest of the buttocks at the pelvic outlet Extension of the legs is the main cause because they interfere with lateral flexion of the spine. This can be managed by Pinard manoev. or by groin traction. Groin traction is performed by putting the index finger in the anterior groin for traction during uterine contractions. This may be helped by fundal pressure. When the posterior groin canbe reached traction is made on both groins, down- ward and backward until the anterior groin appears below the symphysis pubis, and then upward to deliver the posterior buttock. Traction should be directed towards the trunk not the thigh to avoid fracture of the femur.

21
Posteriorly rotated head Prague technique: Rarely, the back of the fetus fails to rotate to the anterior. Rotation may, then, be achieved by using stronger traction on the fetal bony pelvis. If the back still remains posteriorly, the fetus still may be delivered using the modified Prague manoeuvre. It consists of grasping the shoulders of the back-down fetus by two fingers of one hand, from below, while the other hand draws the feet up over the maternal abdomen.

23
Extended arms It usually occurs due to traction before full dilatation of the Cx. Classical method: UGA, the poster. arm is brought down first. A hand is passed along the arm to the cubital fossa, & 2 fingers press to flex the forearm. If there is no enough space anteriorly, we can hold the trunk & rotate it 180 to bring the anterior arm posteriorly then delivering it by the same procedure. Lovsett's technique: This is the method of choice because there is no need for anaesthesia or to pass the hand into the vagina. The fetus is grasped by the pelvic girdle. Traction is applied downward until the inferior angle of the anter scapula appears below the symphysis pubis. Then, the fetus is rotated 180 to bring the post shoulder below the symphysispubis where the arm can be brought down Then, the fetus is rotated 180 in the opposite direction to bring the other shoulder anterior below the symphysis pubis where the other arm can be brought down too. During rotation shoulders descend for few Cms which are enough to assist delivery. During rotation the fetal back should always remain anterior.

25
Nuchal displacement of the arm It results from rotating the trunk in the wrong direction during delivering the extended arm. Treatment is by rotating the trunk at least 90 in the direction of the tips of fingers of the displaced hand until the fetal back is directed toward one side of the pelvis. During rotation, the arm will usually be forced to an extended position by the pressure from the pelvic brim. The arm is, then, swept downward over the face and chest.

27
Double nuchal arms

29
Caesarean section Indications = exclusion criteria for vaginal breech delivery + other indications for CS e.g. previous 2 CS, placenta praevia, etc. It should be emphasized that CS is indicated with any degree of pelvic contraction. This is because with term fetus some degree of head molding may be essential to negotiate the birth canal successfully. In breech presentation, once the breech has passed beyond the vaginal introitus, the abdomen, thorax, arms & head should be delivered promptly. This involves delivery of successively less compressible parts. CS due to only breech presentation is followed by >80% possibility of vaginal delivery of the next pregnancy if the presentation is vertex.

30
Thank you

Similar presentations