Download presentation
Presentation is loading. Please wait.

1
Seasonal flu vaccination programme (2010/2011) September 2010 Dr Syed Ahmed Consultant in Public Health Medicine and Immunisation Coordinator NHS Greater Glasgow and Clyde
 September 2010 Dr Syed Ahmed Consultant in Public Health Medicine and Immunisation Coordinator NHS Greater Glasgow and Clyde")
2
Seasonal flu vaccination programme 2010-2011 Background information about flu viruses Epidemiology of Flu A viruses Vaccines against flu viruses and their indications and safety Rationale for policy in 2010/11 flu season Programme implementation issues and good practice guidance

3
Influenza viruses: three types Type A –Causes epidemics and pandemics –3 pandemics in the last century in 1918, 1957, 1968 and the latest in 2009 Type B –Do not cause pandemics but may cause localised epidemics Type C –Do not cause pandemics or epidemics –Minor respiratory illness only

4
Influenza A viruses (1) 1918 pandemic by H1N1 and became the established Flu A until 1956 1957 pandemic by H2N2 and became the established Flu A until 1967 1968 pandemic by H3N2 and became the established Flu A until 1976
 1918 pandemic by H1N1 and became the established Flu A until pandemic by H2N2 and became the established Flu A until pandemic by H3N2 and became the established Flu A until 1976")
5
Influenza A viruses (2) 1977 – outbreaks of H1N1 (Red Flu) but did not cause a pandemic and did not replace H3N2 From 1977 to 2008 a combination of H3N2 and H1N1 (Red Flu) in circulation 2009 pandemic by H1N1 (2009) Which Flu A is going to be the dominant strain from 2010?
 1977 – outbreaks of H1N1 (Red Flu) but did not cause a pandemic and did not replace H3N2 From 1977 to 2008 a combination of H3N2 and H1N1 (Red Flu) in circulation 2009 pandemic by H1N1 (2009) Which Flu A is going to be the dominant strain from 2010")
6
Flu A: lessons from the Southern Hemisphere In 2010 winter In Chile, mainly H1N1 (2009) in peak winter (June/July) but also emergence of H3N2 in late winter (Aug/Sept) In Australia, mainly H1N1 (2009) In New Zealand, mainly H1N1 (2009) In South Africa, mainly H3N2 in early winter but increasing proportion of H1N1 (2009) in late winter.
 in peak winter (June/July) but also emergence of H3N2 in late winter (Aug/Sept) In Australia, mainly H1N1 (2009) In New Zealand, mainly H1N1 (2009) In South Africa, mainly H3N2 in early winter but increasing proportion of H1N1 (2009) in late winter.")
7
Influenza A virus in 2010/2011? ?Best guess –Flu A viruses behaviour –Experience from Southern Hemisphere –In the Northern Hemisphere probably main Flu A would be H1N1 (2009) but also H3N2.
 but also H3N2..")
8
Influenza Vaccine (2010/2011) Trivalent (seasonal flu) vaccine –Flu A H1N1 (2009) strain –Flu A H3N2 strain –Flu B Monovalent H1N1 (2009) vaccine available since 2009
 Trivalent (seasonal flu) vaccine –Flu A H1N1 (2009) strain –Flu A H3N2 strain –Flu B Monovalent H1N1 (2009) vaccine available since 2009")
9
Trivalent Seasonal Flu (2010/2011) and monovalent H1N1 (2009) vaccines (1) Trivalent seasonal flu vaccine –“traditional” flu vaccine –Protect against 3 different flu strains –No adjuvant present –Give short term protection –Poor immunological response to children under 5 years, those immunocompromised and older people –Tried and tested technology –Long track record on safety –Easy to deliver as come in single dose prefilled syringe
 and monovalent H1N1 (2009) vaccines (1) Trivalent seasonal flu vaccine – traditional flu vaccine –Protect against 3 different flu strains –No adjuvant present –Give short term protection –Poor immunological response to children under 5 years, those immunocompromised and older people –Tried and tested technology –Long track record on safety –Easy to deliver as come in single dose prefilled syringe")
10
Trivalent Seasonal Flu (2010/2011) and monovalent H1N1 (2009) vaccines (2) Monovalent H1N1 (2009) vaccine –Protects against only single strain –Has adjuvant in it with longer protection –Initial concern about safety as brought in quickly to stem pandemic last year –Tenuous historical links between previous “swine flu” vaccine and Guillain-Barré syndrome –Comes in 10 dose vial with thiomersal BUT –Over 6 million doses used in the UK including in pregnant women –Immunologically better response including in children under 5 and those immunocompromised.
 and monovalent H1N1 (2009) vaccines (2) Monovalent H1N1 (2009) vaccine –Protects against only single strain –Has adjuvant in it with longer protection –Initial concern about safety as brought in quickly to stem pandemic last year –Tenuous historical links between previous swine flu vaccine and Guillain-Barré syndrome –Comes in 10 dose vial with thiomersal BUT –Over 6 million doses used in the UK including in pregnant women –Immunologically better response including in children under 5 and those immunocompromised.")
11
Epidemiology/Surveillance Distribution by age group of influenza hospitalised cases Emerging Infections Programme Pandemic H1N1 - 14 July 2009 in the USA

12
Influenza A: risk factors for severe complications Flu A (H3N2) –Underlying chronic conditions –Predominantly affect older age groups –Immunocompromised individuals Flu A (H1N1) 2009 –Underlying chronic conditions –Predominantly affect younger age groups –Immunocompromised individuals –Pregnant women –Metabolic abnormality, eg obesity
 –Underlying chronic conditions –Predominantly affect older age groups –Immunocompromised individuals Flu A (H1N1) 2009 –Underlying chronic conditions –Predominantly affect younger age groups –Immunocompromised individuals –Pregnant women –Metabolic abnormality, eg obesity")
14
Pregnant Women and H1N1 (2009) ANZIC Influenza Study Investigators carried out a detailed study of all critically ill patients in Australia and New Zealand with H1N1 infection, specially looked at pregnant and postpartum women Pregnant women around 7x higher risk of admission to intensive care compared with non-pregnant women of childbearing age 69% of pregnant women admitted to intensive care needed mechanical ventilatory support Mortality for these critically ill pregnant women was 11% (33% for those requiring ECMO) and foetal loss was 12%
 ANZIC Influenza Study Investigators carried out a detailed study of all critically ill patients in Australia and New Zealand with H1N1 infection, specially looked at pregnant and postpartum women Pregnant women around 7x higher risk of admission to intensive care compared with non-pregnant women of childbearing age 69% of pregnant women admitted to intensive care needed mechanical ventilatory support Mortality for these critically ill pregnant women was 11% (33% for those requiring ECMO) and foetal loss was 12%")
15
Flu vaccination policy for 2010/2011 winter season Those in “at risk groups” need protection from both H1N1 and H3N2 Pregnant women not in the “at risk groups” need protection mainly from H1N1 (for short term only) Over 65s mainly need protection against H3N2 For immunocompromised and children under 5 monovalent H1N1 vaccine gives much better protection against H1N1 (2009) than the trivalent vaccine.
 Over 65s mainly need protection against H3N2 For immunocompromised and children under 5 monovalent H1N1 vaccine gives much better protection against H1N1 (2009) than the trivalent vaccine.")
18
Group 1: Summary Not in high risk groups for H1N1 complications Need one dose of trivalent vaccine to protect against all 3 strains

20
Group 2: Summary Children under 13 years need two doses of the trivalent seasonal flu vaccine if no seasonal flu vaccine in previous years Children under 5 years need a single dose of monovalent H1N1 if they have not received a previous H1N1 as they do not respond well to trivalent flu vaccine

22
Group 3: Summary All immunocompromised patients need a dose of monovalent H1N1 vaccine if they have not had it previously to protect them against H1N1 (2009) All immunocompromised under 13 years need two doses of trivalent flu vaccine if they had no previous seasonal flu vaccine All immunocompromised over 13 years only need one dose of trivalent flu vaccine
 All immunocompromised under 13 years need two doses of trivalent flu vaccine if they had no previous seasonal flu vaccine All immunocompromised over 13 years only need one dose of trivalent flu vaccine")
23
Immunosuppressed individuals As detailed in the “Green Book” –Due to disease or treatment –Patients undergoing chemotherapy –Asplenia or splenic dysfunction –HIV patients –Individuals on systemic steroids for more than a month at a dose equivalent to Prednisolone at 20mg or more per day, or children under 20kgs at a dose of 1mg or more/kg/day

24
Immunosuppressed individuals ? Patients on DMARD –Single dose unless evidence of immunosuppression

26
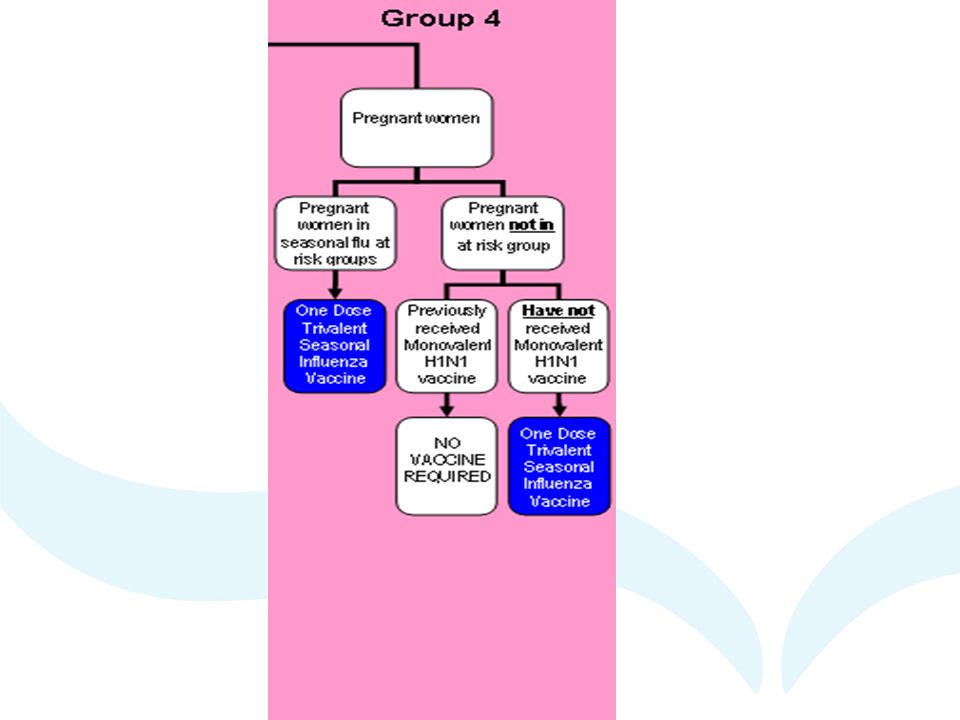
Group 4: Summary No monovalent H1N1 vaccine for pregnant women from October 2010 as they respond well to trivalent vaccine and also only need short term protection Pregnant women in clinical at risk groups need a dose of trivalent flu vaccine Pregnant women NOT in clinical risk groups ALSO need a dose of trivalent flu vaccine UNLESS they have already had a dose of H1N1, as they mainly need protection against H1N1.

27
Flu vaccines: safety data H1N1 monovalent vaccine contains thiomersal and adjuvant but over 6 million doses given last year with no safety concerns Thiomersal adjuvants used in vaccines for over 60 years and found to be safe Seasonal flu vaccines have a long safety record No increase in Guillain-Barré syndrome in the UK last year after H1N1 vaccination Both H1N1 and trivalent vaccine found to be safe in pregnant women

28
Flu vaccine: contraindications Previous life-threatening allergic reaction to flu vaccines Life-threatening reaction to any components of the vaccines If severe life-threatening allergic reaction to egg and egg products

29
Flu vaccines: adverse reactions Headache, fatigue, fever, arthralgic myalgia, pain and redness at injection site A small painless nodule may also form at the injection site Enzira or CSL Biotherapies Generic Influenza vaccines should not be given to under 5s as higher than expected increase in febrile convulsions in Australia.

Similar presentations













 Management Presentation>")








 Virus>")

