Download presentation
1
HYPOTHYROIDISM IN PREGNANCY Mary Lacy

2
Case at the VA 29yo G2P1 w/ h/o poorly controlled primary hypothyroidism. b-hcg positive on 3/15 and TSH that same day of 101.5. Pt has been on 112mcg of levothyroxine since December when her dose was increased from 88mcg 2/2 TSH of 40. What did we do? Increased dose to 150mcg based on 1.6mcg/kg and adding 30% for increased demands in pregnancy Repeat labs (recommended q4-6 weeks in pregnancy rather than q6-8weeks) Most recent labs (at 11 weeks): TSH: 39.81 Free T4: 1.31
 Most recent labs (at 11 weeks): TSH: Free T4:")
3
Classifications of Hypothyroidism Overt Hypothyroidism: 0.3-0.5% of screened women Increased TSH, Decreased Free T4 Subclinical Hypothyroidism: 2-2.5% of screened women Increased TSH, Normal Free T4

4
Changes in labs during pregnancy Increased TBG Increased Total T4/Total T3 secondary to increased Estrogen Serum TSH decreases early in gestation with rise in free T3/free T4 Secondary to hCG stimulation of thyroid normalizes by end of first Trimester Normal TSH in pregnancy First trimester: 0.1-2.5 mIU/L Second Trimester: 0.2-3.0 mIU/L Third Trimester: 0.3-3.0 mIU/L

5
Thyroid in Fetal development Thyroid hormone receptor expressed in fetus at 8-10weeks Reports of when fetus begins to produce thyroid hormone vary, most reports stated 18 weeks, some said 11-12 weeks

6
Observational study between 1987 – 1999 in Argentina Followed 150 consecutive pregnancies of 114 women with primary hypothyroidism (primarily chronic lymphocytic) 99 women were euthyroid on LT4 51 were hypothyroid – 16 with OH, 35 with SCH
 99 women were euthyroid on LT4 51 were hypothyroid – 16 with OH, 35 with SCH")
7
Thyroid Status at Conception Pregnancy LossTerm Delivery Euthryoid (n = 99) 4/99 (4%)84/99 (84.5%) Hypothyroid (n = 51) 16/51 (31.4%)30/51 (59%) p<0.0001p = 0.18 TSH < 4 TSH > 4 92.6% 20.8% p<0.006 0% 66.7% p<0.006
 4/99 (4%)84/99 (84.5%) Hypothyroid (n = 51) 16/51 (31.4%)30/51 (59%) p<0.0001p = 0.18 TSH < 4 TSH > % 20.8% p< % 66.7% p<0.006")
8
4,657 women screened with TSH/TPO-Ab within first 11 weeks of gestation in Southern Italy Subset of women with TPO-Ab negativity: Group A: TSH < 2.5 Group B: TSH between 2.5 – 5.0 Study assessed pregnancy loss, pre-term and very pre-term delivery

9
p=0.006

10
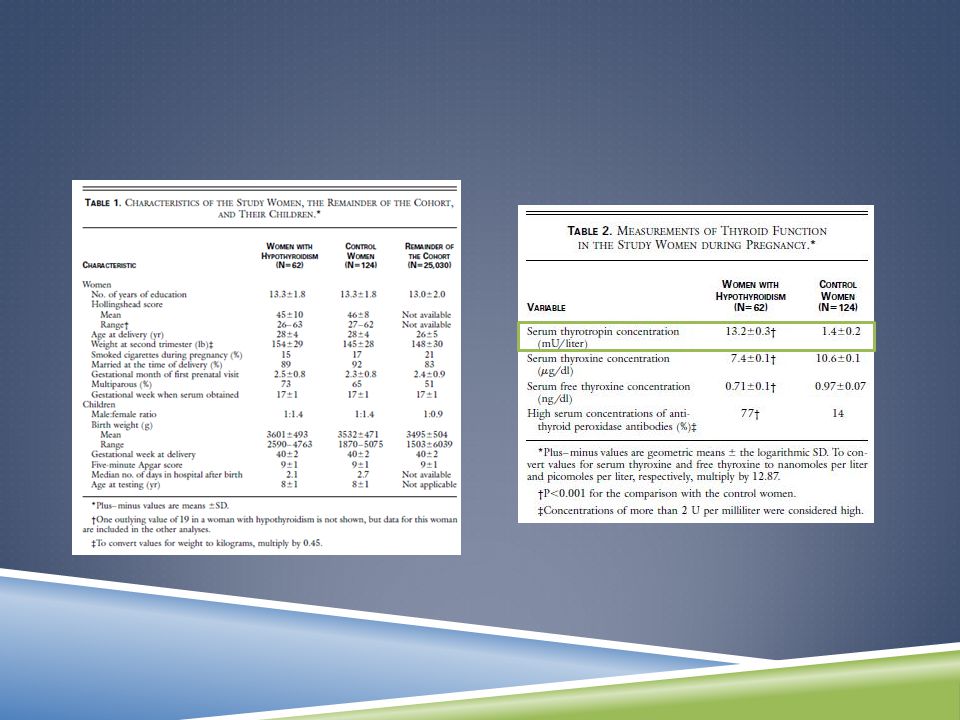
Retrospective analysis of TSH/freeT4/TPO-Ab in 2 nd trimester serum samples of 25,216 pregnant women from 1987-1990 in Maine 47 women with TSH > 99.7% of all values 15 women with TSH in 98-99.7% + T4 < 7.75mcg/dL (4.6-12) Prospective study of 62 children born to mothers with hypothyroidism compared to 124 control children from same schools 7-9 year old children who were euthyroid at birth underwent 15 test of intelligence, school performance, visual-motor performance, etc.
 Prospective study of 62 children born to mothers with hypothyroidism compared to 124 control children from same schools 7-9 year old children who were euthyroid at birth underwent 15 test of intelligence, school performance, visual-motor performance, etc.")
13
RCT of 10 centers in UK and 1 in Italy

14
Target TSH 0.1-1.0

17
Contrasting these papers Haddow 1999Lazarus 2012 Type of studyObservational study of hypothyroid mothers (tx/no tx) vs. non-hypothyroid mothers RCT of treated vs untreated “hypothyroidism” Serum Samples2 nd trimester12-13 weeks TSH Average13.23.8/3.1 Child Testing7-9 years3 years

18
Prospective study in the Netherlands between January - November 1994 448 pregnant women initially assessed Maternal fT4, TSH, TPO-Ab measured at 12 weeks gestation, 32 weeks gestation, and post-partum 220 children from uncomplicated pregnancies/deliveries Neurodevelopment assessed at 10 months

19
Lowest 5% fT4 Lowest 10% fT4 Lowest 15% fT4 Lowest 20% fT4 R = 0.46; p=0.03 Mean difference in Lowest 5% of free T4 = 14.1* (5.9 – 22.3) Mean difference in lowest 10% = 7.4* (1.1 – 13.9) Difference of 10 points on PDI score thought to reflect delay of one month
 Mean difference in lowest 10% = 7.4* (1.1 – 13.9) Difference of 10 points on PDI score thought to reflect delay of one month")
20
Observational case-control study in Maine in 2004 – 2006 Free T4 measured in 5,734 women with normal TSH (0.1-3.5) Women with free T4 ≤ 3% matched with women in 10-90 th % Measurement of Infant Development (VSID III) at age 2 years
 Women with free T4 ≤ 3% matched with women in th % Measurement of Infant Development (VSID III) at age 2 years")
22
So what should I do? If Hypothyroidism known prior to pregnancy – target TSH <2.5 (poor) Thyroxine requirements increase 30-50% by 4-6 weeks (good) can have patients increase dosing to 9 doses/week Targeted case finding for hypothyroidism as opposed to universal screening (fair) Treat overt hypothyroidism (good) Treat subclinical hypothyroidism improves obstetrical outcomes (fair) improves offspring development (poor) Patients with evidence of thyroid autoimmunity are at risk for OH, monitor them throughout pregnancy (fair)
 Thyroxine requirements increase 30-50% by 4-6 weeks (good) can have patients increase dosing to 9 doses/week Targeted case finding for hypothyroidism as opposed to universal screening (fair) Treat overt hypothyroidism (good) Treat subclinical hypothyroidism improves obstetrical outcomes (fair) improves offspring development (poor) Patients with evidence of thyroid autoimmunity are at risk for OH, monitor them throughout pregnancy (fair).")

















 In Macau, around.>")






