Download presentation
Presentation is loading. Please wait.

1
Improving HIV case detection Steve Baguley Genitourinary physician, Aberdeen

3
HIV in Scotland Health protection Scotland 2008

8
Late diagnosis

9
Undiagnosed – 2007 data

10
BHIVA Audit 2006: Scenario leading to death Mortality audit BHIVA audit and Standards Sub-Committee 2006; accessible at www.bhiva.org Top bars: reclassified during audit Bottom bars: as initially reported

11
National HIV testing guideline 2008 BHIVA, BASHH, BIS

12
Universal HIV testing is recommended in all of the following settings: GUM or sexual health clinics antenatal services termination of pregnancy services drug dependency programmes healthcare services for those diagnosed with tuberculosis, hepatitis B, hepatitis C and lymphoma.

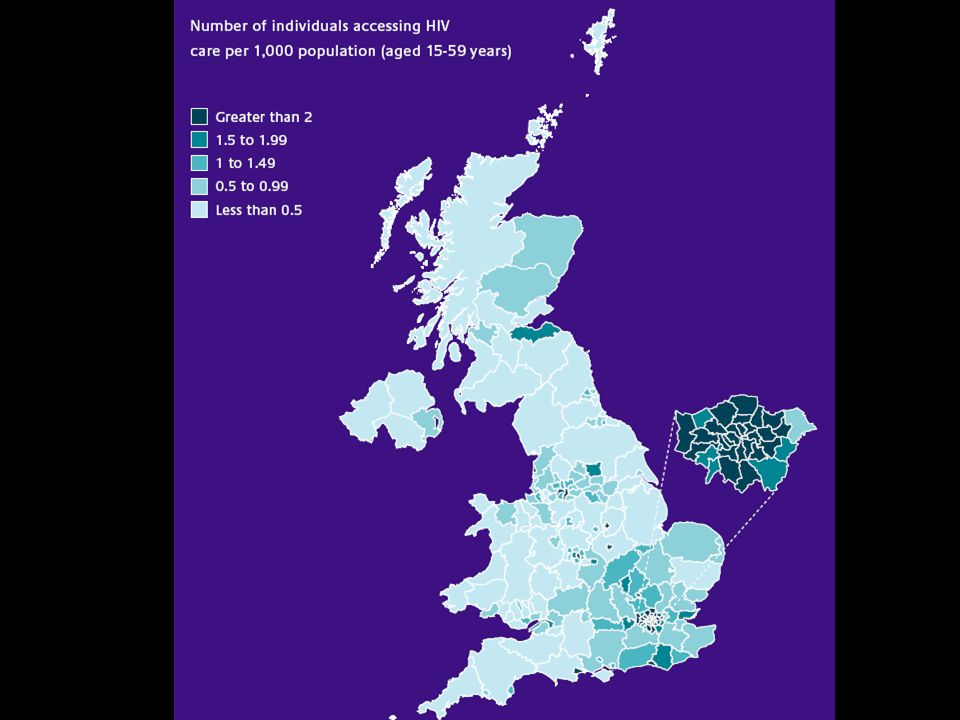
13
An HIV test should be considered in the following settings where diagnosed HIV prevalence in the local 15-59yr old population exceeds 2 in 1000 1. all men and women registering in general practice 2. all general medical admissions.

15
In other areas/populations In other areas a more selective approach is recommended –Testing is recommended if the prevalence in a sub-population is above a certain (unspecified!) level. Groups identified by social/sexual factors Groups identified by their diagnosis

16
HIV testing should be also routinely offered and recommended to the following patients 1. all patients presenting for healthcare where HIV, including primary HIV infection, enters the differential diagnosis 2. all patients diagnosed with a sexually transmitted infection 3. all sexual partners of men and women known to be HIV positive 4. all men who have disclosed sexual contact with other men 5. all female sexual contacts of men who have sex with men 6. all patients reporting a history of injecting drug use 7. all men and women known to be from a country of high HIV prevalence (>1%) 8. all men and women who report sexual contact abroad or in the UK with individuals from countries of high HIV prevalence.
 8. all men and women who report sexual contact abroad or in the UK with individuals from countries of high HIV prevalence..")
17
HIV indicator conditions Some well known to you as HIV related –Kaposi’s sarcoma –PCP Others less well known –Peripheral neuropathy –Recurrent herpes zoster –Weight loss of unknown cause –Lung cancer –Glandular fever-like syndrome (Primary HIV Infection)
")
19
The essential elements that the pre-test discussion should cover are: The benefits of testing to the individual Whether a repeat test might be needed (ie to cover the window period) Details of how the result will be given.
 Details of how the result will be given.")
20
Giving positive results As in any situation where bad news is being conveyed, the result should be given face to face in a confidential environment and in a clear and direct manner. Prior to giving the result, establish a clear pathway for onward referral. Any individual testing HIV positive should be seen by an HIV specialist at the earliest possible opportunity, preferably within 48 hours.

21
How it could work in practice Keith is a 45yr old man with recurrent community acquired pneumonia. He’s lost 10kg weight over the last 6 months. Non-smoker He’s come to see GP due to another episode of presumed pneumonia. An extract from the dialogue could be: “We need to do some investigations to see why you keep on getting these infections. I’ll organise a chest X-ray and we can do some blood tests for anaemia, HIV and to check your liver. How does that sound to you?”

23
We’re trying to normalise HIV testing. Think of it like any other test, the result of which could affect someone’s life. Many common presentations can be HIV related. HIV testing is straightforward and any healthcare professional should be able to do it. Bhiva.org

Similar presentations
























 Public Health England London,>")

