Download presentation
Presentation is loading. Please wait.

1
Validation of A Proposed Testing Strategy using FDA-approved Rapid Tests Eugene Martin, Ph.D. APHA 2008 Annual Meeting San Diego, CA October 25-29, 2008

2
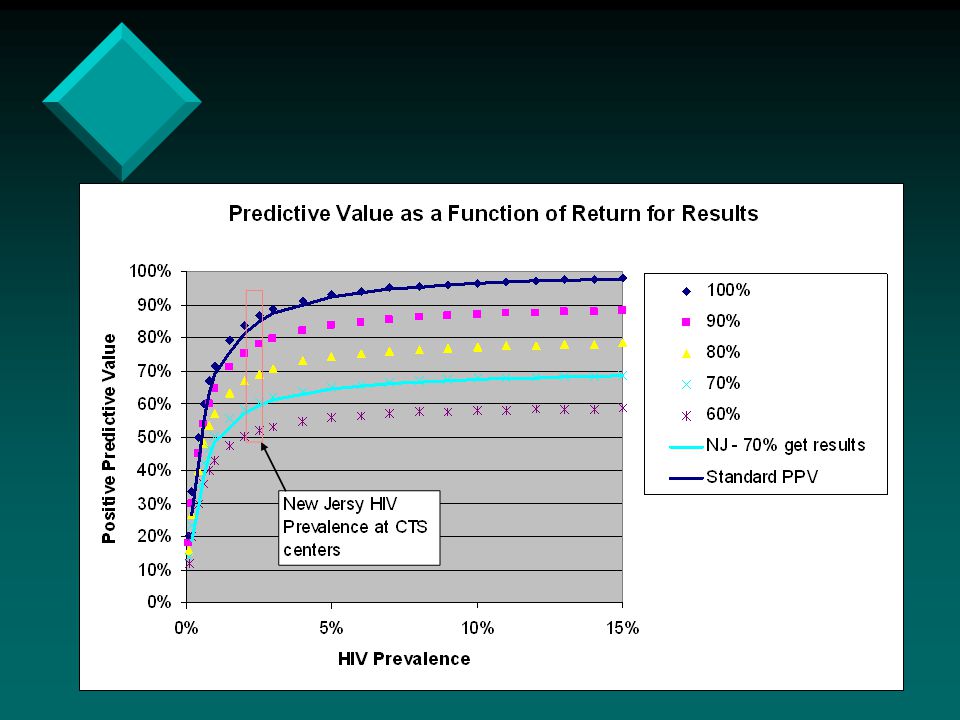
Rapid-rapid Verification Programs Factors to consider:Factors to consider: How is your program organized?How is your program organized? Is it centrally organized or groups of independent labs?Is it centrally organized or groups of independent labs? How much confidence do you have in each labs ability to handle multiple assays?How much confidence do you have in each labs ability to handle multiple assays? How much experience do your laboratories have in figuring out ‘discordant results’?How much experience do your laboratories have in figuring out ‘discordant results’? What will happen if there is a problem?What will happen if there is a problem? How prevalent is HIV where you are testing? As prevalence DECREASES…False Positives results REMAIN constant while true positives decrease. Are you prepared to deal with discordant results?How prevalent is HIV where you are testing? As prevalence DECREASES…False Positives results REMAIN constant while true positives decrease. Are you prepared to deal with discordant results?

3
NJ Rapid HIV Testing One of the largest, most centralized rapid HIV testing programs in the country:One of the largest, most centralized rapid HIV testing programs in the country: County health departmentsCounty health departments Sexually transmitted disease clinics,Sexually transmitted disease clinics, Family planning programs,Family planning programs, Federally qualified healthcare centers,Federally qualified healthcare centers, TB clinics,TB clinics, Prisons,Prisons, Hospital-based programs – 13 ERs (8 counties),Hospital-based programs – 13 ERs (8 counties), Prenatal clinics, andPrenatal clinics, and Outreach through mobile vans.Outreach through mobile vans.
,Hospital-based programs – 13 ERs (8 counties), Prenatal clinics, andPrenatal clinics, and Outreach through mobile vans.Outreach through mobile vans.")
4
New Jersey ‘s Rapid HIV Sites Rapid HIV Testing in NJ Testing Began 2003 23 primary sites 23 primary sites 32 satellite licenses 32 satellite licenses Western Blot confirmation at state lab (PHEL) in Trenton Western Blot confirmation at state lab (PHEL) in Trenton Over 70 CTS sites, including : Hospitals/EDs Hospitals/EDs FQHCs FQHCs CBOs CBOs Health departments Health departments Mobile vans Mobile vans Prisons Prisons
 in Trenton Western Blot confirmation at state lab (PHEL) in Trenton Over 70 CTS sites, including : Hospitals/EDs Hospitals/EDs FQHCs FQHCs CBOs CBOs Health departments Health departments Mobile vans Mobile vans Prisons Prisons")
5
Why a Centralized Program? STEPS pecialized skills are centralizedSpecialized skills are centralized esting and processes are organizedTesting and processes are organized xpenses are optimizedExpenses are optimized roblems are identified more quicklyProblems are identified more quickly Solutions are distributed to all:Solutions are distributed to all: http://www.njhiv1.orghttp://www.njhiv1.orghttp://www.njhiv1.org

6
Why Move to Rapid Confirmation? ProblemProblem Preliminary Positive clients fail to return for results (25.2%)Preliminary Positive clients fail to return for results (25.2%) NAP succeeds ONLY 20% of the time in locating these clientsNAP succeeds ONLY 20% of the time in locating these clients SolutionSolution Confirmatory testing on- site, same dayConfirmatory testing on- site, same day
Preliminary Positive clients fail to return for results (25.2%) NAP succeeds ONLY 20% of the time in locating these clientsNAP succeeds ONLY 20% of the time in locating these clients SolutionSolution Confirmatory testing on- site, same dayConfirmatory testing on- site, same day.")
7
Validation of a Testing Algorithm Can a second rapid HIV test confirm preliminary positives as effectively as a Western Blot? “ Validation is the process of demonstrating that an analytical procedure is suitable for its intended use” – CBER The use of other rapid tests to confirm a rapid HIV test is not new or novel - WHO recommends this approach for countries in which the prevalence of HIV exceeds 10% for a number of years What is new and novel is using this approach in sites with 2% or lower prevalence

8
What does any rapid test algorithm need to do? NEED TO DO Demonstrate SensitivityDemonstrate Sensitivity Identify True PositivesIdentify True Positives Not Identify False PositivesNot Identify False Positives Demonstrate ReproducibilityDemonstrate Reproducibility Demonstrate Robustness - remain unaffected by small, but deliberate, variations in method parametersDemonstrate Robustness - remain unaffected by small, but deliberate, variations in method parameters DATA Sensitivity & Specificity: Manufacturer’s Claims CDC Post Marketing Survey Follow-up Investigations: Existing confirmations Alternative testing

9
Questions for a Rapid Testing Algorithm (RTA): 1. 1.Are there false negative screening tests? i.e Screening test says NEG, but the client is infected. 2. 2.Can a positive client result be confirmed by a second rapid test? 3. 3.Can false positive screening tests be detected by running a second rapid test… or a third? What is the advantage? Disadvantage? 4. 4.How can inconclusive “second-round” test results (eg, WB vs a second rapid test) be resolved? 5. 5.What is the impact on the linkage to care?
 be resolved What is the impact on the linkage to care .")
10
NJ - A Two-Test Algorithm HIV-1/2 Rapid HIV Test (Blood) STAT-Pak Or HIV-1/2 Rapid HIV Test (Oral) Oraquick
 STAT-Pak Or HIV-1/2 Rapid HIV Test (Oral) Oraquick")
11
Unique Characteristics New Jersey: 7,836 sq. mi> Los Angeles: 469.1 sq mi> San Francisco: 47 sq. milesArea: New Jersey: 7,836 sq. mi> Los Angeles: 469.1 sq mi> San Francisco: 47 sq. miles Greater LA (2007) ~17.78 million NJ 8.69 million > San Francisco ~ 4.18 millionPopulation: Greater LA (2007) ~17.78 million > NJ 8.69 million > San Francisco ~ 4.18 million Drive End to End in NJ 3 hrs. (W E 1 ½ hours)Scale: Drive End to End in NJ 3 hrs. (W E 1 ½ hours) A mixture of urban/suburban and rural communitiesA mixture of urban/suburban and rural communities North – urbanNorth – urban South – ruralSouth – rural Many different venues perform rapid testingMany different venues perform rapid testing
 ~17.78 million NJ 8.69 million > San Francisco ~ 4.18 millionPopulation: Greater LA (2007) ~17.78 million > NJ 8.69 million > San Francisco ~ 4.18 million Drive End to End in NJ 3 hrs. (W E 1 ½ hours)Scale: Drive End to End in NJ 3 hrs. (W E 1 ½ hours) A mixture of urban/suburban and rural communitiesA mixture of urban/suburban and rural communities North – urbanNorth – urban South – ruralSouth – rural Many different venues perform rapid testingMany different venues perform rapid testing.")
12
Validation of the NJ algorithm Three Data Sets:Three Data Sets: 20042004 January, 2006 – October, 2007January, 2006 – October, 2007 20082008

13
2004 Ability of a Rapid to Confirm a Rapid ALL confirmatory specimens sent to NJ PHEL during 8 month period:ALL confirmatory specimens sent to NJ PHEL during 8 month period: 1. Re-ran the PHEL specimen using Oraquick again 2.Re-ran the specimen with other rapid tests 3.Confirmed negative result by repeat Western blot and Viral Load

14
Rapid confirmation trial __ ____ _____ _________ __ ____ _____ _________ ______ ________ _______ __ _____ ___ ___ ____________ _______ ______ ________ _______ __ _____ ___ ___ ____________ _______ ______ ___ ________ ______ ___ ________ 15,923 OraQuick tests statewide 363 prelim positive samples to state lab for confirmatory testing 355 Western Blot positive 8 Western Blot negative July 1, 2004 through April 19, 2005

15
2004 NJ Data 363 Specimens at PHEL 8 Negative Western blot 355 Positive Western blot Orasure Oraquick 8 POS 355 POS Trinity UniGold 8 NEG 355 POS Biorad Multispot 7 NEG 1 POS 354 POS 1 QNS MedMira Reveal 8 NEG 340 POS 15 sample interference Follow-up > 2mos 6/6 neg Western blot 6/6 neg viral load

16
Rapid confirmation trial 2004-5 Rapid Testing Evaluation All testing in 2004 involved fingerstick rapid Oraquick HIV testsAll testing in 2004 involved fingerstick rapid Oraquick HIV tests All 8 Western Blot negative clients:All 8 Western Blot negative clients: Negative on follow-up at least 4 weeks later, by both antibody and nucleic acid testingNegative on follow-up at least 4 weeks later, by both antibody and nucleic acid testing 4 of 7 tested reacted with non-viral components of OraQuick device4 of 7 tested reacted with non-viral components of OraQuick device ALL were true Oraquick false positivesALL were true Oraquick false positives

17
A CLIA-waived rapid test matched Western Blot confirmatory results in 100% of the HIV + cases. Every false positive was identified by a proposed rapid confirmation algorithm between 2004-2006! Potential consequences using rapid-rapid confirmation: Eliminate the non-returners Effective sensitivity would approach 99-100% Counseling, contact elicitation and referral for treatment could be Done Immediately In NJ, at least 200 additional HIV + individuals would definitively know their status!! 2004 TAKE HOME MESSAGES:

18
Ability of a Rapid HIV Test to Confirm a Rapid HIV Result January 2006- October 2007 NJ Data Set

19
Jan 2006 – Oct 2007 data BACKGROUND Oral HIV testing had become the predominant means of rapid HIV testing in New Jersey. The rate of discordant results had increased with oral testing METHODS We used retained specimens from follow-up testing of clients that were Rapid Test (+), but Western Blot (-) Testing done on serum Confirmed discordants and indeterminates (if they had follow-up). DID NOT confirm true positives from this data set. Samples were not from the same time as the screening OraQuick. Used CLIA-waived tests ONLY: Repeated OraQuick on blood Trinity Uni-Gold Clearview StatPak
, but Western Blot (-) Testing done on serum Confirmed discordants and indeterminates (if they had follow-up). DID NOT confirm true positives from this data set. Samples were not from the same time as the screening OraQuick. Used CLIA-waived tests ONLY: Repeated OraQuick on blood Trinity Uni-Gold Clearview StatPak.")
20
Follow the data! Total Rapid HIV Testing FingerstickOral Testing NJ Rapid HIV Testing 2005 6 Oral Testing Introduced More False Positive Confirmations

21
Follow-up Information All follow-ups on negative Western Blot specimens were also NAAT negative (i.e.True OraQuick false positive).All follow-ups on negative Western Blot specimens were also NAAT negative (i.e.True OraQuick false positive). All were "second rapid" negative.All were "second rapid" negative. Oral Discordants OraQuick followed by Blood OraQuick:OraQuick followed by Blood OraQuick: 3 tested at CTS site on False Positives:3 tested at CTS site on False Positives: 2 blood negative; 1 blood positive2 blood negative; 1 blood positive 56 tested on follow-up blood specimen56 tested on follow-up blood specimen all were blood negativeall were blood negative SUMMARY: 58 specimens were truly negative; 1 specimen was positiveSUMMARY: 58 specimens were truly negative; 1 specimen was positive Blood Discordants 11 tested on follow-up blood specimen11 tested on follow-up blood specimen 7 negative7 negative 4 repeat positive4 repeat positive

22
Observations Indeterminate Western Blot:Indeterminate Western Blot: 12 total:12 total: 4 no follow-up; 3 QNS4 no follow-up; 3 QNS 3 NAAT negative were "second rapid" negative3 NAAT negative were "second rapid" negative 2 NAAT positive were "second rapid" positive2 NAAT positive were "second rapid" positive

23
2008 Data Randomly sampled serum specimens sent to NJ PHEL some for confirmatory testing; some for standard testing. We didn’t know their identityRandomly sampled serum specimens sent to NJ PHEL some for confirmatory testing; some for standard testing. We didn’t know their identity Ran:Ran: OraquickOraquick UniGoldUniGold StatPakStatPak Discordant – 2 of the 3 rapids agreed – one did notDiscordant – 2 of the 3 rapids agreed – one did not UniGold twiceUniGold twice Oraquick three timesOraquick three times All Pos ALL Neg UniGold Discordant Oraquick Discordant TOTAL 1492623180 Conclusive17597.2% Inconclusive52.8%

24
Potential Issues: Falsely negative 2 nd rapid Frequency 1:180 Falsely positive 2 nd rapid None using Trinity Unigold as the 2 nd rapid Three using StatPak as the 2 nd rapid

25
A second, different rapid HIV test can confirm a preliminary rapid result as reliably as a Western Blot.A second, different rapid HIV test can confirm a preliminary rapid result as reliably as a Western Blot. 98% of time the conclusion will be correct 98% of time the conclusion will be correct 25% of individuals who would never have received their final result will now!!25% of individuals who would never have received their final result will now!! New Jersey will implement rapid-rapid verification and immediate linkage to careNew Jersey will implement rapid-rapid verification and immediate linkage to care Following meetings with Department of Health it was decided to implement rapid-rapid verification statewideFollowing meetings with Department of Health it was decided to implement rapid-rapid verification statewide Conclusions:

27
Implementation PLAN: 3 pilot sites have been identified to begin the ‘roll-out’ 1 site is up, trained and running. The other 2 - within the month Policies, Procedures, Counseling Messages and Forms are completed for the entire system EXPECTATIONS: It will not eliminate Western blot confirmation, BUT it will provide the basis for immediate linkage to care! Less than 1 in 100 will be later removed from care because of a failure to confirm UNKNOWNS: What will be the real world performance of a rapid test in a confirmatory setting? Does reducing the delay really improve the linkage to care? Does post-testing counseling impact positively on prevention messages?

28
Thanks To: RWJMS Evan Cadoff, MD Eugene Martin, Ph.D. Gratian Salaru, MD Sharon Holswade, MBA Franchesca Jackson, BS Nisha Intwala, MT Claudia Carron, RN Lisa May Karen Williams NJDHSS/DHAS Sindy Paul, MD, MPH*Sindy Paul, MD, MPH* Linda Berezny, RNLinda Berezny, RN Maureen Wolski, BSMaureen Wolski, BS Aye Maung MaungAye Maung MaungNJDHSS/PHEL Kenneth EarleyKenneth Earley Kanjana GarciaKanjana Garcia Bruce Wolf, Ph.D.Bruce Wolf, Ph.D. Site coordinators and counselors throughout New Jersey

29
THE END

Similar presentations
 Services at Boston Medical Center Vanessa J. Sasso, MSW Manager, HIV CTR Program Center for HIV/AIDS Care and.>")








 HIV Testing Program using INSTI HIV in an Urban Sexual Health Clinic in Canada Presentation to: 2007 HIV Diagnostics.>")








 within a Pooled HIV Nucleic Acid.>")
