Download presentation
Presentation is loading. Please wait.

1
Update on ADPKD and role of mTOR inhibitors and other agents in its management

2
ADPKD – Introduction Autosomal dominant polycystic kidney disease (ADPKD) - one of the most common inherited disorders in humans Most frequent genetic cause of renal failure in adults Accounts for ~4% of end-stage renal disease (ESRD).
 - one of the most common inherited disorders in humans Most frequent genetic cause of renal failure in adults Accounts for ~4% of end-stage renal disease (ESRD).")
3
Inheritance : Autosomal Dominant Incidence 1 : 700 to 1 : 1000 In India : 10,00,000 cases

4
ADPKD - multisystemic and progressive disorder Characterized by formation and enlargement of cysts in the kidney and other organs (eg, liver, pancreas, spleen) Clinical features usually begin in the third to fourth decade of life, but cysts may be detectable in childhood and in-utero
 Clinical features usually begin in the third to fourth decade of life, but cysts may be detectable in childhood and in-utero")
5
Pathophysiology The main feature of ADPKD is bilateral progressive cystic dilation of the renal tubules, which may lead to end-stage renal disease (ESRD) Hepatic cysts, cerebral aneurysms, and cardiac valvular abnormalities also may occur
 Hepatic cysts, cerebral aneurysms, and cardiac valvular abnormalities also may occur")
6
PATHOGENESIS

8
Modern ADPKD research started when epithelial cell lining the cysts in kidneys of ADPKD patients was successfully isolated and maintained in “ex vivo” cultures.

9
It is observed that cyst cells continue to proliferate, secrete fluid and destroy the surrounding normal tissue by expansion. Cyst fluid contains many hormonal activities including ADH & EGF (Epidermal Growth Factor)
.")
10
The abnormality Approximately 85-90% of patients with ADPKD have an abnormality on the short arm of chromosome 16 (ie, ADPKD type 1 [ADPKD1]) A second defect, termed ADPKD type 2 (ADPKD2), is responsible for 5-15% of ADPKD cases and is found on the long arm of chromosome 4 A third genotype may exist, but no genomic locus is assigned.
![The abnormality Approximately 85-90% of patients with ADPKD have an abnormality on the short arm of chromosome 16 (ie, ADPKD type 1 [ADPKD1]) A second defect, termed ADPKD type 2 (ADPKD2), is responsible for 5-15% of ADPKD cases and is found on the long arm of chromosome 4 A third genotype may exist, but no genomic locus is assigned.](http://images.slideplayer.com/13/4053256/slides/slide_10.jpg "The abnormality Approximately 85-90% of patients with ADPKD have an abnormality on the short arm of chromosome 16 (ie, ADPKD type 1 [ADPKD1]) A second defect, termed ADPKD type 2 (ADPKD2), is responsible for 5-15% of ADPKD cases and is found on the long arm of chromosome 4 A third genotype may exist, but no genomic locus is assigned.")
11
PKD1 and PKD2 expressed in most organs and tissues Proteins encoded by PKD1 and PKD2 - polycystin 1 and polycystin 2 - function together to regulate the morphologic configuration of epithelial cells The polycystins - expressed as early as the blastocyst stage and expressed in a broad array of terminally differentiated tissues The functions of the polycystins have been scrutinized to the greatest extent in epithelial tissues of the kidneys and liver and in vascular smooth muscle.

12
Mortality/Morbidity The major cause of morbidity is progressive renal dysfunctionIn - half of patients with ADPKD undergo renal replacement therapy by age 60 years Cardiovascular pathology and infections account for approximately 90% of deaths of those patients treated by hemodialysis or peritoneal dialysis and after renal transplantation Another cause of mortality is subarachnoidal hemorrhage from intracranial aneurysms (ICAs). This complication is rare and severe.

13
Sex - ADPKD is slightly more severe in males than in females, but it is not statistically significant Age - Symptoms generally increase with age. Children very rarely present with renal failure from ADPKD The mean age of onset of ESRD in patients with ADPKD1 is 53 years; in patients with ADPKD2, it is 74 years.

14
Clinical manifestations Renal - A decrease in urine-concentrating ability is an early manifestation of the disease Microalbuminuria occurs in 35% of patients with ADPKD Patients may develop renal failure, usually in the fourth to sixth decade of life

15
Clinical manifestations – contd. Hypertension is one of the most common early manifestations of ADPKD Pain - located in the abdomen, the flank, or the back, is the most common initial complaint Hematuria - frequently is the presenting manifestation and usually is self-limited Stroke - aneurysm screening with magnetic resonance angiography

16
Physical examination Palpable, bilateral flank masses occur in patients with advanced ADPKD Nodular hepatomegaly occurs in those with severe polycystic liver disease Symptoms related to renal failure (eg, pallor, uremic fetor, dry skin, edema) are rare upon presentation.
 are rare upon presentation.")
17
Diagnosis Renal USG - sensitivity 100% for subjects 30 years or older with a positive family history Diagnostic criteria - two or more cysts in one kidney and at least one cyst in the contralateral kidney in young subjects, but four or more in subjects older than 60 years Most often, the diagnosis is made from a positive family history and imaging studies showing large kidneys with multiple bilateral cysts and possibly liver cysts

18
Diagnosis contd. Before the age of 30 years - CT scan or T2-weighted MRI is more sensitive for detecting presymptomatic disease because the sensitivity of ultrasound falls to 95% for ADPKD type 1 and <70% for ADPKD type 2

19
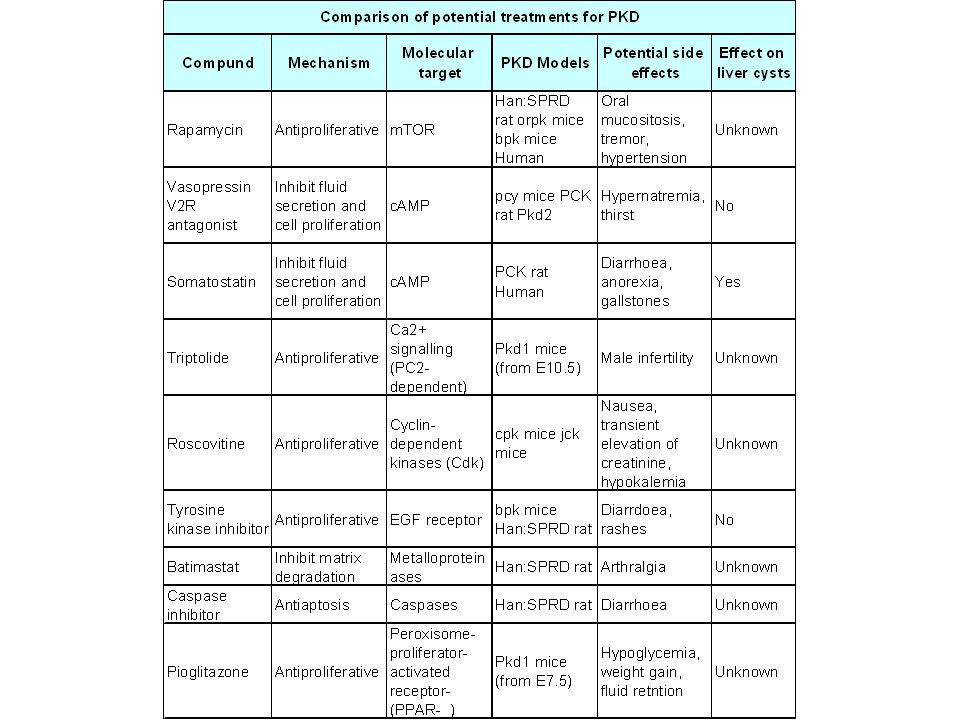
Treatment No specific medication is available for ADPKD However, clinical trials with vasopressin 2 receptor antagonists (Tolvaptan), somatostatin, rapamycin (sirolimus) and some more agents are ongoing At present, treatment is largely supportive, as there is no single therapy that has been shown to prevent the decline in kidney function.
, somatostatin, rapamycin (sirolimus) and some more agents are ongoing At present, treatment is largely supportive, as there is no single therapy that has been shown to prevent the decline in kidney function.")
20
Treatment contd. Hypertension control - target blood pressure of 130/85 or less is recommended Lower levels reported to slow the rate of loss of kidney function A multidrug approach that includes agents to inhibit the renin-angiotensin system is frequently required There is no compelling evidence to recommend a low-protein diet, especially in patients with advanced kidney dysfunction where optimizing nutritional status is important

21
Treatment contd. Lipid-soluble antimicrobials - trimethoprim- sulphamethoxazole and quinolone antibiotics that have good tissue permeation - preferred therapy for infected kidney cysts Pain management - requires cyst drainage by percutaneous aspiration, sclerotherapy with alcohol, surgical drainage Patients with ADPKD appear to have a survival advantage on either peritoneal or hemodialysis compared to patients with other causes of ESRD

22
Treatment contd. Those undergoing kidney transplantation may require bilateral nephrectomy if the kidneys are massively enlarged or have been the site of infected cysts Posttransplantation survival rates are similar to those of patients with other causes of kidney failure, but patients remain at risk for the extrarenal complications of ADPKD.

24
Otsuka Pharmaceutical (basic manufacturer of Tolvaptan) is proceeding with multinational, multicentre, phase III clinical trial to examine the efficacy & safety of Tolvaptan in ADPKD Trials of tolvaptan in humans with ADPKD are ongoing (Ref: Clin Ther. 2010 Jun;32(6):1015-32 ) Approximately 1500 patients will be randomised to either Tolvaptan or Placebo and will be observed for the duration of 5 years TOLVAPTAN
: ) Approximately 1500 patients will be randomised to either Tolvaptan or Placebo and will be observed for the duration of 5 years TOLVAPTAN.")
25
Mechanism of action (V 2 RA) Tolvaptan has been shown to decrease cyst and kidney volume.
 Tolvaptan has been shown to decrease cyst and kidney volume.")
26
Shillingford also observed in a small group of renal transplantation that size of cyst in native ADPKD kidney significally reduced when treated with sirolimus in comparison to CNI. Cincinnati Rapamycin Trial as well as ongoing multicentre trial in UK & US has shown favourable results in cysts of PKD in tuberous sclerosis.

27
Sirolimus therapy in polycystic kidney disease – A pilot study, Nov. 2009 Transplant proceedings A.R. Soliman, E. Ismail, S. Zamil, Cairo university, Egypt.

28
Diagram : dysregulation & accumulation of mTOR in epithelial lining of cyst, which may be final common pathway in cystogenesis.

29
Safety and tolerability of Sirolimus treatment in patients with polycystic kidney Andreas L. Serra, Andreas D. Kistler, Daine Poster et al. Nephrol Dia. Trans (2009) 3334-3342
")
30
Sirolimus reduces polycystic liver volume in ADPKD patients JASN 19, 631-638, 2008 Qian, Hui Du, Bernal F. King et al.

31
Somatostatin has been shown to reduce chloride and fluid secretion in cyst by inhibition of adenylatecyclase & C AMP in epithelial cells of cysts. Mario Negri Institute of Pharmacological research in Italy will enroll 66 ADPKD patients to test the efficacy of long acting somatostatin octreotide LAR. This study will treat patients with an estimated GFR > 40 ml/min./1.73 m 2 and follow the response of therapy by serial MRI over 3 years. SOMATOSTATIN

32
Randomized clinical trial of long-acting somatostatin for autosomal dominant polycystic kidney and liver disease ADPKD(n-34) and ADPLD(n=8). Liver volume decreased by 4.95%+/-6.77% in the octreotide group but remained practically unchanged (+0.92%+/-8.33%) in the placebo group (P=0.048). Among patients with ADPKD, total kidney volume remained practically unchanged (+0.25%+/-7.53%) in the octreotide group but increased by 8.61%+/-10.07% in the placebo group (P=0.045). Changes in GFR were similar in both groups. In summary, octreotide slowed the progressive increase in liver volume and total kidney volume, improved health perception among patients with PLD, and had an acceptable side effect profile Ref: J Am Soc Nephrol. 2010 Jun;21(6):1052-61. Epub 2010 Apr 29
 in the placebo group (P=0.048). Among patients with ADPKD, total kidney volume remained practically unchanged (+0.25%+/-7.53%) in the octreotide group but increased by 8.61%+/-10.07% in the placebo group (P=0.045). Changes in GFR were similar in both groups. In summary, octreotide slowed the progressive increase in liver volume and total kidney volume, improved health perception among patients with PLD, and had an acceptable side effect profile Ref: J Am Soc Nephrol Jun;21(6): Epub 2010 Apr 29.")
34
(R) - Roscovitine (R) – roscovitine is a (R) – sterioisomer of roscovitine. -- Roscovitine is a low molecular weight compound of 2, 6, 9 – tri-substituted purine family. -- 3 week course has long lasting beneficial effect. -- In clinical trials it is well tolerated.

35
(R) – roscovitine is a protein kinase inhibitor with preferenitial selectivity for cyclin dependent kinase (CDKs) Prevents phosphorylation of Rb (retinoblastoma) protein Normalize the level of several cyclins Prevent cell proliferation, transcription and apoptosis Prevents cyst progression.
 – roscovitine is a protein kinase inhibitor with preferenitial selectivity for cyclin dependent kinase (CDKs) Prevents phosphorylation of Rb (retinoblastoma) protein Normalize the level of several cyclins Prevent cell proliferation, transcription and apoptosis Prevents cyst progression.")
36
Mechanism of action (Roscovitine)
")
37
Roscovitine on renal tubular epithelial cell implications for autosomal dominant polycystic kidney disease The cyclin kinase inhibitor roscovitine has shown efficacy in treatment of murine PKD Renal tubular epithelial cells exposed to 'low' concentrations of roscovitine showed minimal apoptosis in association with markedly increased levels of the antiapoptotic protein p21 Data in this study provide a mechanistic explanation of how roscovitine is effective in PKD Ref: Am J Nephrol. 2009;29(6):509-15. Epub 2008 Dec 10
: Epub 2008 Dec 10.")
38
TRIPTOLIDE Natural Chinese herbal compound. Restores intracellular Ca 2+ regulation in cyst lining cells Thus inhibits c-AMP dependent cell proliferation and water secretion.

39
Triptolide reduces cyst formation in a neonatal to adult transition Pkd1 model of ADPKD Daily injections with triptolide significantly reduced the total number of cysts per kidney, with a pronounced effect on the number of microcysts and the overall cystic burden Additionally, renal function as assessed by blood urea nitrogen levels was also improved in triptolide-treated mice These results suggest that the model of ADPKD is amenable to short-term kidney cyst formation drug studies Ref: Nephrol Dial Transplant. 2010 Jul;25(7):2187-94. Epub 2010 Feb 4
: Epub 2010 Feb 4.")
41
How to monitor the therapeutic efficacy in ADPKD. -Very slowly progressive disease. -Initially GFR remains stable. -Once when Serum Creatinine exceeds normal value GFR declines 5 ml/min/yr, leading to ESRD within 10 years. However individual variability is substantial.

42
Consortium for Radiologic Imaging studies of PKD (CRISP) followed 241 ADPKD patients by sequential MRI measurement of cyst & renal volumes. According to them, Volumetric kidney measurements by MRI is the gold standard to determine disease progression. They also observed that Renal & cyst volumes correlated inversely with GFR and directly to hypertension and urinary albumin excretion. Average annual increase in renal volume was 5.3%. Cyst growth was more aggressive in young or who had large renal volume at the time of diagnosis.

43
Is it time to start clinical trials in ADPKD ? Of course Yes.. ADPKD patients have waited enough & suffered enough to find a cure of their disease so any measure to halt the progression of disease is highly warranted.

44
Phase I/II study is initiated by the cleveland clinic which will enroll a total of 45 patients and monitor the changes in iothalamate, GFR and total kidney volume measured by CT over the period of 12 months. The patients will be divided into 3 groups. Control (15), low dose of sirolimus (15) (trough blood level 2-5 ng/ml) and high dose of sirolimus (15) (trough blood level 5-8 ng/ml.).
, low dose of sirolimus (15) (trough blood level 2-5 ng/ml) and high dose of sirolimus (15) (trough blood level 5-8 ng/ml.)..")
45
Other trial will treat 300 ADPKD patients with everolimus. It has been started in Germany and Austria and will follow ADPKD patients with estimated GFR between 30 to 89 ml/min/1.73m 2 (CKD stage II & III) for 2 years by repeated MRI. Dose is the same as given in organ transplantation.
 for 2 years by repeated MRI. Dose is the same as given in organ transplantation..")
Similar presentations

















![Case Report # [] Submitted by:Kandra Vogt, MSIV Faculty reviewer:Sandra A. A. Oldham, M.D. Date accepted:31 August 2007 Radiological Category:Principal.](/18/5671912/big_thumb.jpg "Case Report # [] Submitted by:Kandra Vogt, MSIV Faculty reviewer:Sandra A. A. Oldham, M.D. Date accepted:31 August 2007 Radiological Category:Principal.>")





