Download presentation
Presentation is loading. Please wait.

1
Sport and Dental Injuries

3
History Mr B.S. is a 25 year old male soccer player. He sustained oral injuries involving teeth while playing a tournament as a striker. He played same position since the age of 13. No significant medical history. He was once treated for stress fracture of the tibia. Non-smoking and does not take alcohol at all.

4
Clinical examination General Examination: GCS 15/15. Bleeding from the mouth plugged in cotton wool and gauze. Wt 78 kg Ht 1.76 m BMI 25. BP 117/74 mmHg Pulse 96 b/m SaO2 100 % in room air. Oral Examination: Bleeding penetrating wound of the upper and lower lips. Two upper central incisors broken and loose from the gums. Tongue not injured.

6
Further Management Wound cleaned. ATT 0.5 ml imi stat. IV 1L Lactated Ringers. Kefzol 1g ivi stat. Local anesthetic agent given. Laceration sutured in 3 layers i.e. Chromic 4/0 mucosa & subcutaneous tissue and Nylon 6/0 on the skin. Good haemostasis achieved. Skull and Cervical spine X-rays normal.

9
Further Management continued Dental consultation: Extraction of loose incisors and permanent false teeth later. Analgesics given for 5 days. Removal of Nylon 6/0 sutures in 9 days with good wound union. Player cleared for full contact sport after 6 weeks but with a gum shield on.

11
Biopsychosocial Assessment Patient worried about deformity of his mouth and oral re-injury especially playing as a striker who is more prone to collision injuries. This would have a negative impact to his performance which will affect his team selection. The scar above his upper lip which affects him cosmetically.

12
Discussion Dental injuries are orofacial injuries of traumatic nature. High risk sports for dental injuries namely baseball, basketball, softball, volleyball, gymnastics, wrestling and soccer lag behind in mandatory protective equipments. Incidence of dental trauma compared to all accidents in contact sports is 2% to 33%. Damage or loss of teeth has future economic and psychological implications.

13
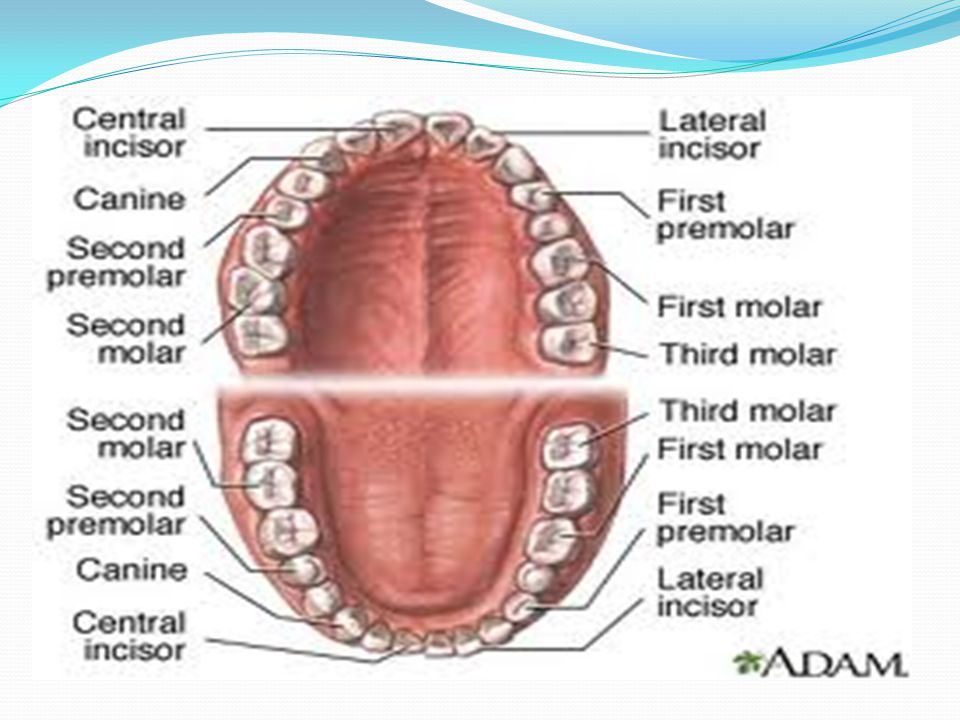
Disussion continued Parents, teachers, coaches and everybody should assist in curbing dental injuries. 2/3 of dental injuries tend to occur during competitive matches compared to 1/3 during training sessions. The majority of sport-related dental and orofacial injuries affect the upper lip, maxilla and maxillary incisors. 50% to 90% of dental injuries involving maxillary incisors.

14
Discussion continued Significant differences between number of teeth injured and the causes of injury. A blow or kick from another player often causes injury to one tooth. A blow from hard object most often causes injury to > 1 tooth. Damage can also result in facial bone fracture and neck or brain injury resulting in increased ICP and deformation.

15
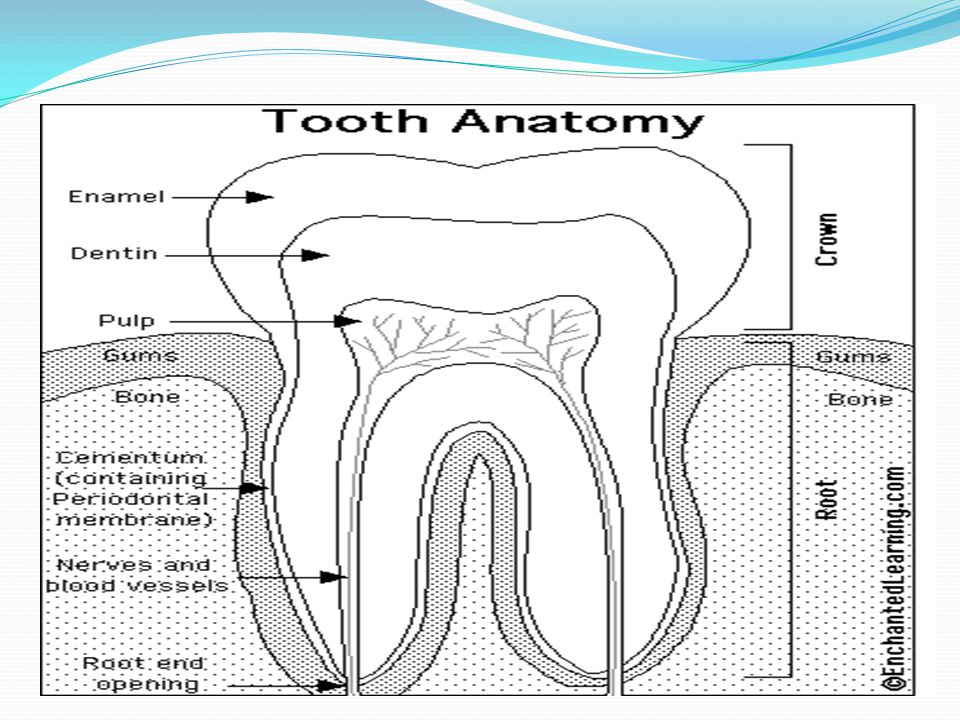
Discussion continued Traumatic injuries to the oral cavity: 1) Teeth: Crown fractures Dental crown fractures frequently affects permanent teeth, mostly maxillary central incisors. Due to direct high-velocity trauma. Good lip coverage diffuses the force and distributes the impact energy over a wider area.

16
Crown fractures: Enamel Enamel infraction or crack usually extends to the dentin-enamel junction, diagnosed by sensitivity to temperature, sweets or biting pressure. Bonding restorations can arrest the progression of enamel infraction. Enamel fracture with loss of enamel substance can be restorated with acid-etch bonding of composite for aesthetics. Oral cavity, lips and tongue should be routinely examined for tooth fragments.

17
Crown fractures: Dentin and Pulp Adequate pulpal protection and acid-etch composite restoration is therapeutic to dentin fracture. Tooth fragments can also be helpful to restore the tooth in perfect aesthetic way. Sensitivity to hot, cold and sweets over a time period of 6 to 8 weeks is diagnostic of crown fractures involving the pulp. Pulpal protective treatment by calcium hydroxide prevents infection.

18
Crown fractures: Pulp The fracture will lead to either a proliferative or destructive response if not treated. Bacterial infection will necessitate pulpotomy (removal of inflamed pulpal tissue) or pulpectomy and root canal therapy. In case of immature teeth, it is essential that pulpal cavity is maintained to allow completion of root development. Complications are internal resorption and pulpal necrosis.
 or pulpectomy and root canal therapy. In case of immature teeth, it is essential that pulpal cavity is maintained to allow completion of root development. Complications are internal resorption and pulpal necrosis..")
20
Crown fractures: Pulp Signs of successful pulp capping and pulpotomy are absence of pain, negative percussion, normal thermal sensitivity, absence of radiographic periapical pathosis and radiographic evidence of continued root development. Pulpal vitality to be monitored at 1, 3 and 6 months post trauma. Thereafter every 6 months for several years. Pain, palpation, percussion and X-rays are more indicative than electrical and thermal pulp tests.

22
Crown fractures: Root Uncomplicated – involving enamel, dentin and cementum. The tooth can be restored by bonding of crown. Complicated – involving enamel, dentin, cementum and pulp. This requires root canal therapy so that a post and crown may be incorporated. The coronal fragment more than 1/3 of the clinical root length and vertical root fractures are indicative of tooth extraction.

23
Root fractures Occur in 7% or fewer of permanent teeth injuries. Most remain vital but 20-40% become non-vital. Diagnosis confirmed by percussion, sensitivity to biting pressure, mobility and X-ray evidence. Prompt reduction and fixation with a rigid acid- etched splint for 3 to 6 months. This promotes healing by calcific callus formation internally on the root canal and externally on the root surface.

24
Periodontal tissues Non-displacement injuries: Characterized by edema, bleeding and trauma to periodontal ligament fibres. Sensitivity to biting pressure, percussion and palpation, so a relief of the occlusion and a soft diet is recommended. X-ray follow-up evaluation for one year is advisable to rule out the need for endodontic therapy.

25
Periodontal tissues Displacement injuries: Low-velocity trauma (primary teeth> permanent). Swelling, discoloration of the crown, mobility or change in their occlusion. 50% 0f affected permanent teeth will require root canal therapy. Pulpal necrosis, root resorption, pulp calcification & obliteration and loss of alveolar crestal height are major complications.

26
Periodontal tissues Splinting time for luxated teeth can range between 2 to 3 weeks, depending on the severity of the injury. When two or more neighbouring teeth are able to be moved jointly as a block, the alveolar bone is fractured. Intrusion: The highest incidence of pulpal necrosis (96%). Mature teeth should be treated by orthodontic extrusion back into position.
. Mature teeth should be treated by orthodontic extrusion back into position..")
27
Periodontal tissues Avulsion: Complete displacement of the tooth from its socket. Mostly affects maxillary central incisors. The sooner an avulsed tooth is replanted, the better its chances of survival. Immature teeth with incomplete root formation have a potential to revitalize and survive. Avulsed tooth should be transported in normal saline or cold pasteurized milk in an emergency.

28
Periodontal tissues Avulsed tooth should never be stored intraorally to avoid aspiration or swallowing and bacterial contamination by saliva. A tooth allowed to dry will lead to periodontal ligament necrosis with replacement resorption (ankylosis) or inflammatory resorption (external root resorption). Infection prevention is also a good to initiate immediate antibiotic therapy after replantation. ATT for those who have not been immunized.
 or inflammatory resorption (external root resorption). Infection prevention is also a good to initiate immediate antibiotic therapy after replantation. ATT for those who have not been immunized..")
29
Periodontal tissues Revascularization is a possibility in replanted immature teeth with open apices. Conversely untreated avulsed teeth with mature roots always develop pulpal necrosis and external root resorption. These teeth must be monitored closely for signs of degeneration. Replanted teeth undergo gradual ankylosis and are capable of functioning for many years.

30
Prevention of sports-related dental injuries

31
Mouthguard / gumshield / mouth protector. Protective, comfortable, resilient, tear-resistant, odourless, tasteless, affordable/cheap, easy to fabricate and no interference with speech. Dentist fitted mouthguards are better. OTC mouthguards not safe. Properly fitted mouthguard can reduce the sports-related dental injuries by 60%. Prevention of sports-related dental injuries

32
Mouthguard is widely regarded as being the most effective way of preventing such injuries. Protection from hard- and soft-tissue injuries. Also reduce incidence of concussion by reducing the ICP & the force of impact to the brain as a result of blow to the chin. This is achieved by increasing the space between the head of the condyle and mandibular fossa of the cranium.

33
Take Home Message Sports-related dental injuries can have financial and psychological consequences to everyone involved. Urgent referral to dentist is very important to prevent more lifelong complications. Use of mouthguards can reduce incidence of these injuries especially if fitted well by dentist.

34
References 1) American Academy of Paediatric Dentistry. Policy on Prevention of Sports-related Orofacial Injuries 2010;63-64. 2) Newsome PRH. The role of the mouthguard in the prevention of sports-related dental injuries. ISMJ 2003;4(1):1-4. 3) Schulze A. Dental traumatic injuries in sports accidents. Clinical Sports Medicine International (CSMI) 2008;1(8):13-15.
 Newsome PRH. The role of the mouthguard in the prevention of sports-related dental injuries. ISMJ 2003;4(1):1-4. 3) Schulze A. Dental traumatic injuries in sports accidents. Clinical Sports Medicine International (CSMI) 2008;1(8):")
Similar presentations









>")














