Download presentation
Presentation is loading. Please wait.

1
Post Graduate student in Community Medicine(M.D) Department of Community Medicine / SRMC & RI (DU ) INDIAN RAILWAY MEDICAL SERVICE B.Sc., M.B.B.S., D.P.H., D.I.H.,PGCH&FW(NIHFW) INDIA
 Department of Community Medicine / SRMC & RI (DU ) INDIAN RAILWAY MEDICAL SERVICE B.Sc., M.B.B.S., D.P.H., D.I.H.,PGCH&FW(NIHFW) INDIA")
12
MAJOR CAUSES OF M.M.R DIRECT CAUSES HEMORRHAGE – 29.6% PUERPERAL COMPLICATION – 16.1% OBSTRUCTED LABOUR – 9.5% ABORTIONS – 8.9% TOXAEMIA OF PREGNANCY 8.3% INDIRECT CAUSES Anaemia Pregnancy with TB Pregnancy with malaria Pregnancy with viral hepatitis

15
DISPARITY OF MATERNAL DEATH BETWEEN DEVELOPED & DEVELOPING COUNTRIES BARRIER TO RECEIVE TIMELY & GOOD QUALITY CARE BARRIER OF AVAILABILITY AND ACCESSIBILITY OF SERVICES POLITICAL BARRIER GEOGRAPHICAL BARRIER CULTURAL BARRIER WOMEN’S LITERACY AND WOMEN EMPOWERMENT TIME BARRIER ECONOMIC BARRIER BARRIER TO HAVE HEALTH PERSONNEL AT GRASS ROOT LEVEL

17
RCH – Ι PROGRAMME 15.10. 1997

18
Objectives · Reduction of Maternal Morbidity and Mortality (MMR) · Reduction of Infant Morbidity and Mortality (IMR) · Reduction of Under 5 Morbidity and Mortality (U5MR) · Promotion of adolescent health · Control of reproductive tract infections and sexually transmitted infections.
 · Reduction of Infant Morbidity and Mortality (IMR) · Reduction of Under 5 Morbidity and Mortality (U5MR) · Promotion of adolescent health · Control of reproductive tract infections and sexually transmitted infections.")
19
The first phase of the programme had started from 1997 To bring down the birth rate below 21 per 1000 population To reduce the infant mortality rate below 60 per 1000 life born To bring down the maternal mortality rate below 400 per one lakh. Eighty per cent institutional delivery, 100 per cent antenatal care and 100 per cent immunization of children

24
COMPONENTS OF RCH PROGRAMME Prevention and management of unwanted pregnancy Maternal care that includes antenatal, delivery, and postpartum services Child survival services for newborns and infants Management of reproductive tract infections and sexually transmitted infections

25
REPRODUCTIVE HEALTH ELEMENTS Responsible and healthy sexual behaviour Intervention to promote safe motherhood Prevention of unwanted pregnancy To increase accessibility of contraceptives Safe abortions Pregnancy and delivery services Management of RTI/STD Referral facility by government/private sector for pregnant women at risk Reproductive health services for adolescents Screening and treatment of infertility, cancer & other gynecological disorders

26
CHILD SURVIVAL ELEMENTS Essential New Born Care Prevention and management of vaccine preventable disease Urban measles campaign Neonatal tetanus elimination Surveillance of vaccine preventable diseases Cold chain system Polio eradication : pulse polio programme ARI control programme Diarrhea control programme and ORS programme Prevention and control of Vitamin A deficiency among children Baby Friendly Hospital Initiative (BFHI)
")
27
STRATEGY BOTTOM-UP PLANNING COMMUNITY NEED ASSESSMENT APPROACH DECENTRALISED PARTICIPATORY PLANNING & IMPLEMENTATION STRENGTHENING INFRASTUCTURE INTEGRATED TRAINING PACKAGE IMPROVED MANAGEMENT SYSTEM INTERVENTIONS MONITORING & EVALUATION

28
ANTE NATAL CARE Early registration of pregnancies (12 – 16 weeks) Minimum 3 antenatal visits (20,32,36 weeks) check- ups Anaemia prophylaxis ( Iron and Folic acid tablets) Two doses of TT Minimum investigations( Weight, B.P,Blood group, Rh typing, Urine examination,VDRL,HIV (TRIDOT TEST) Identification of high risk group, Early detection of complication of pregnancy & timely, safely referral to FRU Treatment of worm infestation with Mebendazole Health education on diet, breast feeding, care of breast, personnel hygiene during pregnancy,& family planning
 Minimum 3 antenatal visits (20,32,36 weeks) check- ups Anaemia prophylaxis ( Iron and Folic acid tablets) Two doses of TT Minimum investigations( Weight, B.P,Blood group, Rh typing, Urine examination,VDRL,HIV (TRIDOT TEST) Identification of high risk group, Early detection of complication of pregnancy & timely, safely referral to FRU Treatment of worm infestation with Mebendazole Health education on diet, breast feeding, care of breast, personnel hygiene during pregnancy,& family planning")
30
COMPLICATIONS DURING ANTE-NATAL, INTRA NATAL, AND POST NATAL PERIOD & WHERE TO REFER COMPLICATIONS AVERAGE TIME FROM ONSET TO DEATH INSTITUTION TO WHICH TO BE REFRRED 1.APH 2.PPH 12 HRS 2 HRS FIRST LEVEL REFERAL CENTER SEVERE TOXAEMIA 2 DAYSPHC/CHC RUPTURED UTERUS 24 HRSFLRC OBSTRUCTED LABOUR 3 DAYSFLRC SEPSIS ( AFTER ABORTION, DELIVERY) 6 DAYSPHC/ CHC/FLRC SEVERE ANAEMIA ( CHF IN LABOUR) 2 HRS TO 1 DAYFLRC
 6 DAYSPHC/ CHC/FLRC SEVERE ANAEMIA ( CHF IN LABOUR) 2 HRS TO 1 DAYFLRC")
31
PACKAGES OF SERVICES AT FRU VACCUM EXTRACTIONS ADMINISTRATION OF ANAESTHESIA BLOOD TRANSFUSION CASEAREAN SECTION MANUAL REMOVAL OF PLACENTA CARRY OUT SUCTION CURETTAGE FOR INCOMPLETE ABORTION INSERTION OF INTRAUTERINE DEVICES STERILIZATION OPERATION

32
TYPES OF KIT for FRU Kit-E – Laparotomy set Kit-F - Mini– Laparotomy set Kit-G – IUD insertion set Kit-H – Vasectomy set Kit- I – Normal delivery set Kit- J – Vacuum extraction set Kit- k – Embryotomy set Kit- L – Uterine evacuation set Kit-M – Equipment for anesthesia Kit-N- Neonatal resuscitation set Kit-O- Equipment and reagent for blood test Kit-P – Donor blood transfusion set

33
INTRANATAL CARE Delivery by trained personnel (100%) Institutional delivery (80%) Care at birth ( Five cleans: Clean Birth Canal,Clean surface for delivery,Clean Hands,Clean Cutting, & Clean Cord)
 Institutional delivery (80%) Care at birth ( Five cleans: Clean Birth Canal,Clean surface for delivery,Clean Hands,Clean Cutting, & Clean Cord)")
34
POST NATAL CARE 3 post natal check-ups of mothers after delivery Breast feeding – early & exclusive breast feeding Spacing – minimum 3 years between two pregnancies

35
NEW STRATEGY EMPOWERED ACTION GROUP HAS BEEN CONSITUTED ON 20.03.2001 TRAINING OF DAIS IN 156 DISTRICTS 18 STATES/UTs 2001-2002 RCH CAMPS & RCH OUT REACH SCHEME GADCHIROLI MODEL TO TAKE CARE OF HOME BASED NEONATEL CARE IN 2002 KANGAROO MOTHER CARE TO TAKE CARE OF LOW BIRTH WEIGHT INFANTS BORDER DISTRICT CLUSTER STRATEGY – 49 DISTRICTS/17 STATES INTEGRATED MANAGEMENT OF CHILDHOOD ILLNESS STRATEGY TO TAKE CARE OF SICK NEWBORNS

39
ACHIVEMENT OF H & FW INDICATORS IN TAMILNADU( 1997-2002) LIFE EXPECTANCY AT BIRTH – 65 CRUDE BIRTH RATE – 19.2 CRUDE DEATH RATE – 7.9 NATURAL GROWTH RATE – 1.1 INFANT MORTALITY RATE – 51 UNDER FIVE MORTALITY RATE – 15.1( R )9.7( U ) MATERNAL MORTALITY RATE – 1.3 TOTAL FERTILITY RATE – 1.95 COUPLE PROTECTION RATE – 51.6 MEAN AGE AT MARRIAGE – 21.2 ANTE NATAL CARE – 98.5% POST NATAL CARE – 90% INSTITUTIONAL DELIVERY – 87.6% DELIVERY BY TRAINED STAFF – 98% PNMR –43/1000 NNMR – 38/1000 % OF LOW BIRTH WEIGHT BABIES –17% AVERAGE BIRTH WEIGHT OF BABIES – 2.7 KG STILL BIRTH RATE – 11.7/1000 IMMUNIZATION COVERAGE –100%
 LIFE EXPECTANCY AT BIRTH – 65 CRUDE BIRTH RATE – 19.2 CRUDE DEATH RATE – 7.9 NATURAL GROWTH RATE – 1.1 INFANT MORTALITY RATE – 51 UNDER FIVE MORTALITY RATE – 15.1( R )9.7( U ) MATERNAL MORTALITY RATE – 1.3 TOTAL FERTILITY RATE – 1.95 COUPLE PROTECTION RATE – 51.6 MEAN AGE AT MARRIAGE – 21.2 ANTE NATAL CARE – 98.5% POST NATAL CARE – 90% INSTITUTIONAL DELIVERY – 87.6% DELIVERY BY TRAINED STAFF – 98% PNMR –43/1000 NNMR – 38/1000 % OF LOW BIRTH WEIGHT BABIES –17% AVERAGE BIRTH WEIGHT OF BABIES – 2.7 KG STILL BIRTH RATE – 11.7/1000 IMMUNIZATION COVERAGE –100%")
42
RCH - II PROGRAMME 01-04-2005

43
THE 5 YEAR PHASE OF RCH II VISION To bring about outcomes as envisioned in the 1. Millennium Development Goals 2. The National Population Policy 2000 (NPP 2000)Goals 3. The Tenth Plan Goals 4. The National Health Policy 2002 5. and Vision 2020 India
Goals 3. The Tenth Plan Goals 4. The National Health Policy and Vision 2020 India.")
45
1728 - FRU PHC - 22928 SUB CENTER- 38044

46
1. MATERNAL HEALTH a) 260 Primary Health Centres are proposed to be taken up for improving access to Essential Obstetric and New Born Care services round the clock in TN. All CHC, & 50% PHCs to be made functional for 24 hrs delivery services,& 2000 FRU are proposed b) Improving quality of antenatal, neonatal and postnatal care by providing increased number of antenatal checkups, fixed day antenatal clinics, linking visits of neonates with postnatal care, empowering the VHNs in performing obstetric first aid and newborn care. c) Improvement of the referral networking systems by establishing emergency help line. d) Regular conduct of blood donation camps for the continued availability of blood in the blood banks. e) Universalizing the concept of birth companionship during the process of labour in all health facilities conducting deliveries. f) Operationalisation of maternal death audit to address the issues that have led to maternal deaths.
 260 Primary Health Centres are proposed to be taken up for improving access to Essential Obstetric and New Born Care services round the clock in TN. All CHC, & 50% PHCs to be made functional for 24 hrs delivery services,& 2000 FRU are proposed b) Improving quality of antenatal, neonatal and postnatal care by providing increased number of antenatal checkups, fixed day antenatal clinics, linking visits of neonates with postnatal care, empowering the VHNs in performing obstetric first aid and newborn care. c) Improvement of the referral networking systems by establishing emergency help line. d) Regular conduct of blood donation camps for the continued availability of blood in the blood banks. e) Universalizing the concept of birth companionship during the process of labour in all health facilities conducting deliveries. f) Operationalisation of maternal death audit to address the issues that have led to maternal deaths..")
47
INFANT AND CHILD HEALTH a. Reduction of new-born deaths, infant deaths and child deaths by providing continuous health care and strengthening of new-born care infrastructure facilities. b. Organizing counselling sessions for the mothers. c. Implementing integrated management of neonatal and childhood illness as a pilot initiative in selected districts in Tamil Nadu. d. Operationalising infant death/stillbirth verbal autopsy. e. Addressing the issue of female infanticide and foeticide.

48
3. ADOLESCENT HEALTH. a) Focusing adolescents as receivers and providers of knowledge and function as link volunteers in the community. b) Utilising the services of trained adolescents for propagating Indian System of Medicines. c) Broadcasting and Telecasting of programme by AIR/TV focusing adolescent, gender and health related subjects. d) Formation of co-ordination committee at the district level and monitoring committee at the State level for overseeing the AIR/TV programme.
 Focusing adolescents as receivers and providers of knowledge and function as link volunteers in the community. b) Utilising the services of trained adolescents for propagating Indian System of Medicines. c) Broadcasting and Telecasting of programme by AIR/TV focusing adolescent, gender and health related subjects. d) Formation of co-ordination committee at the district level and monitoring committee at the State level for overseeing the AIR/TV programme..")
49
a)While sustaining the ongoing family welfare interventions in all districts, 19 districts with Higher order births will be targeted for intensified interventions. b) Social marketing programme for condom and other health commodities, promotion of IUD insertions, familiarizing the concept of one-stop Family Welfare Centre. c) Increasing access to safe abortion services by popularising manual vacuum aspiration (MVA) technique. d) Establishment of one-stop family welfare services at Comprehensive Emergency Obstetric and New Born Care (CEMONC) Centres. e) Popularizing No Scalpel Vasectomy. FAMILY WELFARE
 Social marketing programme for condom and other health commodities, promotion of IUD insertions, familiarizing the concept of one-stop Family Welfare Centre. c) Increasing access to safe abortion services by popularising manual vacuum aspiration (MVA) technique. d) Establishment of one-stop family welfare services at Comprehensive Emergency Obstetric and New Born Care (CEMONC) Centres. e) Popularizing No Scalpel Vasectomy. FAMILY WELFARE.")
50
5. Reproductive tract infections / Sexually transmitted infections / Cancer control. a) Establishment of Reproductive Tract Infection / Sexually Transmitted Infection, early Cancer detection clinics. b) Strengthening RCH outreach services. c) RTI/STD clinic in selected 70 primary health centers
 Establishment of Reproductive Tract Infection / Sexually Transmitted Infection, early Cancer detection clinics. b) Strengthening RCH outreach services. c) RTI/STD clinic in selected 70 primary health centers.")
51
Infrastructure strengthening for service delivery a) Construction of HSC buildings where HSCs are currently functioning in rented premises b) Rebuilding HSCs which are unfit for occupation. c) Taking up of repairs/renovation and provision of water supply/electrical works to PHCs/HSCs. d) Need-based supply of equipment/furniture to the HSCs and PHCs as per the standard list including gas connections. e) Provision of Cell phones to HSCs where large number of deliveries take place. f) Provision of telephones to PHCs
 Taking up of repairs/renovation and provision of water supply/electrical works to PHCs/HSCs. d) Need-based supply of equipment/furniture to the HSCs and PHCs as per the standard list including gas connections. e) Provision of Cell phones to HSCs where large number of deliveries take place. f) Provision of telephones to PHCs.")
52
TRAINING a) Skill upgradation training with focus on improving/upgrading the skills of health care providers. b) Integrated skill training for peripheral health functionaries such as VHNs, SHNs, medical officers and health inspectors. c) Improving managerial and communication skills of health staff.
 Integrated skill training for peripheral health functionaries such as VHNs, SHNs, medical officers and health inspectors. c) Improving managerial and communication skills of health staff..")
53
BEHAVIOURAL CHANGE COMMUNICATION (BCC) a) Social mobilisation activity against female infanticide and foeticide by preventive counselling. b) Formation of HSC, Block, District level committees for saving female babies. c) Conducting of Kalaipayanam (travelling street theatre) to promote social mobilization and to improve health care among the target population d) Telecasting of TV serials, Radio broadcasts, wall paintings, hoardings and glow signs for popularizing health and reproductive health messages in important places.
 Formation of HSC, Block, District level committees for saving female babies. c) Conducting of Kalaipayanam (travelling street theatre) to promote social mobilization and to improve health care among the target population d) Telecasting of TV serials, Radio broadcasts, wall paintings, hoardings and glow signs for popularizing health and reproductive health messages in important places..")
54
HEALTH MANAGEMENT INFORMATION SYSTEMS Introduction of IT-enabled HMIS for planning and monitoring health services at the State/District /Block levels STRENGTHENING OF TEACHING INSTITUTIONS Strengthening the facilities at teaching institutions for providing optimum obstetric, family welfare, neonatal child health services. ESTABLISHING URBAN HEALTH POSTS To provide an integrated and sustainable system for primary health care service delivery catering to the requirements of urban slum population and other vulnerable groups

55
HEALTH FINANCING The health care expenditure in India currently stands at 6.1% of GDP. The private out of pocket expenditure being 4.7% of Gross Domestic Product (GDP). The total government expenditure on family welfare has shown an increasing trend from 4.9 billion in fifth plan (1974-79) to Rs. 271.25 billion in the tenth plan (2002-07)
. The total government expenditure on family welfare has shown an increasing trend from 4.9 billion in fifth plan ( ) to Rs billion in the tenth plan ( ).")
56
ACCESSIBILITY INDICATOR No. of eligible couples registered/ANM No. of Antenatal Care sessions held as planned % of sub Centers with no ANM % of sub Centers with working equipment of ANC % ANM/TBA without requisite skill % sub centers with DDKs % of sub centers with infant weighing machine % subcenters with vaccine supplies % sub centers with ORS packets % sub centers with FP supplies

57
QUALITY INDICATOR % Pregnancy Registered before 12 weeks % ANC with 5 visits % ANC receiving all RCH services % High risk cases referred % High risk cases followed up % deliveries by ANM/TBA %PNC with 3 PNC visits % PNC receiving all counselling % PNC complications referred % Eligible couple offered FP choices % women screened for RTI/STDs % Eligible couple counselled for prevention of RTI/STDs % ADD given ORS % ARI treated % children fully immunized

58
IMPACT INDICATOR % DEATHS FROM MATERNAL CAUSES MATERNAL MORTALITY RATIO PREVALENCE OF MATERNAL MORBIDITY % LOW BIRTH WEIGHT NEO-NATAL MORTALITY RATIO PREVALENCE OF POST NATAL MATERNAL MORBIDITY % BABY BREAST FEED WITHIN 6 HRS OF DELIVERY COUPLE PROTECTION RATE PREVALENCE OF TERMINAL METHOD OF STERILIZATION PREVALENCE OF SPACING METHOD % ABORTION RELATED MORBIDITY PREVALENCE OF ADD PREVALENCE OF ARI PREVALENCE OF RTI/STDs

59
THANK YOU

Similar presentations










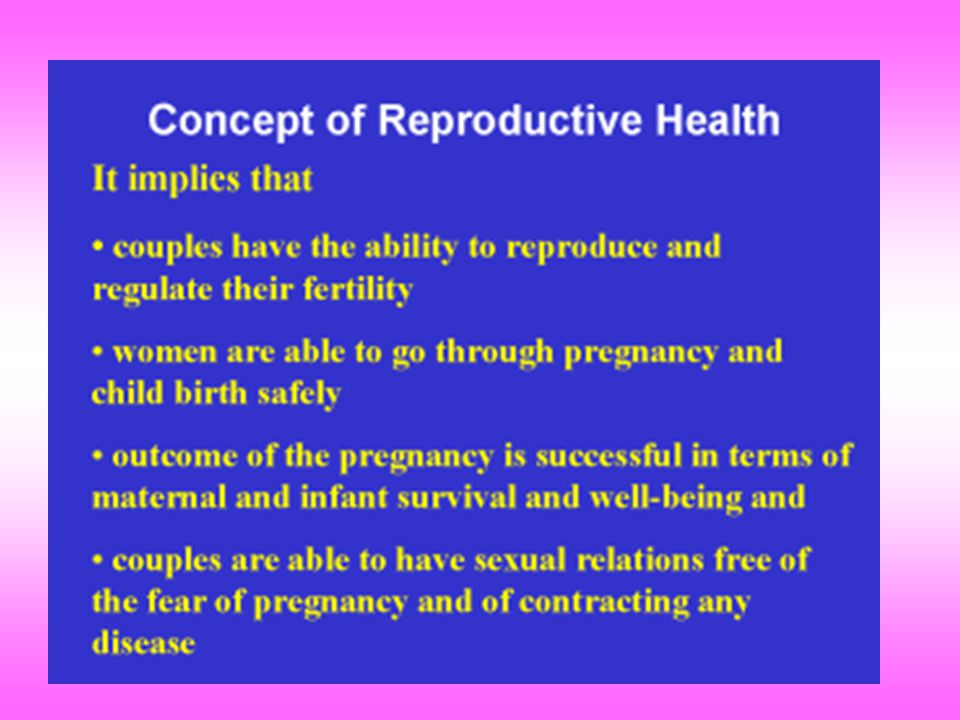















. ▪ Programme launched on 15 th October 1997 ▪ ‘People have the ability to reproduce and regulate their fertility,>")









>")



