Download presentation
Presentation is loading. Please wait.

1
Failed Intubation in Children Dr Philip Ragg Royal Children’s Hospital Melbourne

2
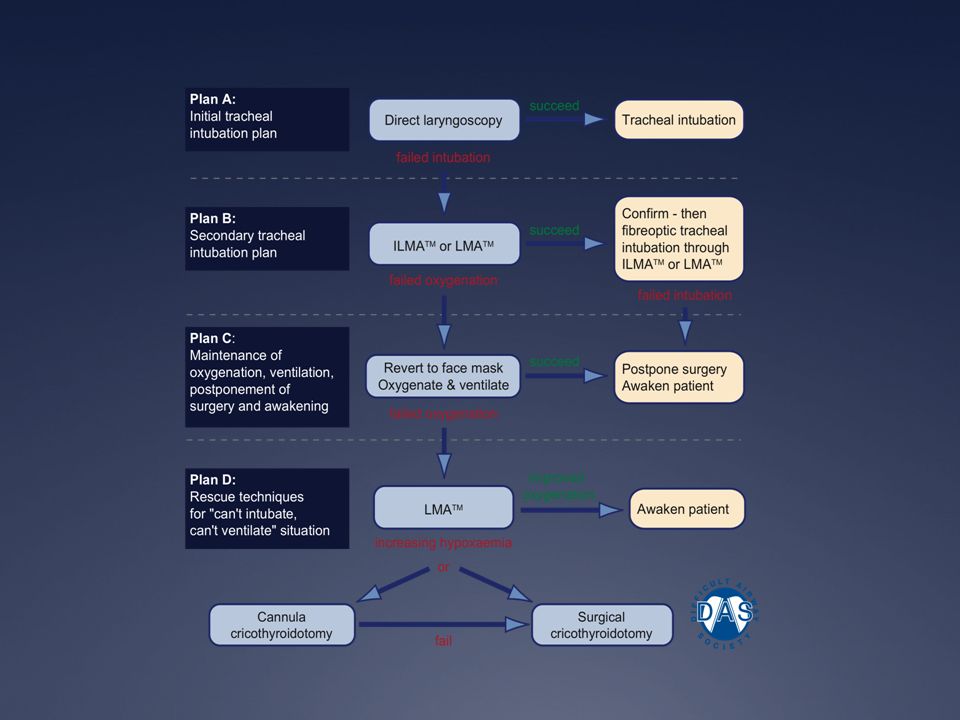
Difficult Airway Management Explosion of interest in airways NAP-4 Guidelines 2011 “Difficult Airway Society” Algorithms Video-laryngoscopes on the scene Very little guidance for Paediatrics!!

3
APLS 2011 5 th Edition Recommendations If intubation is impossible or unsuccessful consider: needle cricothyroidotomy ONLY if 12 yrs Un-referenced

4
Structured Approach to Airway Management Basic Manoeuvres Adjuncts Intubation Surgical Airway Clear, appropriate, logical sequence

5
Paediatric Scenarios for The Failed Intubation Anticipated Failure due to Difficult Airway Un-anticipated Failure (rare with experience) ! Complicating Factors: Time available (stable patient, oxygenating, fasted) No Time available (deteriorating, hypoxic, un-fasted) Walker RWM, Ellwood J. Paed Anesth. Review Article 2009:19;77-87
 No Time available (deteriorating, hypoxic, un-fasted) Walker RWM, Ellwood J. Paed Anesth. Review Article 2009:19;")
6
Golden Rules for Any Intubation First - Assess the airway Know your skill level Always have a plan B Any problem at any time - Call for help early Prepare your equipment, environment, drugs Optimize the patients position OXYGENATION as Number 1 priority

7
Anticipated Failure to Intubate Reasons may be: Congenital or Acquired Acute or Chronic Supra or Subglottic Examples include: Syndromes (Pierre Robin, Treacher Collins, Goldenhar) Burns or Scarring or Trauma to face Haemangiomas Epiglotittis or Croup etc.
 Burns or Scarring or Trauma to face Haemangiomas Epiglotittis or Croup etc.")
8
Assess the Airway Dysmorphic features: small mandible, micrognathia, assymetry, large tongue, prominent teeth, syndromes Limited mouth opening, neck movement, burns scars Stridor or surface haemangiomas indicating possible tracheal pathology

9
Anticipated Failure Planning: Staff (anaesthesia, surgical, experienced help) Equipment (laryngoscopes, adjuncts, fibreoptics) Drugs (for sedation, paralysis, anaesthesia) Oxygenation technique: Bag and Mask Two operator technique Supra-glottic airways (guedel, nasal, copa, iGel) LMA Follow an Algorithm
 Equipment (laryngoscopes, adjuncts, fibreoptics) Drugs (for sedation, paralysis, anaesthesia) Oxygenation technique: Bag and Mask Two operator technique Supra-glottic airways (guedel, nasal, copa, iGel) LMA Follow an Algorithm")
11
Un-anticipated Failed Intubation in a Child EXTREMELY RARE in experienced hands Morbidity and Mortality are due to failed oxygenation Management of failed intubation must include: 1. Oxygenation Plan 2. Intubation Plan 3. Rescue Plan Weiss M and Engelhardt T. Proposal for Difficult Airway. Ped Anesth 2010:20;454-464

12
Oxygenation Face mask bag ventilation/oxygenation is an ESSENTIAL skill required before intubation If difficulties occur with oxygenation with a bag and mask consider : Anatomical causes (e.g. tonsils/adenoids) and use jaw thrust, mouth opening, two operator, guedel airway Functional causes (e.g. laryngospasm, bronchospasm) and consider sedatives, relaxants, anaesthesia
 and use jaw thrust, mouth opening, two operator, guedel airway Functional causes (e.g. laryngospasm, bronchospasm) and consider sedatives, relaxants, anaesthesia.")
13
Pediatric Anesthesia November 2012 EDITORIAL Cannot ventilate – paralyze! Markus Weiss and Thomas Engelhardt Pediatric Anesthesia 2012 : 22 : 1147-49

14
Oxygenation Face mask bag ventilation/oxygenation is an ESSENTIAL skill required before intubation If difficulties occur with oxygenation with a bag and mask consider : Anatomical causes (e.g. tonsils/adenoids) and use jaw thrust, mouth opening, two operator, guedel airway Functional causes (e.g. laryngospasm, bronchospasm) and consider sedatives, relaxants, anaesthesia
 and use jaw thrust, mouth opening, two operator, guedel airway Functional causes (e.g. laryngospasm, bronchospasm) and consider sedatives, relaxants, anaesthesia.")
15
Failed Oxygenation Plan A Call for help if these manoeuvres fail Perform Laryngoscopy and remove foreign body or suction secretions Intubate with a suitable sized ETT

16
Failed Oxygenation Plan B Insert an LMA if unable to visualise the vocal cords OR unable to insert the ETT. If this is successful consider (degree of urgency): Waking the child if sedated OR Fibreoptic Intubation through the LMA OR Leaving the LMA until further help arrives
: Waking the child if sedated OR Fibreoptic Intubation through the LMA OR Leaving the LMA until further help arrives.")
17
Tracheal Intubation Teaching and Training are essential for success Optimize conditions Range of Blades and ETT’s Age appropriate position of head and neck Consider sedation and anaesthesia External compression to bring larynx into view Confirm placement (clinically, capnography)
")
18
Failed Intubation Plan A Call for help early Most experienced operator to consider need for: Change of position Different equipment (blades, adjuncts, introducer, Bougies) Different approach (retromolar, paraglossal) Consider new devices (if experienced and practiced!) Video-laryngoscope (Glidescope, Airtrak, C-Mac, Pentax) Fibreoptic devices (Ambu, Bronchoscopes) Limit attempts to 3 to minimize trauma Oxygenation between attempts
 Different approach (retromolar, paraglossal) Consider new devices (if experienced and practiced!) Video-laryngoscope (Glidescope, Airtrak, C-Mac, Pentax) Fibreoptic devices (Ambu, Bronchoscopes) Limit attempts to 3 to minimize trauma Oxygenation between attempts")
19
Failed Intubation Plan B LMA device for oxygenation Mount an ETT on fibreoptic bronchoscope to pass through LMA or Intubating LMA (iLMA) Bougie or Oxygen Exchange Catheter can also be passed through LMA for ETT exchange. If unsuccessful after 2 attempts – STOP Use LMA for oxygenation

20
Rescue Can’t Intubate and Can’t Oxygenate (CICO) Worst situation imaginable The child is going to DIE if nothing is done Need to overcome the psychological barriers to proceeding from this point i.e. anything is worth trying

21
CICO rescue procedure No good evidence in paediatric literature for preferred technique at this point: 3 choices : 1. Rigid Bronchoscope by experienced operator 2. Needle Cricothyroidotomy (Cook, VBM, Ravussin 13g, 14g, 16g) High complication rate 60 % success in experienced hands ! 3. Surgical Cricothyroidotomy / Tracheostomy Traditionally discouraged < 12 yrs Higher success rate in adult literature Recently proposed as preference if < 6 yrs * * Engelhardt T, Weiss M. Curr Opinion Anesth 2012;25:326-332
 High complication rate 60 % success in experienced hands . 3. Surgical Cricothyroidotomy / Tracheostomy Traditionally discouraged < 12 yrs Higher success rate in adult literature Recently proposed as preference if < 6 yrs * * Engelhardt T, Weiss M. Curr Opinion Anesth 2012;25:")
22
Oxygenation techniques with cricothyroidotomy Enk oxygen flow modulator (4 holes) Oxygen tubing with hole 3.0 ETT connector and circuit (low flow) Jet ventilation (set up time?) Allow time (>4 seconds) for lung deflation to prevent baro-trauma
 Oxygen tubing with hole 3.0 ETT connector and circuit (low flow) Jet ventilation (set up time ) Allow time (>4 seconds) for lung deflation to prevent baro-trauma")
23
Needle or Surgical Airway Require practice on simulators, manikins, cadavers or animals Size appropriate equipment MUST be used Cricothyroid puncture in infant or neonate is EXTREMELY DIFFICULT ( membrane is 2x3 mm ) and Trans-tracheal puncture with neck extension may be safer Cote CJ and Hartnick CJ. Ped Anesth 2009:19;66-76 Holm Knudsen et al. Ped Anesth 2012:22;1159-65

25
PREVENTION (skill, assessment, preparation) Oxygenation Face Mask Plan A: Larngoscopy Plan B: LMA Tracheal Intubation BURP, Position, Blades Plan A: Get help + Oxygenate Plan B: LMA Intubation + Oxygenate Rescue Rigid Bronch OR Needle Cricothyroidotomy OR Surgical Airway Failed OxygenationFailed intubation +
 Oxygenation Face Mask Plan A: Larngoscopy Plan B: LMA Tracheal Intubation BURP, Position, Blades Plan A: Get help + Oxygenate Plan B: LMA Intubation + Oxygenate Rescue Rigid Bronch OR Needle Cricothyroidotomy OR Surgical Airway Failed OxygenationFailed intubation +")
27
Summary Practice techniques and failure plans Optimize position, equipment, assistance Call for help EARLY Oxygenate at all times

Similar presentations




>")
 What does the ideal DAT look like? Top work surface and 4-5 drawers Mobile Robust Stocked in a logical sequence Clearly.>")










 Facemasks: Intersurgical sizes 0 and 1 Laerdal sizes 0 and 1 (re-usable) Oropharyngeal Airway (sizes 000, 00 and 0) ETT.>")




