Download presentation
Presentation is loading. Please wait.

1
Patent Pools Increasing access to Medicines and Innovation Ellen ‘t Hoen MSF Access to Essential Medicines Campaign Barcelona 9 Dec. 2008
3
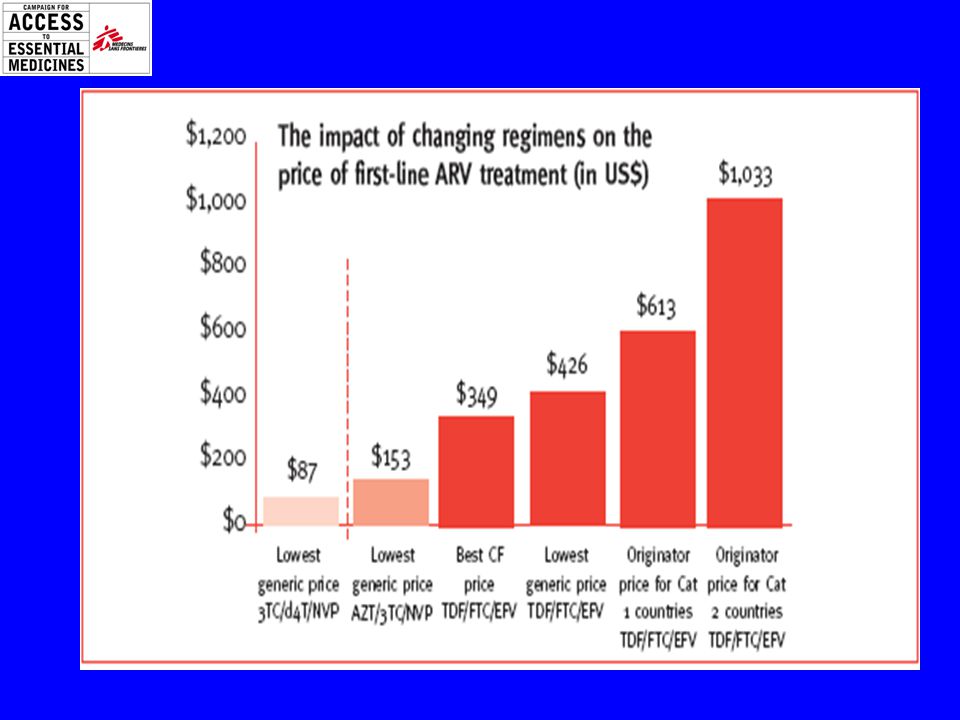
Effect of Generic Competition

4
Fixed Dose Combinations

5
Access to Generics Until 2005 India ’s excluded pharmaceutical products from patenting (1970 Patents Act) Overall, 60% of ARVs taken by 3 million people on treatment are from India 1st line ARV only, 75-80% are from India 80% of ARVs MSF uses are purchased in India “Generics fuel Aids Programme”: Generics accounted for 57% of $131 million U.S. PEPFAR spending in 2007 (WSJ, 31 July 08)
.")
6
But …Times Are Changing 2005 WTO TRIPS Agreement fully implemented Medicines become patentable everywhere India started granting product patents following amendment of the Patents Act in 2005 China started product patents in 1993 Affect on the price of new medicines are becoming apparent

9
Access to treatment for CMV retinitis CMV retinitis is an infection of the eye that most commonly occurs in people at an advanced stage of AIDS who have severely weakened immune systems (CD4 white blood cell count of less than 50). Early detection is crucial because vision loss is irreversible once it has begun.

10
Valganciclovir Valganciclovir price: US$ 10,000 per treatment Patented in India MSF asked a better price to Roche

11
Results of 2 years of talks with Roche Sets the price: 500 CHF per pack (60 tabs of 450 mg ) US$ 1,900 per treatment Determines where it can be used: initially for Sub-Saharan African Countries, least-developed countries, after complaints middle income countries Determines the indication: for use in AIDS patients only Determines who can use it: by NGOs only Where to buy it: purchasing directly from Basel, Switzerland (special labeling) min. USD10,000 order How: Through import only (not from local suppliers) not available where we need it e.g. China
 not available where we need it e.g. China.")
12
Responses 1 Differential pricing –Discounts not steep enough and not as effective as generic competition –No solution to patent barriers to the development of FDCs and new formulations e.G. For children ‘Voluntary’ licenses –Restrictions that hamper full effect of generic competitions e.G on trade in API, export markets –Rare and response to threats e.G CL or legal action, e.G. TAC’s complaint at the south African competition commission and pre grant oppositions

13
Responses 2 Compulsory licensing Thailand => EFV price 1400 Baht (45$) to 615 Baht (19$) a bottle. Brazil ==> EFV 77% price drop ==> increase of patients from 23.300 to 75.000 DC’s use “government use” powers to procure generics regardless of patent status LDC’s exclude product patents when patented India – strict patentability criteria –15 Patent-grant oppositions related to AIDS medicines by Indian civil society

14
Prioritising Health over Patent Protection Harsh criticism on countries with AIDS programmes aiming at universal access that use CL to increase access Retaliation e.g. Abbott refusal to make new drugs available in Thailand (withdrawal of new drug applications incl heat-stable lopi/r) Legal action Novartis against section 3d of the Indian Patents Act Limiting the scope and effectiveness of TRIPS flexibilities through TRIPS+ measures in bilateral trade agreements
 Legal action Novartis against section 3d of the Indian Patents Act Limiting the scope and effectiveness of TRIPS flexibilities through TRIPS+ measures in bilateral trade agreements.")
15
Hand to Hand Combat Price increase of newer medicines lead to rapid increase in cost of treatment We can no longer count on automatic generic competition to bring prices down Threat to scale up, improve care and universal access Patent disputes break out – including over treatments for non-infectious diseases Need for a more systematic approach to deal with monopolies

16
Doha Declaration “ We affirm that the (TRIPS) Agreement can and should be interpreted and implemented in a manner supportive of WTO Members' right to protect public health and, in particular, to promote access to medicines for all. ” WTO Ministerial Declaration on the TRIPS Agreement and Public Health November 14, 2001

17
“For diseases affecting millions of poor people in developing countries, patents are not a relevant factor or effective in stimulating R&D and bringing new products to the market” WHO commission on intellectual property, innovation and public health, April 2006 WHO Commission on IP, Innovation and Public Health (CIPIH)
")
18
World Health Assembly - to encourage the development of proposals for health- needs driven research and development for discussion at the Intergovernmental Working Group that includes a range of incentive mechanisms including also addressing the linkage between the cost of research and development and the price of medicines, vaccines, diagnostic kits and other health-care products and a method for tailoring the optimal mix of incentives to a particular condition or product, with the objective of addressing diseases that disproportionately affect developing countries; (WHA 60.30)
")
19
UNITAID Board decided in principle to establish a patent pool and set in motion a process to do so. (EB8 2 -3 July 08) “Patent pools of upstream technologies may be useful in some circumstances to promote innovation relevant to developing countries. WHO and WIPO should consider playing a bigger role in promoting such arrangements, particularly to address diseases that disproportionately affect developing countries. (WHO Commission on Intellectual Property, Innovation and Public Health, April 2006) “Examine the feasibility of voluntary patent pools of upstream and downstream technologies to promote innovation of and access to health products and medical devices” (WHO Global Strategy and Plan of Action on public health, innovation and intellectual property. May 08) Times are changing … again?
 Patent pools of upstream technologies may be useful in some circumstances to promote innovation relevant to developing countries. WHO and WIPO should consider playing a bigger role in promoting such arrangements, particularly to address diseases that disproportionately affect developing countries. (WHO Commission on Intellectual Property, Innovation and Public Health, April 2006) Examine the feasibility of voluntary patent pools of upstream and downstream technologies to promote innovation of and access to health products and medical devices (WHO Global Strategy and Plan of Action on public health, innovation and intellectual property. May 08) Times are changing … again .")
20
What is a patent pool? A number of patent rights held by different owners (companies, universities, government institutions) are brought together (pooled) and made available on a non-exclusive basis to manufacturers and distributors of medicines against the payment of royalties. Third parties e.g. generic manufactures of drugs can make use of the patents against the payment of a royalty “One stop shop” - no need for case by case negotiations
 are brought together (pooled) and made available on a non-exclusive basis to manufacturers and distributors of medicines against the payment of royalties. Third parties e.g. generic manufactures of drugs can make use of the patents against the payment of a royalty One stop shop - no need for case by case negotiations.")
21
Patent Pool and WHO recommended improved 1 st line ARV New WHO recommended 1 st line regimen: –TDF/ 3TC or FTC/ EFV or NVP –4 to 11 fold increase in price compared to d4t containing regimen Potentially 5 patent holders: –TDF and FTC– Gilead –3TC – GSK –EFV – Merck –NVP – BI –TDF/FTC/EFV – Gilead/BMS joint patent application

22
Is the Patent Pool Feasible? Political momentum –WHO IP/PH negotiations paved the way –UNITAID commitment –NGO commitment Companies’ initial responses positive: –IFPMA “very interesting” –European Generics Association: “interesting” –Indian Generics Association endorsed UNITAID’s board decision –Individual companies response positive Hard work ahead to succeed –Devil will be in the details of the licenses –If any of you can help let us know!

23
Conclusion Changed environment post TRIPS era Newer products patented in developing countries –Prices will not come down automatically –IP barriers to the development of specific formulations e.g. FDC Deliberate action needed to counter the consequences of global pharmaceutical patenting –Use of the flexibilities in patent law by governments e.g. compulsory licensing –New licensing mechanisms: UNITAID Patent Pool –Alternative mechanisms for R&D financing

24
Thank You! http://www.accessmed-msf.org/ Ellen.t.hoen@paris.msf.org

Similar presentations





 From Alma Ata, via Doha to Geneva (in 10 minutes) Bellagio, Italy 22-26 October 2007 Ellen ‘t.>")















