Download presentation
Presentation is loading. Please wait.

1
Dose Adjustments and Fighting the Emergence of Resistance in Pneumococci Donald E. Low, MD Canada

2
Optimize antimicrobial use 1.Prevent resistance from emerging 2.Prevent colonization/infection with pre- existing resistant strains 1.Prevent resistance from emerging 2.Prevent colonization/infection with pre- existing resistant strains

3
AntimicrobialsAntimicrobials l β-Lactams l Fluoroquinolones l β-Lactams l Fluoroquinolones

4
Emergence of resistance in pneumococci l ß-lactam –Acquisition of DNA which encodes resistance element l Fluoroquinolones –Spontaneous point mutations l ß-lactam –Acquisition of DNA which encodes resistance element l Fluoroquinolones –Spontaneous point mutations

5
β-Lactams

7
Mechanism of action

8
Mechanism of action: -Lactams bind to PBP Peptidoglycan Layer Cytoplasmic Membrane Penicillin-Binding Proteins Cross-link Cell wall Slide of M. Jacobs

9
Mechanisms of resistance: alterations in target binding site Peptidoglycan Layer Cytoplasmic Membrane Penicillin-Binding Proteins Cross-link Cell wall Slide of M. Jacobs

10
Mechanism of resistance l PBPs with reduced binding affinities which are the products of mosaic genes that have arisen via inter-species transformation and recombination events l resistance develops in a step-wise manner with the level of resistance in a particular strain reflecting the number of PBPs affected by the mosaicism l PBPs with reduced binding affinities which are the products of mosaic genes that have arisen via inter-species transformation and recombination events l resistance develops in a step-wise manner with the level of resistance in a particular strain reflecting the number of PBPs affected by the mosaicism

11
-Lactam Resistance due to Alterations in the Penicillin Binding Protein (PBP) Target Binding Sites Gene pbp1a pbp1b pbp2a pbp2b pbp2x Penicillin Susceptible Penicillin Resistant Penicillin Intermediate Slide of M. Jacobs

12
Antimicrobial susceptibilities and analysis of genes related to penicillin or macrolide resistance in S. pneumoniae Hiramatsu K et a. Intern J Antimicrob Agents 2004 PBP changes

13
Resistance due to selection acquisition of piece of DNA via inter- species transformation and recombination Sanders CC et al. J Infect Dis 1986;154:792-800 Treatment with marginally active drug Resistant bugs are selected for by drug treatment as susceptible strains die off Resistant clone multiplies Resistance spreads

14
Maximizing T>MIC l Increased dosing frequency l Higher dose l Improved pharmacodynamic profile within class l Increased duration of infusion l Increased dosing frequency l Higher dose l Improved pharmacodynamic profile within class l Increased duration of infusion

15
Dagan & Leibovitz. Lancet Infect Dis 2002; 2:593–604

16
What’s the evidence this actually happens?

17
Adapted from Guillemot & Carbon JAMA 1998; 279: 365–370 25 50 75 100 Oral cephalosporinAmoxicillin Penicillin susceptibility (MIC) in µg/ml ‘High dose’ Median ‘Low dose’ Percentile of daily dose 0 0.016 0.032 0.064 0.125 0.25 0.50 1 2 Sub-optimal dosage leads to increased resistance
 in µg/ml ‘High dose’ Median ‘Low dose’ Percentile of daily dose Sub-optimal dosage leads to increased resistance")
18
Effect of Short-Course, High-Dose Amoxicillin Therapy on Resistant Pneumococcal Carriage Children were randomly assigned to receive 1 of 2 twice-daily regimens of amoxicillin: 90 mg/kg per day for 5 days (n = 398) or 40 mg/kg per day for 10 days (n = 397) At the day 28 visit, risk of penicillin-nonsusceptible pneumococcal carriage was significantly lower in the short- course, high-dose group (24%) compared with the standard- course group (32%); relative risk (RR), 0.77; 95% confidence interval (CI), 0.60-0.97; P =.03; risk of trimethoprim- sulfamethoxazole nonsusceptibility was also lower in the short- course, high-dose group (RR, 0.77; 95% CI, 0.58-1.03; P =.08). Schrag et al. JAMA 2001; 286:49–56

20
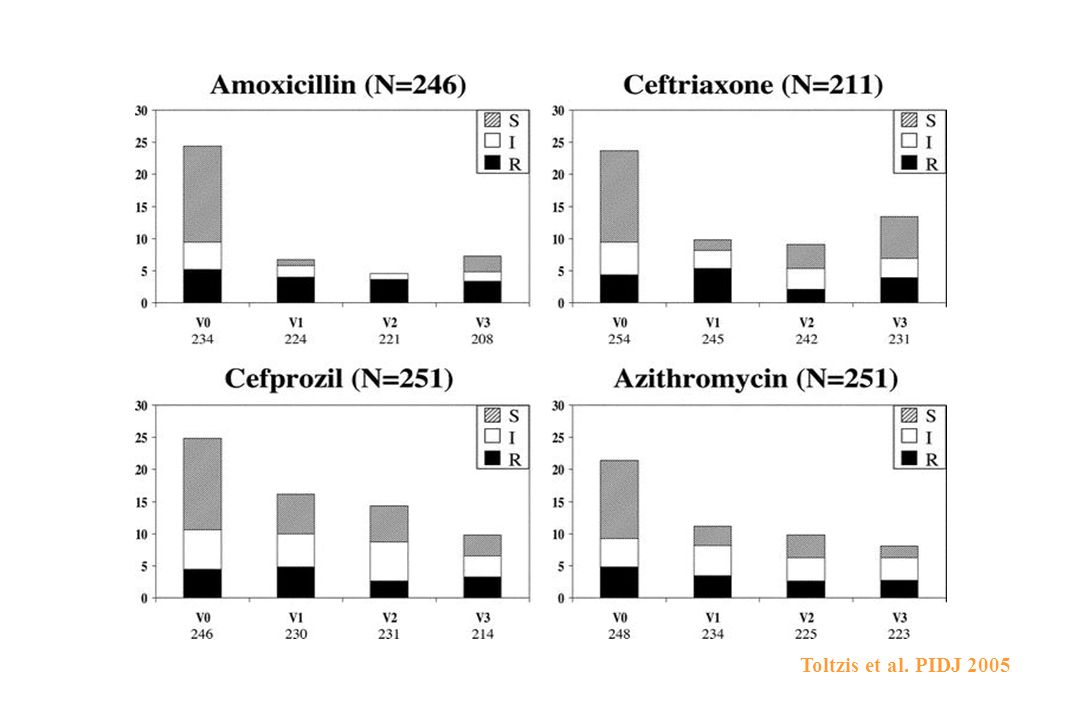
Impact of Amoxicillin on Pneumococcal Colonization Compared With Other Therapies for Acute Otitis Media Children presenting with acute otitis media were randomized to receive amoxicillin, cefprozil, ceftriaxone or azithromycin. Nasopharyngeal specimens were collected on days 0, 3–5, 10–14 and 28–30 and assessed for the presence of S. pneumoniae Toltzis et al. PIDJ 2005

21
Impact of Amoxicillin on Pneumococcal Colonization Compared With Other Therapies for Acute Otitis Media Colonization by nonsusceptible pneumococci was unaltered during the observation period in all treatment groups, with no detectable differences among groups at each visit By contrast, there was a substantial reduction in the prevalence of colonization by penicillin-susceptible organisms, most notably in subjects treated with amoxicillin This resulted in a proportional shift toward resistant organism colonization in all groups, with this shift being significantly more pronounced among amoxicillin recipients than in the other groups at 10– 12 days (P < 0.02 for each comparison with amoxicillin) Toltzis et al. PIDJ 2005

23
Bacteriological eradication maximizes clinical success: evidence in AOM Bacteriological success 97% clinical success faster resolution of signs and symptoms Bacteriological failure 63% clinical success slower resolution of signs and symptoms Dagan et al. Pediatr Infect Dis J 1998; 17: 776–782

24
Failure of bacteriological eradication results in clinical failure in AECB Pechère. Infect Med 1998; 15(Suppl. E): 46–54 Eradication failure rate (%) Clinical failure rate (%) Meta-analysis: 12 studies, 16 antibiotics Slope = 0.59, correlation = 0.83 0 10 20 30 40 50 60 7080 60 50 40 30 20 0 10
: 46–54 Eradication failure rate (%) Clinical failure rate (%) Meta-analysis: 12 studies, 16 antibiotics Slope = 0.59, correlation =")
25
Infection Inappropriate treatment Failed bacterial eradication Spread Selection of resistant bacteria Increasing resistance Appropriate treatment Maximize clinical cure Bacterial eradication Minimize potential for resistance Breaking the ‘vicious cycle’

26
Fluoroquinolones

27
Topoisomerases: Critical Enzymes in DNA Replication l Topoisomerase IV (parC, parE) l DNA gyrase (gyrA, gyrB) l Topoisomerase IV (parC, parE) l DNA gyrase (gyrA, gyrB)
 l DNA gyrase (gyrA, gyrB) l Topoisomerase IV (parC, parE) l DNA gyrase (gyrA, gyrB)")
28
Development of Resistance l De novo –Spontaneous mutations in primary target –The frequency of a spontaneous mutation is 1/10 7 to 10 8 l De novo –Spontaneous mutations in primary target –The frequency of a spontaneous mutation is 1/10 7 to 10 8

29
l stepwise occurrence l “First-step” –enzyme for which the quinolone has the greatest affinity –MIC increases l “Second-step” –result in a further increase in MIC l stepwise occurrence l “First-step” –enzyme for which the quinolone has the greatest affinity –MIC increases l “Second-step” –result in a further increase in MIC Spontaneous Mutation

30
Fluoroquinolone Use and Pneumococcal Resistance: Canada, 1988–1998 Year 0 1 2 3 4 5 19881989199019911992199319941995199619971998 % cipro-R pneumococci 0 1 2 3 4 5 6 Prescriptions per 100 Persons <15 years 15-64 years 65 years Quinolone use Chen et al. 1999 NEJM

31
From 1994 to 1998, there was a statistically significant increase in the proportion of isolates with a MIC for ciprofloxacin of 32 g/ml (P=0.04) Chen et al. 1999 NEJM

32
Relationship between increased levofloxacin use and decreased susceptibility of S. pneumoniae in the US l All data for S. pneumoniae blood isolates collected from US hospitals participating in the SENTRY Antimicrobial Surveillance Program (1997–2002) were included l Annual regional quinolone use data for the same period were obtained from IMS and matched using designated “Metropolitan Statistical Areas” to the geographical region surrounding each SENTRY Program hospital l The primary outcome variable was the in vitro activity of levofloxacin against S. pneumoniae l All data for S. pneumoniae blood isolates collected from US hospitals participating in the SENTRY Antimicrobial Surveillance Program (1997–2002) were included l Annual regional quinolone use data for the same period were obtained from IMS and matched using designated “Metropolitan Statistical Areas” to the geographical region surrounding each SENTRY Program hospital l The primary outcome variable was the in vitro activity of levofloxacin against S. pneumoniae Bhavnani et al Diagn Microbiol Infect Dis 2005
 were included l Annual regional quinolone use data for the same period were obtained from IMS and matched using designated Metropolitan Statistical Areas to the geographical region surrounding each SENTRY Program hospital l The primary outcome variable was the in vitro activity of levofloxacin against S. pneumoniae l All data for S. pneumoniae blood isolates collected from US hospitals participating in the SENTRY Antimicrobial Surveillance Program (1997–2002) were included l Annual regional quinolone use data for the same period were obtained from IMS and matched using designated Metropolitan Statistical Areas to the geographical region surrounding each SENTRY Program hospital l The primary outcome variable was the in vitro activity of levofloxacin against S. pneumoniae Bhavnani et al Diagn Microbiol Infect Dis")
34
PD therapeutic goals for fluoroquinolones: Peak:MIC or AUC:MIC ratio 35–40 Time AUC:MIC ratio, or Peak:MIC ratio Peak Area under curve (AUC) Antibiotic concentration ( g/ml) Wright et al. J Antimicrob Chemother 2000; 46 :669–683

36
Fluoroquinolone pharmacodynamics for S. pneumoniae : relationship between AUC and bacterial eradication l In vitro model –Lacy et al. Antimicrob Agents Chemother 1999;43:672–677 –Lister & Sanders. J Antimicrob Chemother 1999;43:79–86 l In vivo model –Andes & Craig. 39th ICAAC 1999 [Abstr. P-0191] –Mattoes et al. Antimicrob Agents Chemother 2001:45;2092–2097 l In vivo human –Ambrose et al. Antimicrob Agents Chemother 2001;45:2793–2797 –Free-drug 24-hour AUC:MIC >33.7 resulted in 100% microbiological eradication; probability of response was 64% at AUC:MIC <33.7 l In vitro model –Lacy et al. Antimicrob Agents Chemother 1999;43:672–677 –Lister & Sanders. J Antimicrob Chemother 1999;43:79–86 l In vivo model –Andes & Craig. 39th ICAAC 1999 [Abstr. P-0191] –Mattoes et al. Antimicrob Agents Chemother 2001:45;2092–2097 l In vivo human –Ambrose et al. Antimicrob Agents Chemother 2001;45:2793–2797 –Free-drug 24-hour AUC:MIC >33.7 resulted in 100% microbiological eradication; probability of response was 64% at AUC:MIC <33.7 AUC/MIC of 40 optimizes antibacterial killing against S. pneumoniae

37
Free AUC/ MIC Ciprofloxacin 750 mg q12 Levofloxacin 500 mg q24 Gatifloxacin 400 mg q24 Moxifloxacin 400 mg q24 (94-188) (52-170) (16-103) (11-22) 0 50 100 150 200 250 300 Grant E.,Nicolau DP.Antibiotic for Clinicians 1999;3(Suppl 1):21-28. Comparison of Quinolone In Vivo Potency for Streptococcus pneumoniae

38
Emergence of First Step ParC Mutation in Streptococcus pneumoniae l TRUST surveillance program, 1999-2000 found that 6.6% and 71% of the S. pneumoniae isolates having an MIC of 1.0 g/ml and 2.0 g/ml, respectively, contain a first step parC mutation. Davies TA, et al. AAC 2002;46:119-124 l 164 unique patient isolates of S. pneumoniae, 29.9% of the isolates harbored a mutation in either the parC or the gyrA gene, with the majority of isolates (67.3%) having a mutation in the parC locus only. Brueggemann AB, et al. AAC 2002;46(3):680-688 l TRUST surveillance program, 1999-2000 found that 6.6% and 71% of the S. pneumoniae isolates having an MIC of 1.0 g/ml and 2.0 g/ml, respectively, contain a first step parC mutation. Davies TA, et al. AAC 2002;46:119-124 l 164 unique patient isolates of S. pneumoniae, 29.9% of the isolates harbored a mutation in either the parC or the gyrA gene, with the majority of isolates (67.3%) having a mutation in the parC locus only. Brueggemann AB, et al. AAC 2002;46(3):680-688
 having a mutation in the parC locus only. Brueggemann AB, et al. AAC 2002;46(3): l TRUST surveillance program, found that 6.6% and 71% of the S. pneumoniae isolates having an MIC of 1.0 g/ml and 2.0 g/ml, respectively, contain a first step parC mutation. Davies TA, et al. AAC 2002;46: l 164 unique patient isolates of S. pneumoniae, 29.9% of the isolates harbored a mutation in either the parC or the gyrA gene, with the majority of isolates (67.3%) having a mutation in the parC locus only. Brueggemann AB, et al. AAC 2002;46(3):")
39
Emergence of First Step ParC Mutation in Streptococcus pneumoniae l examined 115 S. pneumoniae isolates with a levofloxacin MIC of >2 mg/mL for first-step parC mutations. A total of 48 (59%) of 82 isolates with a levofloxacin MIC of 2 mg/mL, a level considered susceptible by NCCLS criteria, had a first-step mutation in parC. Lim et al. EID 2003
 of 82 isolates with a levofloxacin MIC of 2 mg/mL, a level considered susceptible by NCCLS criteria, had a first-step mutation in parC. Lim et al. EID")
40
Targets for the Fluoroquinolones l First-step –Topoisomerase IV (parC, parE) –DNA gyrase (gyrA, gyrB) l First-step –Topoisomerase IV (parC, parE) –DNA gyrase (gyrA, gyrB) or
 –DNA gyrase (gyrA, gyrB) l First-step –Topoisomerase IV (parC, parE) –DNA gyrase (gyrA, gyrB) or")
41
40 Wild type 1 st step 1 st and 2 nd

42
41

43
42

44
43

45
44

46
45

47
46 Pneumococcal pneumonia with first-step mutant

48
47 Wild type 1 st step 1 st and 2 nd

49
48

50
49

51
Fluoroquinolone treatment failures l 19 treatment failures that met our case definition: –LRTI due to a fluoroquinolone resistant pneumococci that –failed clinically or bacteriologically after ≥ 48 hours of fluoroquinolone therapy, such that additional antimicrobial therapy was required l 19 treatment failures that met our case definition: –LRTI due to a fluoroquinolone resistant pneumococci that –failed clinically or bacteriologically after ≥ 48 hours of fluoroquinolone therapy, such that additional antimicrobial therapy was required (Fuller and Low, CID, In Press)
")
52
Fluoroquinolone treatment failures l 7 had a history of prior fluoroquinolone use QRDR characterization available for 15 isolates –12 had mutations in both parC and qyrA – 3 had mutation in parC only l 7 had a history of prior fluoroquinolone use QRDR characterization available for 15 isolates –12 had mutations in both parC and qyrA – 3 had mutation in parC only (Fuller and Low, CID, In Press)
")
53
Levofloxacin Resistance in S. pneumoniae : Results from a Cross-Canada Surveillance Study Canadian Bacterial Surveillance Network, Feb. 2005

54
Prescriptions for Fluroquinolones used for RTIs Source: IMS Canada

55
Relative risk of infection with FQ resistant pneumococci, by prior antibiotic use

56
Risk factors for levofloxacin resistance: Multivariable analysis 9.9 (2.2, 45)Nosocomial 12.9 (3.9, 43)Nursing home acquired 12.1 (4.1, 35)Prior FQ use Odds Ratio (95% CL)Characteristic
Nosocomial 12.9 (3.9, 43)Nursing home acquired 12.1 (4.1, 35)Prior FQ use Odds Ratio (95% CL)Characteristic")
57
ConclusionsConclusions l That the best way to fight the emergence of antimicrobial resistance is to minimize the use of these agents l When needed, the strategy of best dosage may depend on the class of agents or agent within the class l That the best way to fight the emergence of antimicrobial resistance is to minimize the use of these agents l When needed, the strategy of best dosage may depend on the class of agents or agent within the class

Similar presentations




 surveillance (2009Q1-4) **** Data as.>")


 William A. Craig, MD University of Wisconsin.>")















