Download presentation
Presentation is loading. Please wait.

1
Medicaid and SCHIP in 2007: Current Trends and the Outlook for the Future Vernon K. Smith, Ph.D. for State Coverage Initiatives Workshop for State Officials Conducted by AcademyHealth Denver August 3, 2007 vsmith@healthmanagement.com

2
Smith1 Outline for Presentation Medicaid spending trends Medicaid & SCHIP enrollment trends State policy directions –Cost containment –DRA Initiatives –Waiver Initiatives Outlook for the future –Policy focus and spending projections

3
Smith2 “Medicaid… …has always been under-appreciated, particularly for the role that it plays in the lives of so many Americans.” –John Iglehart, Editor, Health Affairs

4
Smith3 Medicaid Nationally in 2007: A State – Federal Partnership $340 billion for over 62 million individuals, the largest health program in America … 30 million children –including 1.5 million newborns 16 million adults in families 10 million persons with disabilities 6 million persons age 65 or older Medicaid accounts for 44% of federal funds to states, the largest single component Sources: CBO March 2007 Medicaid Baseline; HMA projections of 2007 total spending. All data for federal fiscal year 2007. NASBO, State Expenditure Report, 2006.

5
Smith4 Medicaid is the “Financial Glue” of the U.S. Health Care Safety Net –Mental health over half of publicly financed care –Public health and schools –Hospitals that serve the uninsured special Medicaid “DSH” payments $16 billion in 2007 –Community Health Centers Medicaid averages 40% of CHC revenues –Medicare 7 million low-income elderly and disabled are “dual eligibles”– on both Medicaid and Medicare “Duals” account for about 40% of Medicaid spending

6
Smith5 Note: Data for 2005. SOURCE: Aaron Catlin, et.al., “National Health Spending in 2005,” Health Affairs, January/February 2007. Based on National Health Care Expenditure Data for 2005, CMS, Office of the Actuary, 2007. Part D allocation by Health Management Associates. Medicaid: 1/6 of U.S. Health Spending and 2.7% of GDP After Part D 2006 19% Before Part D 2005

7
Smith6 Medicaid Spending Increased When State Tax Revenue Dropped: Annual Percentage Changes 1997-2006 NOTE: State Tax Revenue data is adjusted for inflation and legislative changes. Preliminary estimate for 2006. SOURCE: Vernon Smith, Kathleen Gifford, Eileen Ellis, Amy Wiles, Robin Rudowitz, Molly O’Malley and Caryn Marks, Low Medicaid Spending Growth Amid Rebounding State Revenues: Results from a 50-State Medicaid Budget Survey State Fiscal Years 2006 and 2007, Kaiser Commission on Medicaid and the Uninsured, October 2006..kff.org/Medicaid/7569.cfm

8
Smith7 U.S. Medicaid Spending: Growth Now at Near-Record Lows Due to: Number of persons enrolled –Low growth Health care costs –Slowing in growth overall, particularly for prescription drugs Cost containment –Cumulative effect of strategies adopted in recent years

9
Smith8 Growth in Medicaid and SCHIP Coverage of Children, 1997-2005 Millions of Children

10
Smith9 U.S. Medicaid Enrollment: Percentage Changes FY 1992- FY 2006 SOURCES: Eileen R. Ellis, Vernon K. Smith and David M. Rousseau, Medicaid Enrollment in 50 States, June 2005 Update – Preliminary Data, Kaiser Commission on Medicaid and the Uninsured, June 2006. 2006 data provided by state officials to Health Management Associates for Kaiser Commission on Medicaid and the Uninsured, 2006. For 1992-1997 data are from CMS for federal fiscal years. 1998-2006 are June-June state fiscal years. Annual growth rate:

11
Smith10 Increases in Health Insurance Premiums, Earnings and Inflation, 1988-2006 * Estimate is statistically different from the previous year shown at p<0.05.† Estimate is statistically different from the previous year shown at p<0.1. Note: Data on premium increases reflect the cost of health insurance premiums for a family of four. Source: KFF/HRET Survey of Employer- Sponsored Health Benefits: 1999-2006; KPMG Survey of Employer-Sponsored Health Benefits:1993, 1996; The Health Insurance Association of America (HIAA): 1988, 1989, 1990; Bureau of Labor Statistics, Consumer Price Index (U.S. City Average of Annual Inflation (April to April), 1988-2005; Bureau of Labor Statistics, Seasonally Adjusted Data from the Current Employment Statistics Survey (April to April), 1988-2006. 13.9%† 3.5% 3.8%
: 1988, 1989, 1990; Bureau of Labor Statistics, Consumer Price Index (U.S. City Average of Annual Inflation (April to April), ; Bureau of Labor Statistics, Seasonally Adjusted Data from the Current Employment Statistics Survey (April to April), %† 3.5% 3.8%.")
12
Smith11 Fiscal Pressures Forced Every State to Take Aggressive Medicaid Cost Containment FY 2003 – FY 2007 NOTE: Adopted actions are not always implemented. SOURCE: Vernon Smith, Kathleen Gifford, Eileen Ellis, Amy Wiles, Robin Rudowitz, Molly O’Malley and Caryn Marks, Low Medicaid Spending Growth Amid Rebounding State Revenues: Results from a 50-State Medicaid Budget Survey State Fiscal Years 2006 and 2007, Kaiser Commission on Medicaid and the Uninsured, October 2006. www.kff.org/Medicaid/7569.cfm Number of States, by Year

13
Smith12 Improving State Revenues Decreased Likelihood of Medicaid Rate Cuts, 2004 - 2007 SOURCE: Vernon Smith, Kathleen Gifford, Eileen Ellis, Amy Wiles, Robin Rudowitz, Molly O’Malley and Caryn Marks, Low Medicaid Spending Growth Amid Rebounding State Revenues: Results from a 50-State Medicaid Budget Survey State Fiscal Years 2006 and 2007, Kaiser Commission on Medicaid and the Uninsured, October 2006. www.kff.org/Medicaid/7569.cfm FY 2004FY 2005FY 2006FY 2007 Number of States Cutting Medicaid Rates for Inpatient Hospitals, Doctors, Nursing Facilities or Managed Care Organizations

14
Smith13 In 2006 and 2007, States Increasingly Turned to Program and Quality Improvement SOURCE: Vernon Smith, Kathleen Gifford, Eileen Ellis, Amy Wiles, Robin Rudowitz, Molly O’Malley and Caryn Marks, Low Medicaid Spending Growth Amid Rebounding State Revenues: Results from a 50-State Medicaid Budget Survey State Fiscal Years 2006 and 2007, Kaiser Commission on Medicaid and the Uninsured, October 2006. www.kff.org/Medicaid/7569.cfm Number of States in

15
Smith14 Disease Management: Focus on 4 Percent of Medicaid Enrollees with 48% of Expenditures SOURCE: Urban Institute estimates for Kaiser Commission on Medicaid and the Uninsured based on MSIS 2001 data, 2005. Adults 1% Disabled 25% Total = 46.9 millionTotal = $180.0 billion Elderly 20% <$25,000 in Costs 96% Children 3% <$25,000 in Costs 52% >$25,000 in Costs Children (.2%) Adults (.1%) Disabled (1.6%) Elderly (1.8%) >$25,000 in Costs 4% 48%
 Adults (.1%) Disabled (1.6%) Elderly (1.8%) >$25,000 in Costs 4% 48%.")
16
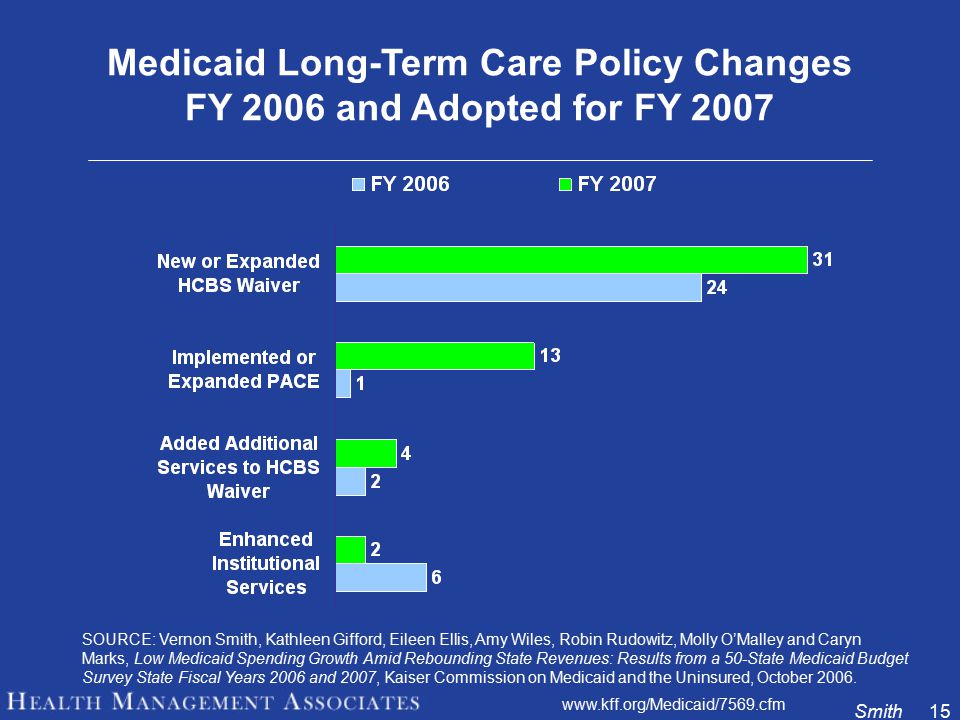
Smith15 Medicaid Long-Term Care Policy Changes FY 2006 and Adopted for FY 2007 SOURCE: Vernon Smith, Kathleen Gifford, Eileen Ellis, Amy Wiles, Robin Rudowitz, Molly O’Malley and Caryn Marks, Low Medicaid Spending Growth Amid Rebounding State Revenues: Results from a 50-State Medicaid Budget Survey State Fiscal Years 2006 and 2007, Kaiser Commission on Medicaid and the Uninsured, October 2006. www.kff.org/Medicaid/7569.cfm
17
Smith16 Medicaid Long Term Care: Trend Is To Home and Community Care 1991 - 2006 86% 79% 71% 21% 14% $34 B $52 B $75 B Billions of Dollars for U.S. Source: 1991-2001, Brian Burwell, Kate Sredl and Steve Eiken, Thomson Medstat, 2006. 2006 projection by Health Management Associates, 2007. $101 B 38% 62% 29% HCBS

18
Smith17 Across States, the Medicaid Now Has Moved Beyond Cost Containment Leaders in 2005: Vermont –Expanded coverage –“Global Commitment” for all federal funds –Preserved federal Medicaid funds Florida –Rewards for personal responsibility –“Defined Contribution” for managed care –Preserved federal Medicaid funds

19
Smith18 In 2006, the DRA Provided New Options New Flexibility Options: –Benefits or Cost Sharing –New HSA-like “Health Opportunity Accounts” New Long Term Care Options –LTC Partnership –Self-Directed Personal Assistance Service –Money Follows the Person programs –HCBS as a State Plan Option –About half of all states considering LTC options SOURCE: Vernon Smith, Kathleen Gifford, Eileen Ellis, Amy Wiles, Robin Rudowitz, Molly O’Malley and Caryn Marks, Low Medicaid Spending Growth Amid Rebounding State Revenues: Results from a 50-State Medicaid Budget Survey State Fiscal Years 2006 and 2007, Kaiser Commission on Medicaid and the Uninsured, October 2006. www.kff.org/Medicaid/7569.cfm

20
Smith19 So far, Few States Have Used DRA Options Benefit Flexibility: WV, KY, FL, KS Cost Sharing Flexibility: KY Health Opportunity Acct:SC HCBS State Plan Option: IA Cash & Counseling Option: AL

21
Smith20 In 2006, Two States Leveraged Medicaid to Move toward Broad, Near-Universal Health Coverage Massachusetts Health Plan –Universal coverage, with individual and employer mandates / assessment of $295 –Subsidies for low income individuals –Health insurance “Connector” –Strong quality component Vermont – Catamount Health Plan –Near-universal coverage, with Premium Assistance for low-income uninsured –New individual product for uninsured –Employer assessment of $365/FTE (exceptions) –Chronic care management initiative
 –Chronic care management initiative")
22
Smith21 In 2007, Over 2/3 of All States Offered New Proposals Governors in 34 states offered plans to reduce the number of uninsured children, parents, adults, aged and disabled in their state through –Medicaid expansions –SCHIP expansions –DRA waivers –Comprehensive Section 1115 waivers –Market-based approaches –Improving quality through prevention and better management of chronic conditions Source: NASBO, The Fiscal Survey of States, June 2007.

23
Smith22 Indiana Plan Adopted 2007 Eligibility for subsidized private insurance: –up to 200 percent of the FPL ($20,420 for an individual, $41,300 for family of four) could buy insurance. –Estimate 132,000 persons qualify. Coverage: –$500 in preventive care; a $1,100 health savings account; up to $300,000 of annual coverage from a private insurer. Premiums: –2 to 5 percent of adjusted gross income, sliding scale. Medicaid eligibility: –increases for children and pregnant women Other provisions: –allows children up to age 24 to stay on their parents' health insurance plans; –creates an insurance pool for small businesses; and –tax incentives to encourage more employers to offer insurance. Financing: cigarette tax increased by $0.44 to $0.995

24
Smith23 Oregon “The biggest agenda piece right now is to insure all kids in Oregon.” –Russ Kelley, spokesman for Oregon House Speaker Jeff Merkley, quoted in The New York Times, June 11, 2007

25
Smith24 Pennsylvania Comprehensive, 47-point health plan: “Prescription for Pennsylvania” Coverage for all children “…affordable health insurance to all adults, with payments based on income.” Focus on personal responsibility and quality No mandates.

26
Smith25 California …The Boldest Proposal Yet Universal coverage for 6.5 million uninsured Expanded Medicaid coverage for all children Mandates for Employers (with 10 or more employees) and individuals Assessments on providers –2% for doctors, 4% for hospitals “California will be the first state, I guarantee you, where we will have universal health coverage, where we will insure everybody.” --Gov. Arnold Schwarzenegger, speaking to the California Medical Association, May 2, 2007

27
Smith26 An Emerging Consensus: To Control Medicaid Spending, Control Overall Health Costs “Medicaid is one purchaser in a larger health care market … the most effective way to control Medicaid spending growth is to pursue strategies to control overall health care spending growth.” --Richard Kronick and David Rousseau, “Is Medicaid Sustainable? Spending Projections for the Program’s Second Forty Years,” Health Affairs – Web Exclusive, February 23, 2007.

28
Smith27 New Focus: Slow the growth of conditions that need treatment A new emphasis on prevention, primary care and care management for –Chronic disease is the number one cause of death and disability in the U.S. –accounts for 70 percent of all deaths and more than 75 percent of health care spending “We should be moving into an era now… that puts much more emphasis on keeping people well and not just paying for costly complications after they happen.” --Mark McClellan, former CMS Administrator, July 17, 2007.

29
Smith28 Data-Based Policy: Obesity, Disease Prevalence and Health Care Spending Are Linked Total diabetes prevalence has increased 53% over the past 20 years “All the increase in diabetes is linked to the doubling of obesity prevalence among adults.” 27% of the increase in health care spending is accounted for by the increase in obesity prevalence. Source: Kenneth Thorpe, 2006

30
Smith29 Historic Growth of Obesity Prevalence Adults, 1978-2002 Source: Kenneth Thorpe, 2006 19782002

31
Smith30 States Are Also Focusing on IT to Improve the Delivery of Health Care Fact: Chronically ill Americans receive the recommended treatment only 56% of the time. Improvements in information technology infrastructure have great potential to improve care, especially for the chronically ill Source: Partnership for Fighting Chronic Disease, 2007

32
Smith31 The Future: Medicaid Cost Increases Expected to Parallel Overall Health Spending “Medicaid spending as a share of national health spending will average 16.6 percent from 2006 to 2025 – roughly unchanged from the 16.5 percent in 2005.” Even after accounting for “… the anticipated decline in employer-sponsored health insurance and the long term care needs of the baby boomers…” --Richard Kronick and David Rousseau, “Is Medicaid Sustainable? Spending Projections for the Program’s Second Forty Years,” Health Affairs – Web Exclusive, February 23, 2007.

33
Smith32 Medicaid Spending Projected to More than Double to Over $700 Billion in Ten Years: 2007 - 2017 Source: Health Management Associates estimates based on data from CBO and CMS, 2007. All funds: Federal, State and Local

34
Smith33 Medicaid Spending Projections Average annual Medicaid spending growth: Ten year forecast –CMS: 8% –CBO: 8% 9% for long term care State budgets: –increase on average by 6.5% Based on actual growth over the past 30 years. Sources: Source: John Poisal, et al., “Health Spending Projections Through 2016: Modest Changes Obscure Part D’s Impact,” Health Affairs, 21 February 2007; CBO, Medicaid Baseline 2007; NASBO, Fiscal Survey of States, June 2007.

35
Smith34 Medicaid Projected to Continue to Grow as a Share of State Budgets: 1985 - 2010 Source: National Association of State Budget Officers, State Expenditure Reports, 2005 and earlier reports; 2010 percentages projected by HMA. Total Medicaid Spending as % of State Budgets GF

36
Smith35 Summary and Conclusion Medicaid is the largest health program in America and one of the most significant programs administered by states. States have a huge stake in the future of Medicaid, particularly due to the limits of state fiscal capacity to sustain it. Medicaid has the potential to –Help finance strategies to reduce the number of uninsured –improve quality of care –improve the health of beneficiaries that could help slow overall health costs and costs to Medicaid

Similar presentations

















 MinnesotaCare General Assistance Medical Care (GAMC) Minnesota Comprehensive.>")

