Download presentation
Presentation is loading. Please wait.

1
Fatigue and Resident Education Thomas Miner, MD, FACS Associate Program Directory, Surgery Residency Director of Surgical Oncology Assistant Professor of Surgery Warren Alpert Medical School at Brown University

3
Fatigue and Resident Education Why should I care? Not my problem….. Tired, fatigued, burnt out, distressed. What’s the difference? The emperor’s new cloths? Sleep: a refresher course

4
Who is at risk for fatigue? Insufficient sleep Fragmented sleep –Pagers, phone calls, emergencies Circadian rhythm disruption –Night float Genetic Factors –Some people need more –Surgical selection?

5
Warning Signs of Fatigue Falling asleep in conferences or on rounds Feeling restless and irritable with staff, colleagues, family, and friends Having to check your work repeatedly Having difficulty focusing on the care of your patients

6
Fatigue and Resident Education 1999 Institute of Medicine report –48,000 to 98,000 deaths due to preventable medical errors –50% of hospitalized patients affected by medical error –Numerous reports implicate fatigue as source of errors Patient Safety –“We deserve competent health care from well rested physicians” - Public Citizen 2003 2003 ACGME instituted duty hour regulations –Number of work hours per week –Number of continuous work hours –Frequency of in-house call –Minimum amount of time between duty periods –Days free of work duties

7
© American Academy of Sleep Medicine American Academy of Sleep Medicine *Baldwin and Daugherty, 1998-9 Survey of 3604 PGY1,2 Residents Work Hours, Medical Errors, and Workplace Conflicts by Average Daily Hours of Sleep*

9
Number of Fatigue-Related Accidents

10
Work Hours and Motor Vehicle Accidents ExtendedNo Extended MVC5873 Rate ( per 1000 commutes )1.070.40 Near Misses19711156 Rate ( per 1000 commutes )36.426.41 Nodding w/driving9.3%6.6% Nodding at STOP16.5%10.2% L Barger, Extended Work Shifts and the Risk of MVC, NEJM, 2005
 Near Misses Rate ( per 1000 commutes ) Nodding w/driving9.3%6.6% Nodding at STOP16.5%10.2% L Barger, Extended Work Shifts and the Risk of MVC, NEJM, 2005")
11
Heavy Night Call = 0.05% Blood Alcohol ? Pediatric residents – 4 week rotations 4 conditions: –light call, light call with alcohol –Heavy call, heavy call with placebo Evaluated on 3 tasks (driving simulator) –One training session at week 3 –Test at week 4 –Test after placebo/alcohol Conclusions: –Light call vs. Heavy call reaction times ↓ 10%, lane variability ↑ 13-27% –Light call & alcohol vs. Heavy call Equivalent to blood alcohol of 0.04 -0.05 JT Arnedt, Neurobehavioral Performance of Residents, JAMA, 294, 2005
 –One training session at week 3 –Test at week 4 –Test after placebo/alcohol Conclusions: –Light call vs. Heavy call reaction times ↓ 10%, lane variability ↑ 13-27% –Light call & alcohol vs. Heavy call Equivalent to blood alcohol of JT Arnedt, Neurobehavioral Performance of Residents, JAMA, 294,")
13
Work Hours and Reducing Fatigue- Related Risk: Good Research vs. Good Policy “ The authors rightly assert that the majority of studies in the area can be characterized as poorly controlled and based primarily on subjective, introspective, and poorly defined dependent measures.” - Editorial: Drew Dawson PhD, Phyllis Zee MD, PhD JAMA Sept 2005

14
Causes of Medical Error Survey: June 2003 821 / 1440 surveys returned –# adverse events, describe most recent AE, mistake Causes: –Inadequate supervision (20%) –Working too many hours (19%) –Problems with hand-offs (15%) –Census too high (12%) –Cross-covering too many pts (5%) R Jagsi, Residents report of Adverse Events and their causes, Arch Int Med, 2005
 –Working too many hours (19%) –Problems with hand-offs (15%) –Census too high (12%) –Cross-covering too many pts (5%) R Jagsi, Residents report of Adverse Events and their causes, Arch Int Med, 2005")
15
80 Hour Work Week Resident Education & Patient Safety PRO Rested, better learner Better quality of life Rested residents Safer work environment CON Insufficient clinical volume ↑ work intensity, ↑ errors Man power Duration of training? Errors of sign-out ↑ work intensity, ↑ errors Competence? Cost

16
Fatigue in trauma surgeons Psychomotor and cognitive skills of trauma residents and attending surgeons evaluated pre-call and post- call Call-associated fatigue associated with increased error rates in the cognitive skills domain, although less so in attending surgeons. Gerdes et al. The effect of fatigue on cognitive and psychomotor skills of trauma and attending surgeons. Amer J Surg 2008; 196:813-820

18
ABSITE and Resident Hours Brown / RIH

19
80 Hour Work Week Resident Well-being, Patient Care & Resident Education Survey of internal medicine residents; 2001 / 2004 73% response rate Surveys –Maslach Burnout Inventory –Career Satisfaction survey –Educational satisfaction L Goitein, The Effects of Work-Hour Limitations on Resident Well-being…, Arch Int Med, 2005

20
P = 0.05 P = 0.02 L Goitein, The Effects of Work-Hour Limitations on Resident Well-being…, Arch Int Med, 2005

21
80 Hour Work Week Resident Well-being, Patient Care & Resident Education Patient care: –“cutting corners” to leave hospital on time –Less active treatment of patients 2 nd x-cover –Overall: negative (37%) – neutral (34%) – positive (29%) Resident education –70% felt less time for attending teaching –81% missing conferences –Overall: negative (47%) – neutral (21%) – positive (32%) L Goitein, The Effects of Work-Hour Limitations on Resident Well-being…, Arch Int Med, 2005
 – neutral (34%) – positive (29%) Resident education –70% felt less time for attending teaching –81% missing conferences –Overall: negative (47%) – neutral (21%) – positive (32%) L Goitein, The Effects of Work-Hour Limitations on Resident Well-being…, Arch Int Med, 2005")
22
Duty Hour Reform and Safety An observational study of all patients (318,636) admitted to VA Hospitals (121) over 5 years. Duty hour reform associated with mortality improvement for 4 common medical conditions No associated benefit for surgical patients Volpp et al. Mortality among patients in VA Hospitals in the First 2 years following ACGME resident duty hour reform. JAMA 2007; 298:284-992

23
Fatigue and Distress Fatigue and distress have been shown to be associated with medical errors Prospective longitudinal study of medical residents at Mayo clinic Higher levels of fatigue and distress independently associated with self-perceived medical errors West CP, et al. Association of resident fatigue and distress with perceived medical errors. JAMA 2009;302:1294-1300.

24
Doctors and Distress

25
Summary 80 hour work week Residents, especially junior residents, are happier. We should see a dividend with residents safer on the roads. Data on performance of tasks is mixed: –No appreciable deterioration of skills / procedures –Some decrement in learning of new skills Data on maintenance and acquisition of cognitive function when fatigued also mixed. Positive effect on patient safety is oversimplified.

26
Summary Sleep & Fatigue Drowsiness, sleepiness, and fatigue cannot be eliminated in residency, but can be managed. Recognition of sleepiness and fatigue and use of alertness management strategies are simple ways to help combat sleepiness in residency. Be aware that personal and professional distress affects performance. When fatigue and distress affect your performance or health, talk to your supervisors and program director.

27
Fatigue and Resident Education Thomas Miner, MD, FACS Associate Program Directory, Surgery Residency Director of Surgical Oncology Assistant Professor of Surgery Warren Alpert Medical School at Brown University

28
© American Academy of Sleep Medicine American Academy of Sleep Medicine Alertness Management Strategies

29
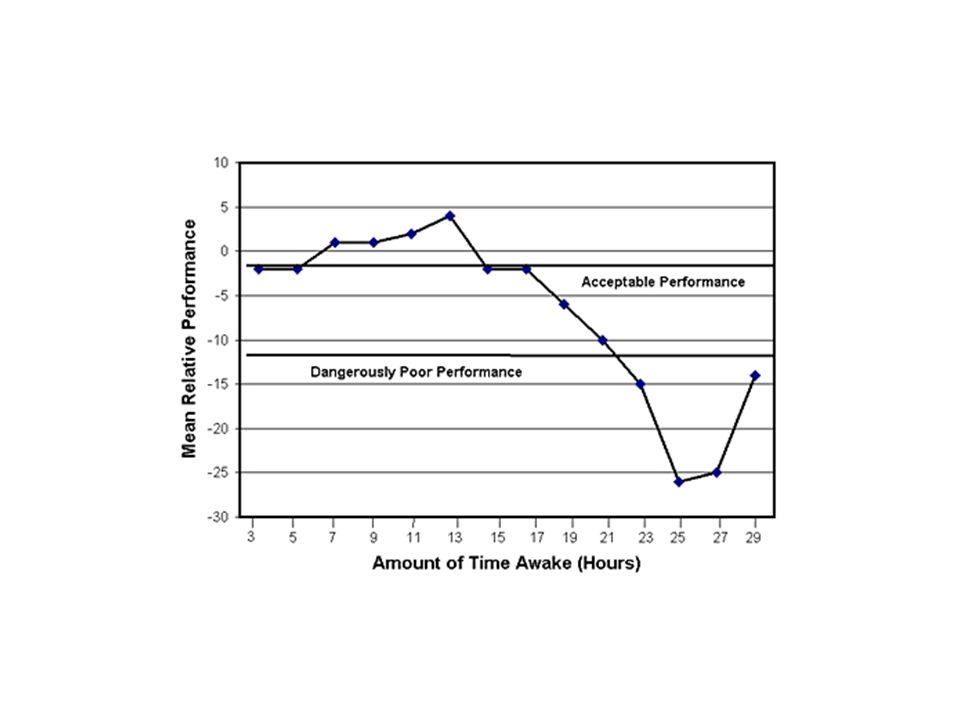
Sleep Sleep is as necessary as food or water, and no matter how much we try we cannot eliminate the need for sleep. We cannot reduce the amount of time we spend asleep without adverse consequences. Without sufficient sleep we can quickly become vulnerable to illnesses, errors, and accidents. Alertness and performance are directly related to quality and quantity of sleep.

30
Sleepiness Myths and Misconceptions Myth: People can tell how tired they are. Fact: Studies show that sleepy people underestimate their level of sleepiness and overestimate their alertness Misconception: People are aware when they are not functioning up to par. Fact: The sleepier you are, the less accurate your perception of degree of impairment. Fact: You can fall asleep briefly (“micro sleeps”) without knowing it.
 without knowing it..")
31
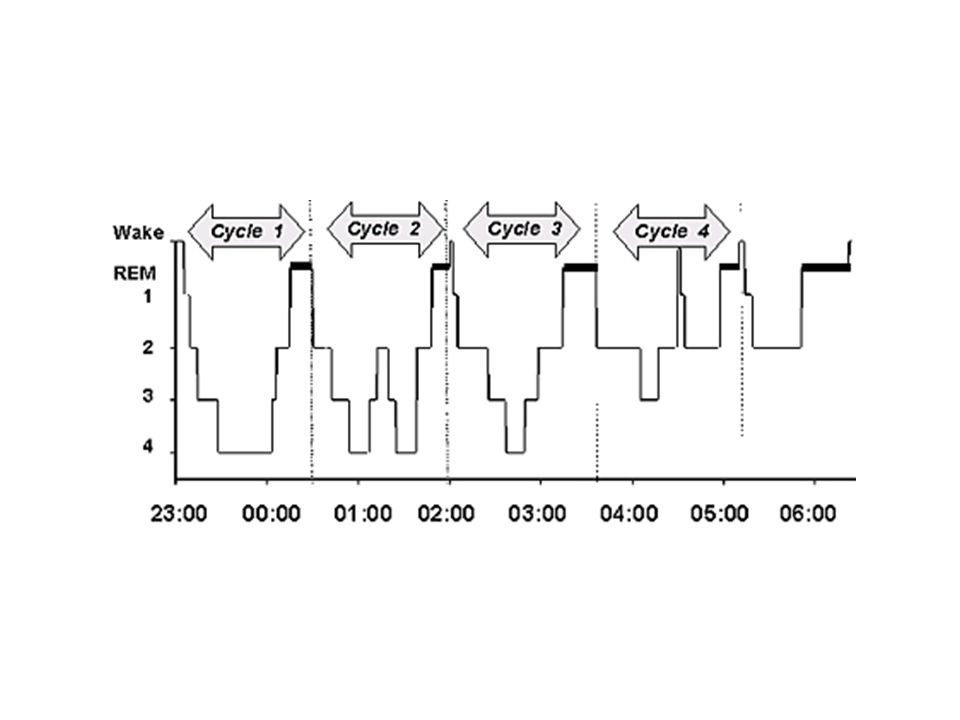
Sleep Architecture Stage 1 – “Mirco-sleep” Stage 2 – 45-55% of sleep Stage 3 – Delta waves on EMG, transition to Stage 4, ↑ Growth hormone Stage 4 – Delta sleep, deepest stage, 10-15% of sleep, ↑ Growth hormone Stage 5 – REM, dreaming, EMG looks like stage 1, allows organization and consolidation of memory

33
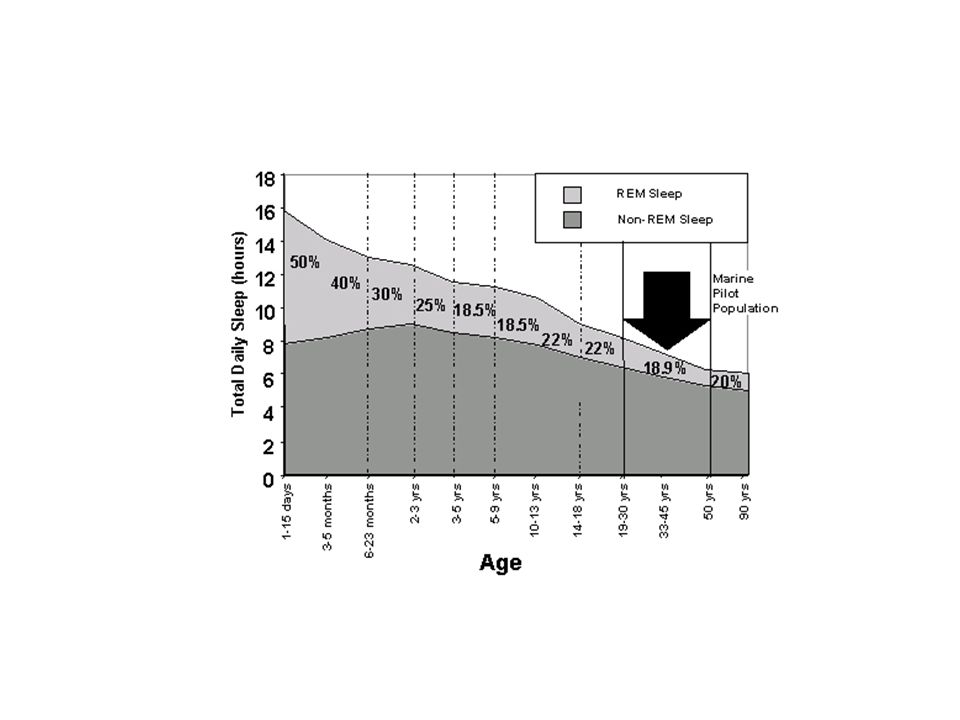
Sleep Myths and Misconceptions Everyone needs 8 hours You can store sleep –I can manage it Need for sleep decreases with age

35
Adapted from Shapiro et al., 1997 Duration of Sleep for Time of Day Sleepiness Over the 24-hour Cycle

36
How do you treat it? Get good sleep “Power” naps Appropriate drugs: i.e. strategic caffeine Smart driving habits

37
Healthy Sleep Habits Go to bed and get up at about the same time every day. Develop a pre-sleep routine. Use relaxation to help you fall asleep. Protect your sleep time; enlist your family and friends.

38
Healthy Sleep Habits Sleeping environment: –Cooler temperature –Dark (eye shades, room darkening shades) –Quiet (unplug phone, turn off pager, use ear plugs, white noise machine) Avoid going to bed hungry, but no heavy meals within 3 hours of sleep. Get regular exercise but avoid heavy exercise within 3 hours of sleep.

39
Napping Pros: Naps temporarily improve alertness. Types: –preventative (pre-call) –operational (on the job) Length: –short naps: 30 minutes –long naps: up to 2 hours – no longer than 2’ to avoid grogginess (“sleep inertia”)
 –operational (on the job) Length: –short naps: 30 minutes –long naps: up to 2 hours – no longer than 2’ to avoid grogginess ( sleep inertia ).")
40
Drugs: Do’s and Don’ts Do –Caffeine: strategic, judicious –Hypnotics: may be helpful in specific situations (eg, persistent insomnia) Don’t –using stimulants (methylphenidate, dextroamphetamine, modifying) to stay awake –using alcohol to help you fall asleep; it induces sleep onset but disrupts sleep later on No Data –Melatonin: little data in residents
 Don’t –using stimulants (methylphenidate, dextroamphetamine, modifying) to stay awake –using alcohol to help you fall asleep; it induces sleep onset but disrupts sleep later on No Data –Melatonin: little data in residents")
41
Caffeine Strategic consumption is key Effects within 15 – 30 minutes; half-life 3 to 7 hours Use for temporary relief of sleepiness Cons: –disrupts subsequent sleep (more arousals) –tolerance may develop –diuretic effects
 –tolerance may develop –diuretic effects")
42
Driving While Drowsy Signs Trouble focusing on the road Difficulty keeping your eyes open Nodding Yawning repeatedly Drifting from your lane, missing signs or exits Not remembering driving the last few miles Closing your eyes at stoplights

43
Drive Smart, Drive Safe What works AVOID driving if drowsy. Don’t drive 2 AM to 9 AM. If you are really sleepy, get a ride home, take a taxi, or use public transportation. Take a 20 minute nap and/or drink a cup of coffee before going home post-call. Stop driving if you notice the warning signs of sleepiness. Pull off the road at a safe place, take a short nap.

44
Drive Smart, Drive Safe What doesn’t work Turning up the radio Opening the car window Chewing gum Blowing cold air (water) on your face Slapping (pinching) yourself hard Promising yourself a reward for staying awake
 on your face Slapping (pinching) yourself hard Promising yourself a reward for staying awake")
Similar presentations













 – apathetic (don’t care) – lethargic (can’t be bothered) – irritable (grouchy) Feelings – tired (sleepy)>")








