Download presentation
Presentation is loading. Please wait.

1
Tracheostomy Care Bill Wojciechowski, MS, RRT Department of Cardiorespiratory Care University of South Alabama Mobile, Alabama

2
Tracheostomy care Upper airway functions bypassed when patient has
tracheotomy performed.

3
Upper airway functions
Heat/moisture exchange Thermoregulation Gustation (taste) Olfaction (smell) Filtration Normally the upper airway performs these functions flawlessly.
 Olfaction (smell) Filtration. Normally the upper airway performs these functions flawlessly.")
4
Clinical Complications
Altered or loss of voice Speech & language delays (young children) Loss of smell & taste Compromised nutritional status Impaired swallowing/increased risk of aspiration Secretion control issues/infection Psychological distress Loss of physiologic PEEP Let’s consider some clinical complications associated with a tracheotomy. Loss of physiologic PEEP & compromised gas exchange
 Loss of smell & taste. Compromised nutritional status. Impaired swallowing/increased risk of aspiration. Secretion control issues/infection. Psychological distress. Loss of physiologic PEEP. Let’s consider some clinical complications associated with a tracheotomy. Loss of physiologic PEEP & compromised gas exchange.")
5
ClinIcal Complications
Absence of airflow often creates Frustration Anxiety Psychological distress For children: delayed speech & language development When airflow through the upper airway is absent, normal sensations and pressures are lost or compromised. Absence of airflow through the vocal cords leaves patients without the ability to speak, causing varying degrees of: frustration anxiety psychological distress For children, losing their ability to use their voices during the crucial years of development can lead to significant speech and language delays.

6
Clinical Complications
Absence of airflow decreases sensations Smell Taste Poor appetite Skin health Supplemental feeding Difficulty swallowing Risk of aspiration Patients with tracheotomies also have decreased senses of smell and taste, which can lead to poor appetite and compromised nutritional status. Poor nutrition accelerates skin breakdown at the stoma site and at points along the tracheal wall in contact with the trach tube (cuff/wall and distal tip/wall). These patients sometimes require supplemental feeding through a NG tube or a PEG tube.
. These patients sometimes require supplemental feeding through a NG tube or a PEG tube.")
7
Clinical Complications
Cuffed trach tubes anchor larynx & sometimes interfere with: Laryngeal elevation Epiglottic inversion Airway protection Cuffed trach tubes secure larynx, Deflated cuff: more freedom. A cuffed tracheostomy tube anchors the larynx, causing interference with laryngeal elevation, epiglottic inversion, thereby compromising airway protection. A cuffed tracheostomy tube tethers the larynx, thereby interfering with the movement of the hyoid bone and larynx during swallowing. Studies have shown that the larynx moves more freely when the cuff is deflated than when the cuff is inflated. Consequently, a cuffless trach tube tends to reduce the risk of aspiration.

8
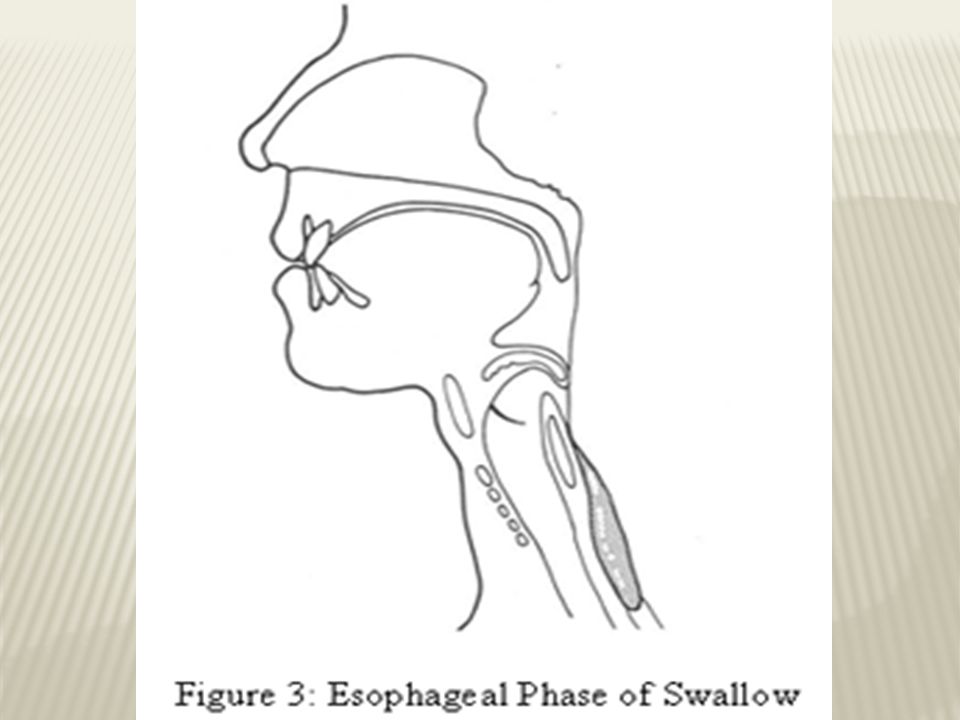
Three phases of normal swallowing: 1) Oral phase 2) Pharyngeal phase 3) Esophageal phase
Let’s look at the normal act of swallowing.

12
Upper airway functions
Normal swallowing (pharyngeal phase): Oral & nasal cavities sealed Vocal cords close Positive pressure generated below cords Air prevented from entering larynx Larynx elevates & moves forward Acts as a lever (mechanical event) Epiglottis seals larynx Food/liquid directed into esophagus The pharyngeal phase begins when a bolus, or packet, of food/liquid reaches the pharynx. During the pharyngeal phase, the following events occur: 1) The palate pushes against the pharynx, separating the oral cavity from the nasal cavity and preventing food/liquid from moving into the nose. 2) The vocal cords close and breathing temporarily ceases. Positive pressure develops beneath them, preventing air from entering the larynx. 3) The pharyngeal muscles constrict to push the “packet” down toward the esophagus. 4) The larynx is pulled upward and forward, acting as a mechanical lever. 5) The epiglottis tilts posteriorly, covering and protecting the laryngeal opening. 6) The upper esophageal sphincter (muscle that controls entry of food/liquid into the esophagus) relaxes, enabling the “packet” to enter the esophagus.
: Oral & nasal cavities sealed. Vocal cords close. Positive pressure generated below cords. Air prevented from entering larynx. Larynx elevates & moves forward. Acts as a lever (mechanical event) Epiglottis seals larynx. Food/liquid directed into esophagus. The pharyngeal phase begins when a bolus, or packet, of food/liquid reaches the pharynx. During the pharyngeal phase, the following events occur: 1) The palate pushes against the pharynx, separating the oral cavity from the nasal cavity and preventing food/liquid from moving into the nose. 2) The vocal cords close and breathing temporarily ceases. Positive pressure develops beneath them, preventing air from entering the larynx. 3) The pharyngeal muscles constrict to push the packet down toward the esophagus. 4) The larynx is pulled upward and forward, acting as a mechanical lever. 5) The epiglottis tilts posteriorly, covering and protecting the laryngeal opening. 6) The upper esophageal sphincter (muscle that controls entry of food/liquid into the esophagus) relaxes, enabling the packet to enter the esophagus.")
13
Upper airway functions
Swallowing with Trach Tube Inserted: Vocal cords close Air flows through trach tube No subglottic positive pressure Reduced sensations in larynx & pharynx Pooling of airway secretions Increase risk of aspiration Most patients OK!! READ SLIDE. Fortunately, most patient’s accommodate having a tracheostomy tube and do not experience an inability to eat and swallow. However, sometimes swallowing dynamics change, requiring adjustment. Most difficulties can be overcome in a short time. Most swallowing problems result from limited elevation of the larynx or poor closure of the epiglottis and vocal cords, which allows food or liquid in the trachea.

14
Clinical complications
Absence of upper airway airflow (inability to nose-breathe) compromises: Heat/moisture exchange Increased secretion viscosity Increased secretion volume Frequent suctioning Increase risk of airway trauma/infection Presence of trach tube stimulates secretions The inability to nose-breathe, interferes with warming, humidifying, and filtering the inspired air. This inability negatively impacts the quality and quantity of pulmonary secretions. Secretions accumulate in the airways, requiring frequent suctioning and increasing the risk of airway trauma and infection. The presence of a trach tube acts as a foreign body in the trachea and stimulates secretion production.
 compromises: Heat/moisture exchange. Increased secretion viscosity. Increased secretion volume. Frequent suctioning. Increase risk of airway trauma/infection. Presence of trach tube stimulates secretions. The inability to nose-breathe, interferes with warming, humidifying, and filtering the inspired air. This inability negatively impacts the quality and quantity of pulmonary secretions. Secretions accumulate in the airways, requiring frequent suctioning and increasing the risk of airway trauma and infection. The presence of a trach tube acts as a foreign body in the trachea and stimulates secretion production.")
15
To overcome these problems HMEs are available.

16
FlexiDerm™ is flexible and has the strongest adhesive properties. It is especially suitable for persons with a deep and/or irregular stoma or those who prefer a very soft and flexible adhesive. Average durability: 48 hours. Regular is an easy-to-remove, easy to handle transparent adhesive that is less flexible than FlexiDerm™ and leaves less residual glue. Recommended for persons with a regular (normal) stoma and skin. Average durability: 24 hours.
 stoma and skin. Average durability: 24 hours.")
17
Clinical complications
With cuff inflated: No physiologic PEEP Possible micro-atelectasis Decreased alveolar ventilation Compromised oxygenation A tracheostomy tube with its cuff inflated does not allow a patient to generate physiologic PEEP. Without physiologic PEEP, the alveoli are prone to micro-atelectasis, which may result in decreased alveolar ventilation and compromised oxygenation.

18
Cuff deflated Cuff inflated Physiologic PEEP Present Physiologic PEEP
A tracheostomy tube with its cuff inflated does not allow a patient to generate physiologic PEEP. Without physiologic PEEP, the alveoli are prone to micro-atelectasis, which may result in decreased alveolar ventilation and compromised oxygenation. Physiologic PEEP Present Physiologic PEEP Absent

19
Tracheostomy Care Inspect stoma daily: irritation/inflammation.
Tracheostomy care is done every 8 to 12 hours and PRN. Avoid dressings trapping moisture. Check secretions: white & clear; greenish-yellow Odor often indicates infection. Assess need for suctioning q2h. Stoma Care The stoma should be inspected daily for signs of irritation and inflammation. The site must be maintained clean and dry through careful attention to replacing soiled ties and removing secretions that collect around or under the tracheostomy tube plate. Dressings that trap moisture should be avoided (i.e., gauze pads). At home, mild soap and water applied with a Q-tip is usually sufficient to clean the stoma site. Adherent secretions may be removed with a Q-tip and half-strength hydrogen peroxide and sterile water. NUTRITION The patient should be evaluated for nutritional well-being and wound healing. The relationship among good nutrition, meticulous skin care, and prevention of wound infection should be stressed. The patient with a tracheostomy is at risk of nutritional deficiency, because of altered taste and smell sensations. To counter these problems, the patient is encouraged to maintain good oral hygiene and eat high-calorie snacks, if not medically contraindicated. Maintenance of body weight is one objective measure of nutritional adequacy. Another component of trach care includes READ ABOVE.
. At home, mild soap and water applied with a Q-tip is usually sufficient to clean the stoma site. Adherent secretions may be removed with a Q-tip and half-strength hydrogen peroxide and sterile water. NUTRITION. The patient should be evaluated for nutritional well-being and wound healing. The relationship among good nutrition, meticulous skin care, and prevention of wound infection should be stressed. The patient with a tracheostomy is at risk of nutritional deficiency, because of altered taste and smell sensations. To counter these problems, the patient is encouraged to maintain good oral hygiene and eat high-calorie snacks, if not medically contraindicated. Maintenance of body weight is one objective measure of nutritional adequacy. Another component of trach care includes READ ABOVE.")
20
Tracheostomy Care Signs of Infection:
Yellow or green secretions (pink or blood-tinged) Thicker mucus Greater volume of mucus Stoma site bleeding Foul odor from stoma Febrile patient Pulmonary congestion Increased RR Listlessness Discomfort with trach/tender stoma site
 Thicker mucus. Greater volume of mucus. Stoma site bleeding. Foul odor from stoma. Febrile patient. Pulmonary congestion. Increased RR. Listlessness. Discomfort with trach/tender stoma site.")
21
Cleaning inner cannula
PROCEDURE

22
Clean inner cannula 1. Loosen inner cannula. 2. Hold outer cannula with one hand. Turn inner cannula to right with other hand to unlock.

23
Clean inner cannula 3. Remove the inner cannula by steadily pulling it down and toward your chest until it is out.

24
Clean inner cannula 4. Place inner cannula in the solution of hydrogen peroxide & normal saline, and don sterile gloves.

25
Clean inner cannula 5. Use trach brush, or pipe cleaner, to clean inner cannula of mucus and dried secretions.

26
Clean inner cannula 6. Place it in bowl of normal saline (NS). 7. Shake off excess NS. Moisture will act as lubricant during inner cannula reinsertion. Do not dry inner cannula. Some RTs advocate drying it.
. 7. Shake off excess NS. Moisture will act as lubricant during inner cannula reinsertion. Do not dry inner cannula. Some RTs advocate drying it.")
27
Clean inner cannula 8. Reinsert inner cannula, keeping curved portion facing downward.

28
Clean inner cannula 9. Lock inner cannula into position. 10. Wash bowls thoroughly and allow to air dry. Soak trach brush soak in hydrogen peroxide-NS solution &, rinse with NS. Air to dry. Discard pipe cleaners.

30
Cuff Pressure Goal: maintain cuff pressure below tracheal mucosal capillary perfusion pressure which is: 25 to 30 mm Hg. Cuff pressure maintained: 20 to 25 mm Hg, or 25 to 35 cm H2O Higher cuff pressures Cut off tracheal mucosal blood flow Tracheal wall damage (necrosis/tracheomalcia)
")
31
CPR - Tracheostomy Caregivers must receive CPR training.
Suction if indicated. Change trach tube if clogged. Spare tubes (cuffless &/or cuffed): same size & 1 size smaller Pinch nose & mouth (cuffless trach). 2 breaths with manual resuscitator/mouth-to-trach/mouth-to-stoma: STOMA LEAK Mouth-to-mouth/bag-mask with finger over stoma: STOMA LEAK READ SLIDE compression-vent ratio A cuffed trach tube should be inflated and a manual resuscitator used. With cuffless trach tube inserted, remove it & replace it with cuffed tube if it’s available.
: same size & 1 size smaller. Pinch nose & mouth (cuffless trach). 2 breaths with manual resuscitator/mouth-to-trach/mouth-to-stoma: STOMA LEAK. Mouth-to-mouth/bag-mask with finger over stoma: STOMA LEAK. READ SLIDE compression-vent ratio. A cuffed trach tube should be inflated and a manual resuscitator used. With cuffless trach tube inserted, remove it & replace it with cuffed tube if it’s available.")
32
Tracheostomy & Speech Fenestrated: Weaning Speech Granuloma formation
Increased risk of aspiration

33
Tracheostomy & Speech Some space around tube Snug fit: tube too large
non-fenestrated: poor or no speech

34
Tracheostomy & Speech Passy-Muir valves.
The "No Leak" design of the Passy-Muir Valves means that the valve is always in a closed position until the patient inhales. The valve opens easily with less than normal inspiratory pressures and closes automatically at the end of the inspiratory cycle without air leak and without patient expiratory effort. Some patients immediately adjust to breathing with the valve. Others need to gradually increase the time the valve is worn. More resistance is encountered exhaling around the tracheostomy tube. Exhalation is more difficult than breathing out through the tracheostomy tube. Patients may need to build up the strength to use the valve.

35
A Passy-Muir valve is a one-way valve that attaches to the outside opening of the tracheostomy tube and allows air to pass into the trach tube during inspiration, but not through it during expiration. The valve opens when the patient inspires. When the patient exhales, the valve closes and air flows around the tracheostomy tube, up through the vocal cords allowing vocalization. The patient exhales through the mouth and nose instead of the tracheostomy tube. The design creates a protective column of air in the tracheostomy tube which resists secretions from moving up the tube and occluding the valve. Instead, secretions may be coughed up around the tube and expectorated or suctioned from the mouth.

36
Tracheostomy Tube Precautions
Use extreme caution with baths and water No swimming Avoid powder, talc, chlorine bleach, ammonia, aerosol sprays, or colognes and perfumes Prevent foreign objects from entering trach tube The PMV O2 adapter is small, lightweight, clear and snaps onto both the Clear and Purple Tracheostomy and Ventilator Speaking Valves and is easily removed when not in use. Oxygen is delivered in front of the diaphragm of the PMV to avoid complications associated with devices that provide continuous flow behind the diaphragm of a speaking valve which may include air trapping, drying of secretions and possible ciliary damage.

37
Tracheostomy tube precautions
Avoid dust Avoid sand and beach Watch play with other children to assure toys, fingers or other foreign bodies are not put into trach and trach is not pulled No contact sports Frequent hand washing

38
Education Teach airway anatomy Teach about equipment Teach CPR
Teach infection control Teach humidification Teach suctioning Teach about speaking valves/fenestrated trach tubes Teach communication through speech therapy

Similar presentations











 – Oral-tracheal – Naso-tracheal Tracheostomy (trach) 1.>")









 Amended 2012.>")
