Download presentation
Presentation is loading. Please wait.

1
Susanna Shouls, Irene Carey, Adrian Hopper AMBER care bundle design team Guy’s and St Thomas’ Foundation Trust April 2014 International Forum The AMBER care bundle for patients whose recovery is uncertain

2
Anita Hayes, Transforming End of Life Care in Acute Hospitals Programme, NHS Improving Quality Peter Kennedy, Cliff Hughes, Bernadette King and Amanda Walker Commission for Clinical Excellence, New South Wales, Australia Contributors

3
Case-note review (14/20 consecutive deaths) (adapted 2x2 matrix review) Focus on treatment Many patients likely to die while ongoing active medical therapy Decision making/ escalation planning, patient/carer involvement inconsistent Communication flows within (between staff) and between organisations 3 Source: GSTFT, 2010
 (adapted 2x2 matrix review) Focus on treatment Many patients likely to die while ongoing active medical therapy Decision making/ escalation planning, patient/carer involvement inconsistent Communication flows within (between staff) and between organisations 3 Source: GSTFT, 2010")
4
Care bundles and reliability A care bundle: - 4/5 components - Can be rapidly answered yes/no - Based on good evidence or self evident good practice All or nothing Locally implemented / quality controlled Resar R, Griffin F, Haraden C, et al. Using Care Bundles to Improve Health Care Quality. IHI Innovation Series white paper. Cambridge, Massachusetts: Institute for Healthcare Improvement 2012. (www.ihi.org)www.ihi.org

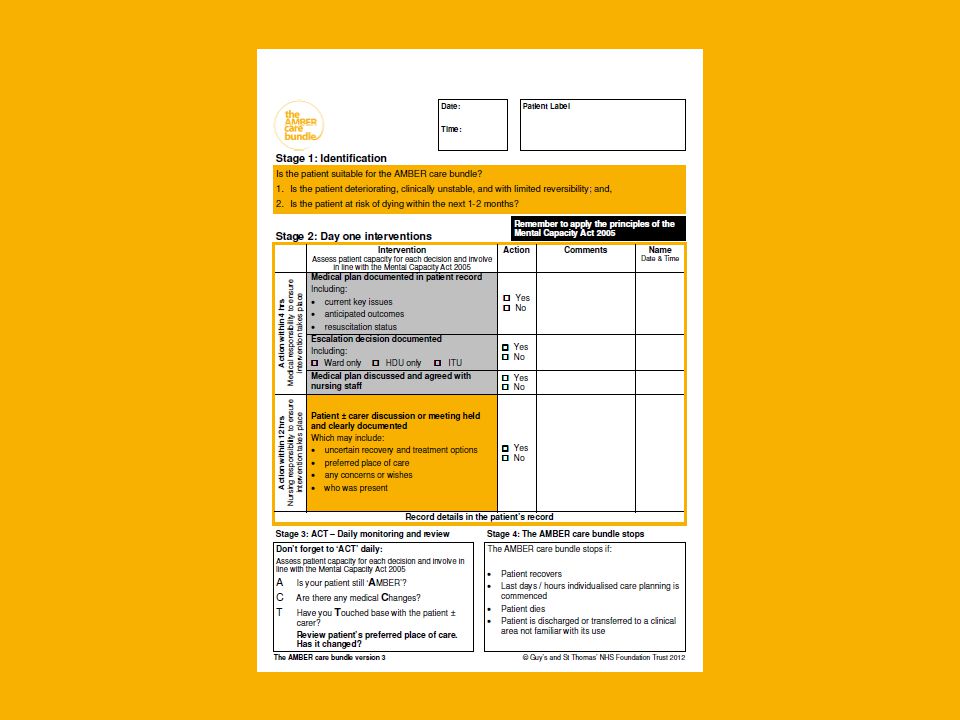
5
5

6
A standardised approach to individualised care 6

9
Why focus on hospitals? 52% of people die in hospital in England More likely to be in inpatient in the last year of life than any other time in adult life Census study of 25 hospitals in Scotland of inpatients (2014) –28.2% died within 1 year –16.2% within 3 months –http://pmj.sagepub.com/content/early/2014/03/17/0269216314526443.a bstracthttp://pmj.sagepub.com/content/early/2014/03/17/0269216314526443.a bstract –http://www.endoflifecare-intelligence.org.uk/home 9
 –28.2% died within 1 year –16.2% within 3 months – bstracthttp://pmj.sagepub.com/content/early/2014/03/17/ a bstract – 9.")
10
Proxy measure of quality of care : death in usual place of residence About 80% of those who had expressed a preference stated their own home was their preferred place to die but only half of these actually died at home (49%). In England, hospital is the most common place of death (52%). VOICES survey, 2012. Published 2013. Office for National Statistics.
. VOICES survey, Published Office for National Statistics..")
11
“Uncertain recovery” 11

12
HOSPITAL LEVEL STRATEGIC CAPABILITY KEY ENABLERS INTERVENTION AT EVERY LEVEL WARD IS THE MICROSYSTEM OF FOCUS Transforming End of Life Care in Acute Hospital National Programme: creating the receptive context for change at the level of the microsystem PULL NOT PUSH FOR CHANGE

13
‘HOW TO’ 3 MODULES Getting Started End of Life Care Pathway Steps 1 - 6 How to sustain ENABLERS Advance care planning Care for patients whose recovery is uncertain and are at risk of dying in 1-2 months - AMBER care bundle Electronic palliative care coordination systems (EPaCCS) Rapid Discharge Home Care of the dying patient- individualised last days of life care plans METRICS Organisational Ward Spread at Feb 2013 x 71 Trusts across England Transforming End of Life Care in Acute Hospitals programme
 Rapid Discharge Home Care of the dying patient- individualised last days of life care plans METRICS Organisational Ward Spread at Feb 2013 x 71 Trusts across England Transforming End of Life Care in Acute Hospitals programme")
14
Jun 10 How to guide Feb 2012 East Midlands SHA: feasibility study Launch Sep 11 Regional workshops: cascade. Early intervention package, resources + 2 x workshop design, monthly calls Development of a faculty and regional support.

15
15 Australia … 8 hospitals New South Wales

16
Implementation package Board sign up Standardised implementation –Clinical leadership (palliative care ++) –Workshop, materials, minimum data set –Network support Ward by ward with clinical facilitation 16
 –Workshop, materials, minimum data set –Network support Ward by ward with clinical facilitation 16")
17
How many patients may be suitable for the AMBER care bundle? N=212, 10 hospitals Source: Baseline audit AMBER network. 2013 Retrospective review of deceased patient records, excludes critical care Australia 70% England

18
Initial findings: improved processes 18 N= 154, 10 hospitals N= 96, 3 hospitals 18 N= 154, 9 hospitals N= 105, 4 hospitals Source: Baseline and follow-up audit AMBER network. 2013

19
Overall outcome: eg from a network hospital 19 Hospital collected 100% data for patients receiving care supported by the care bundle N=555, Sep 2012-Oct 2013 46% patients died 39% discharged

20
Patient, relative feedback It was difficult to hear but I knew wasn’t feeling better, I know now what's happening to me Knowing that he may not recover – (we just thought he would) earlier allowed us time to talk about what would happen to the house, and bank accounts. Which was important because at the end he couldn’t talk to me anymore Source: AMBER network hospital trust, 2013

21
Staff feedback 21 I didn’t think the patient would deteriorate so quickly. I am glad I was able to talk to the relatives and prepare them for what may happen. When I mention to a doctor that I think a patient’s recovery is uncertain and may be suitable for AMBER the doctor listens and revaluates the patients medical plan.

22
Patients who are discharged 30d emergency readmission rates Before implementation 43% (n=40, 6 hospitals, patients suitable) After implementation 11% (n=25, 3 hospitals, patients received care supported by AMBER care bundle) 22 Source: AMBER care bundle design team, GSTFT June 2013
 After implementation 11% (n=25, 3 hospitals, patients received care supported by AMBER care bundle) 22 Source: AMBER care bundle design team, GSTFT June 2013")
23
?Social movement Connects to real clinical experience Expectation of peer support Ownership & emergent clinical leadership Community of practice Standard programme & implementation Local pace Set by hospitals Rapid adoption: all teach all learn model

24
24 Context Intervention Implementation Benefits and impact Unintended consequences Challenges and opportunities Neuberger review Evaluation and evidence

25
"I don't think we should tell them what we're going to do in advance. Let them think. Worry. Wonder. Uncertainty is the most chilling thing of all." Vernon A. Walter A former United States army officer and diplomat.

26
www.ambercarebundle.org ambercarebundle@gstt.nhs.uk AMBER care bundle design team Dr Irene Carey Dr Adrian Hopper Michelle Morris Susanna Shouls Helen Thurkettle NHS Improving Quality / NHS England Anita Hayes Dr Bee Wee Clinical Excellence Commission, NSW Australia Amanda Walker Bernadette King AMBER network hospitals and the AMBER faculty 26

Similar presentations