Download presentation
Presentation is loading. Please wait.

1
The Aphasias Woodford A. Beach, MS, CCC/SP Senior Speech-Language Pathologist Clinical Instructor, Otolaryngology MCVH&P of VCUHS May 3, 2002

2
Objectives Define aphasia Review Boston aphasia classification Consider atypical aphasias Note other neurogenic communication disorders

3
Aphasia acquired language disorder, that is a CNS disturbance of the capacity to interpret and formulate symbols for communicative purposes secondary to focal brain damage –perisylvian region –dominant hemisphere –not due to diffuse or multifocal dysfunction

4
Aphasia characterized by impairment in connected speech and conversation, auditory comprehension, repetition, naming, reading, & writing

5
What aphasia is not:

6
What aphasia is not: dysarthria apraxia of speech

7
Dysarthria group of speech disorders neurogenic associated with CNS, PNS, muscle pathology

8
Darley, Aronson, & Brown 1975 Dysarthria movement disorder abnormal neuromuscular execution –affects speed, strength, timing, accuracy –affects respiration, phonation, resonance, articulation, and prosody

9
Apraxia of Speech disorder of motor planning absence of aphasia & neuromotor deficits characterized by symptom variability –mutism –difficulty initiating speech –problems in syllable transition –more difficulty in volitional than automatic –more difficulty in long than short –more difficulty in complex than simple

10
Duffy 1995 Apraxia of Speech Often –articulatory struggle –phoneme metathesis –syllable transposition

11
Aphasia is not language of confusion Aphasia is not due to psychiatric disease Aphasia is not due to primary cognitive dysfunction it is focal, and not caused by multifocal or diffuse brain disease

12
Comatose patients are not aphasic

13
Assessment of Aphasia

14
Assessment of Aphasia: Formal Boston Diagnostic Aphasia Examination Western Aphasia Battery Burns Left Hemisphere Inventory Boston Assessment of Severe Aphasia Aphasia Diagnostic Profiles Boston Naming Test Minnesota Test for the Differential Diagnosis of Aphasia

15
Assessment of Aphasia: Informal Conversation & Connected Speech –fluent –hyperfluent (logorrhea or press of speech) –nonfluent –grammatic/paragrammatic/agrammatic –empty –appropriate without dyspragmias
 –nonfluent –grammatic/paragrammatic/agrammatic –empty –appropriate without dyspragmias")
16
Assessment of Aphasia: Informal Conversation & Connected Speech –if there is only minimal speech automatic series (counting, days of week) singing –does the patient engage linguistically
 singing –does the patient engage linguistically")
17
Assessment of Aphasia: Informal Auditory Comprehension –commands 1 part axial 1 part other 2 part 3 part –yes/no questions with known answer orientation bizarre complex

18
Assessment of Aphasia: Informal Repetition –repeat sentences “No ifs, ands, or buts” “They heard him speak on the radio last night” –repeat words vary length and familiarity

19
Assessment of Aphasia: Informal Word Retrieval –confrontation name objects name parts of objects –responsive answer questions –verbal fluency list words belonging to semantic class or beginning with common letter

20
Assessment of Aphasia: Informal Word Retrieval Errors –paraphasias: word substitutions –circumlocutions: talk around target –neologisms: nonwords –stereotypy: restricted subpropositional forms (often yes & no) –frank dysnomia: no response or do not know
 –frank dysnomia: no response or do not know")
21
Assessment of Aphasia: Informal Reading Comprehension –silent reading of command –silent reading of yes/no question –oral reading is not reading comprehension any more than dictation or copying are written expression –If reading comprehension compromised, assess oral reading

22
Assessment of Aphasia: Informal Written Expression –generate sentence given stimulus word –automatic writing (e.g. signature) is not written expression –If writing impaired, assess taking dictation, then copying of words or figures
 is not written expression –If writing impaired, assess taking dictation, then copying of words or figures.")
23
Boston Aphasia Classification Relative sparing vs relative impairment Reading and writing always impaired Differentiate aphasias in –fluency –auditory comprehension –repetition –naming

24
Classic Boston Aphaisas Nonfluent –Broca –Global –Transcortical Motor –Mixed Transcortical (isolation syndrome) Fluent –Wernicke –Conduction –Anomic –Transcortical sensory
 Fluent –Wernicke –Conduction –Anomic –Transcortical sensory")
25
Taxonomy of Nonfluent Aphasias

26
Taxonomy of Fluent Aphasias

27
Disclaimers & caveats re: aphasia taxonomy Receptive/expressive dichotomy invalid –all aphasias have an expressive component –all aphasias have a receptive component If you are binary, use the fluent/nonfluent dichotomy

28
Disclaimers & caveats re: aphasia taxonomy Other taxonomies exist Some researchers argue that aphasia is a unary phenomenon Metter showed that PET scans demonstrate metabolic hypodensities distal to site of lesion (is this diaschisis of von Monokow?) Reliability dogs all taxonomies
 Reliability dogs all taxonomies")
29
Disclaimers & caveats re: aphasia taxonomy Taxonomies often fail to capture characterististics of aphasia which are important therapeutically e.g., Broca’s Aphasia –agrammatism –dysfluency Labels are abbreviations. Describe Sxs!

30
Disclaimers & caveats re: aphasia taxonomy Boston model fails to capture –natural course and evolution of aphasia –severity –localization consistently Boston group admits: –“In many instances (30-40% of unselected cases), inspection of the speech characteristics leads directly to a diagnostic assignment” Albert et al. 1981 –Therefore, are 60-70% aphasias mixed?

31
Disclaimers & caveats re: aphasia taxonomy Research by Nina Dronkers (2000) –Chronic Broca’s N=12 with Broca’s aphasia 2 had lesions sparing Broca’s area 10 others with Broca’s lesion had no persisting Broca’s aphasia Chronic Broca’s Aphasia always involved insula –Chronic Wernicke’s N= 7 with Wernicke’s aphasia 2 had lesions sparing Wernicke’s 7 others with Wernicke’s lesion had no persisting Wernicke’s aphasia Chronic Wernicke’s always has large temporal lesion with destruction of posterior MTG –Data reflect structural lesions in chronic aphasias
 –Chronic Broca’s N=12 with Broca’s aphasia 2 had lesions sparing Broca’s area 10 others with Broca’s lesion had no persisting Broca’s aphasia Chronic Broca’s Aphasia always involved insula –Chronic Wernicke’s N= 7 with Wernicke’s aphasia 2 had lesions sparing Wernicke’s 7 others with Wernicke’s lesion had no persisting Wernicke’s aphasia Chronic Wernicke’s always has large temporal lesion with destruction of posterior MTG –Data reflect structural lesions in chronic aphasias")
32
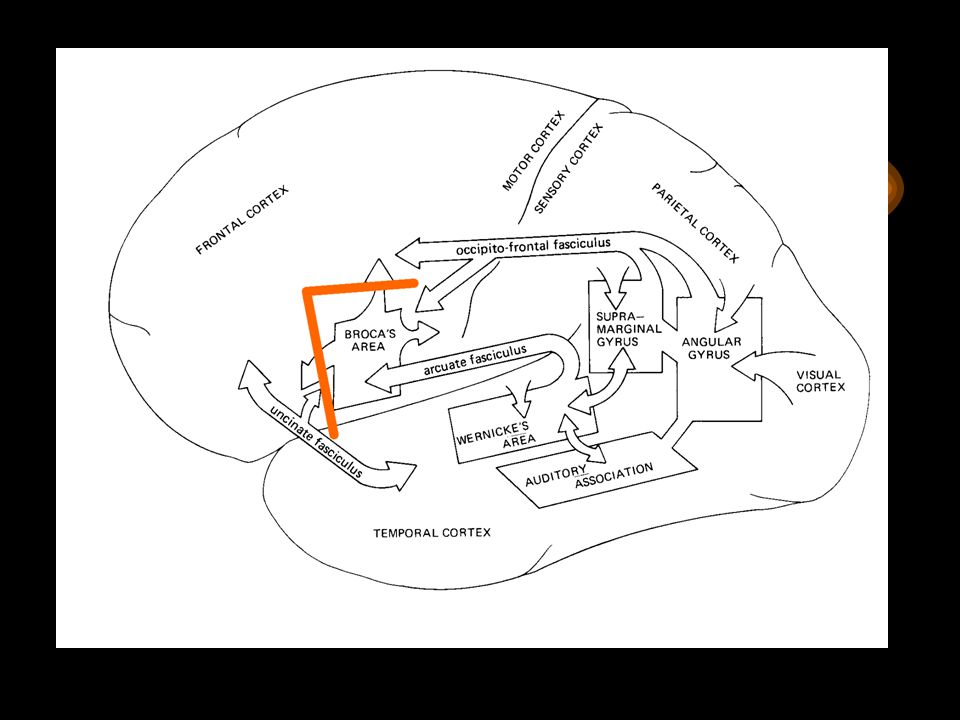
Cortical Organization of Language

33
Localization of Classical Aphasias Broca: third left frontal convolution Global: entire perisylvian region Transcortical Motor: anterior watershed Mixed Transcortical: anterior watershed & posterior watershed

35
Localization of Classical Aphasias Broca: third left frontal convolution Global: entire perisylvian region Transcortical Motor: anterior watershed Mixed Transcortical: anterior watershed & posterior watershed

37
Localization of Classical Aphasias Broca: third left frontal convolution Global: entire perisylvian region Transcortical Motor: anterior watershed Mixed Transcortical: anterior watershed & posterior watershed

39
Localization of Classical Aphasias Broca: third left frontal convolution Global: entire perisylvian region Transcortical Motor: anterior watershed Mixed Transcortical: anterior watershed & posterior watershed

41
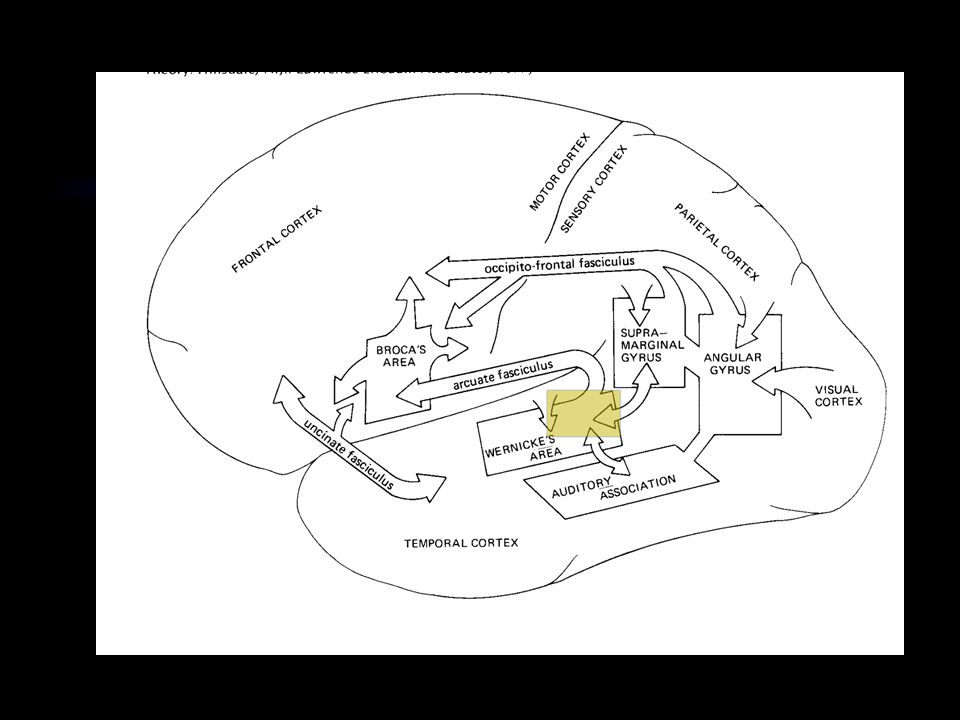
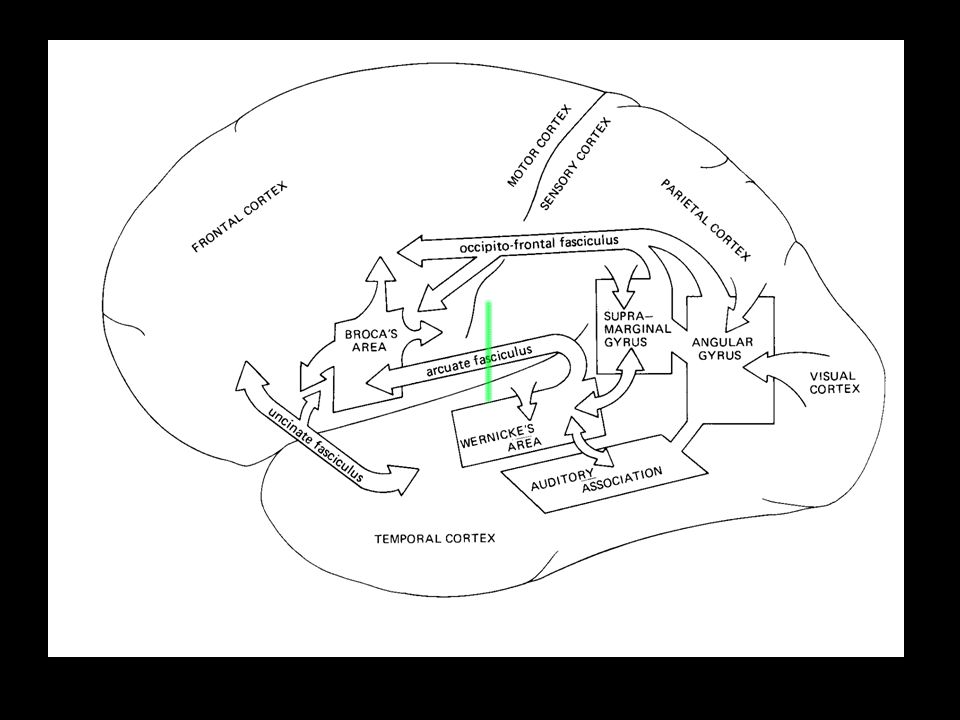
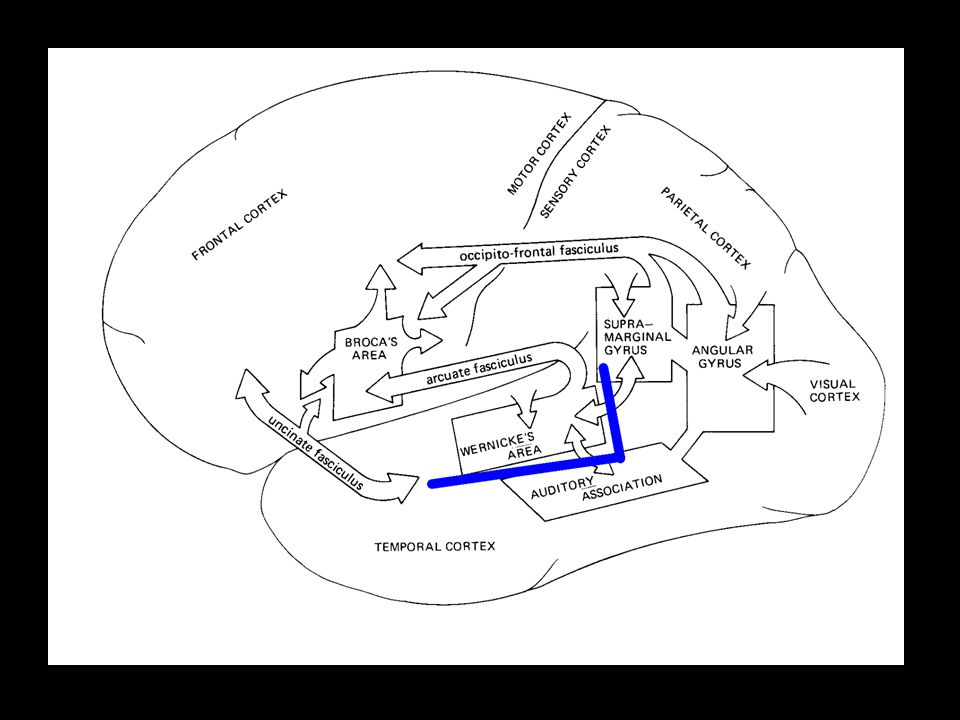
Localization of Classical Aphasias Wernicke: posterior, superior temporal lobe Conduction: archuate fasciculus; inferior parietal lobe Transcortical sensory: posterior watershed Anomic: posterior: temporoparietal?

43
Localization of Classical Aphasias Wernicke: posterior, superior temporal lobe Conduction: archuate fasciculus; inferior parietal lobe Transcortical sensory: posterior watershed Anomic: posterior: temporoparietal?

45
Localization of Classical Aphasias Wernicke: posterior, superior temporal lobe Conduction: archuate fasciculus; inferior parietal lobe Transcortical sensory: posterior watershed Anomic: posterior: temporoparietal?

47
Localization of Classical Aphasias Wernicke: posterior, superior temporal lobe Conduction: archuate fasciculus; inferior parietal lobe Transcortical sensory: posterior watershed Anomic: posterior: temporoparietal?

49
Frattali 2000 Dorsolateral Syndrome Reduced selective attention lack of drive & awareness reduced initiation dynamic aphasia of Luria Localize to frontal dorsolateral cortex –anterior and inferior to Broca’s area

51
Frattali 2000 Aphasia in DLS decreased spontaneous speech limits in amount and range of narrative reduced verbal fluency limited capacity to formulate propositions

52
Frattali 2000 DLS and TMA TMA lesion is larger and less circumscribed. Fewer behavioral manifestations

53
Frattili 2000 Orbitomedial Syndrome Deficit in exclusionary attention utilization behavior impulsive poor inhibition impaired moral judgment localized to frontal orbomedial cortex

54
Subcortical aphasia Thalamic Aphasia fluent with occasional dysfluency paraphasias, neologisms, & word finding impaired repetition intact perseveration Left caudate, putamen, ALIC Aphasia limited spontaneous speech intact repetition mild anomia relatively spared comprehension

55
Atypical Aphasias Aphemia & Anarthria Alexia without agraphia Alexia with agraphia Pure word deafness Pure agraphia

56
Atypical Aphasias Gerstmann’s Syndrome –r/l disorientation –finger agnosia –dyscalculia –dysgraphia Angular Gyrus Syndrome –anomia –alexia –Gerstmann’s Syndrome

58
Nonaphasic Language Disorders TBI Minor hemisphere CVA Dementias Primary progressive aphasia Diffuse & multifocal neurological deficits (encephalopathies) Seizures
 Seizures")
59
Treatment in a Nutshell Aphasia therapy is efficacious –Robey –Frattali It must exceed 2 hours per week (i.e., rehab frequency)
")
60
Treatment in a Nutshell Symptomatic Multimodal Gradually increasing in complexity should focus on both deficits and compensatory strategies should consider communicative handicap

61
Deglutition & Expectoration in the camelid Lama glama

Similar presentations









 Ling 411 – 05.>")



>")

. What hemisphere of the brain is involved in language? Left (for the majority)>")


![Disorders Fluent aphasias [3] Nonfluent aphasias [4] Pure aphasias [1] Watershed.](/14/4364138/big_thumb.jpg "Disorders Fluent aphasias [3] Nonfluent aphasias [4] Pure aphasias [1] Watershed.>")

 is a treatment technique designed to improve the naming abilities by increasing the level of activation within.>")




