Download presentation
Presentation is loading. Please wait.

1
Health and Homelessness: the right to the highest attainable standard of health? Katy Hetherington, Programme Manager Katy.Hetherington@nhs.net Neil Hamlet, Consultant in Public Health, NHS Fife Neil.Hamlet@nhs.net

2
Our vision and mission Our Strategy 2012-17: “A FAIRER HEALTHIER SCOTLAND”

3
Each stop on the Argyll line travelling East represents a drop of 2 years in male life expectancy Source: McCartney G. Illustrating Glasgow’s health inequalities. JECH 2010; doi 10.1136/jech.2010.120451

4
What do we mean by health inequalities? Health inequalities are: Unfair differences in health within the population across social classes and between different populations These unfair differences: Are not random, or by chance, but largely socially determined Are not inevitable.

5
What causes health inequalities? Wider environmenta l influences Economic & work Physical Educ & learning Social & cultural Services Individual experiences Economic & work Physical Educ & learning Social & cultural Services Fundamental causes Global forces, political priorities, societal values leading to: Unequal distribution of power, money and resources INEQUALITIES Effects Inequalities in the distribution of health and wellbeing HEALTH INEQUALITIES Undo MitigatePrevent

6
What is most and least effective in reducing health inequalities? Least likely to be effective Interventions reliant on people opting in; information based campaigns; written materials; messages designed for the whole population; interventions that involve significant price or other barrier Most likely to be effective Structural changes to the environment; legislation, regulatory and fiscal policies; income support, reduced price barriers; accessibility of public services, prioritising disadvantaged groups and individuals; intensive support for disadvantaged population groups; starting young.

7
Substance Misuse Dental Care Foot and skin care Alcohol Abuse Mental Health Issues Nutrition and diet Homelessness Homelessness - a cross-cutting agenda Community Health Partnerships Social Work NHS Acute Services Registered Social Landlords Council Housing Departments Third Sector Agencies Health & Social Care Integration Bodies Alcohol and Drug Partnerships (ADPs)
")
8
Employment Family nurturing (conflict resolution) Education & skills Income maximisation Honour and purpose Coping & resilience Homelessness - a agenda Homelessness - a prevention agenda Social Work NHS Outreach Services Registered Social Landlords Council Housing Departments Third Sector Agencies Health & Social Care Integration Bodies Alcohol and Drug Partnerships (ADPs)
 Education & skills Income maximisation Honour and purpose Coping & resilience Homelessness - a agenda Homelessness - a prevention agenda Social Work NHS Outreach Services Registered Social Landlords Council Housing Departments Third Sector Agencies Health & Social Care Integration Bodies Alcohol and Drug Partnerships (ADPs)")
9
Housing Vol Sector NHS HSCP

10
Homelessness as a public health issue – ScotPHN Report ‘Re-energise’ the health and homelessness agenda Set it in the current policy context – health and social care, focus on inequalities, prevention agenda, homelessness policy and legislative 2005 Health and Homelessness standards Discussion and engagement – housing, voluntary sector, SG, academics, NHS Boards Gaps? What do we want to recommend to Directors of Public Health?

11
Severe and multiple disadvantage ‘Hard Edges’ 2015 – Mapping severe and multiple disadvantage in England “services still categorise people in separate boxes, defined by simple issues…different approaches from services and from policy” Understanding complex lives – Joseph Rowntree Foundation, 2011 ‘There needs to be an integrated response across health, housing and social care’ Early childhood experiences – the roots of many people’s experiences lay within very troubled childhoods.

12
Linkage of Hospital data and Homelessness data in the Kingdom of Fife Bryan Archibald, Senior Information Officer barchibald@nhs.netbarchibald@nhs.net Bryan Archibald barchibald@nhs.net

13
The Data Sources Fife Council HL1 National data set for each homeless application Based on the application (not the number of homeless individuals) NHS Fife Acute Hospitals eOASIS (patient administration system) SMR data submitted to ISD (information Services Division of NHS Scotland) Based on Patient Episodes http://www.scotland.gov.uk/Topics/Statistics/15257/22833
 NHS Fife Acute Hospitals eOASIS (patient administration system) SMR data submitted to ISD (information Services Division of NHS Scotland) Based on Patient Episodes")
14
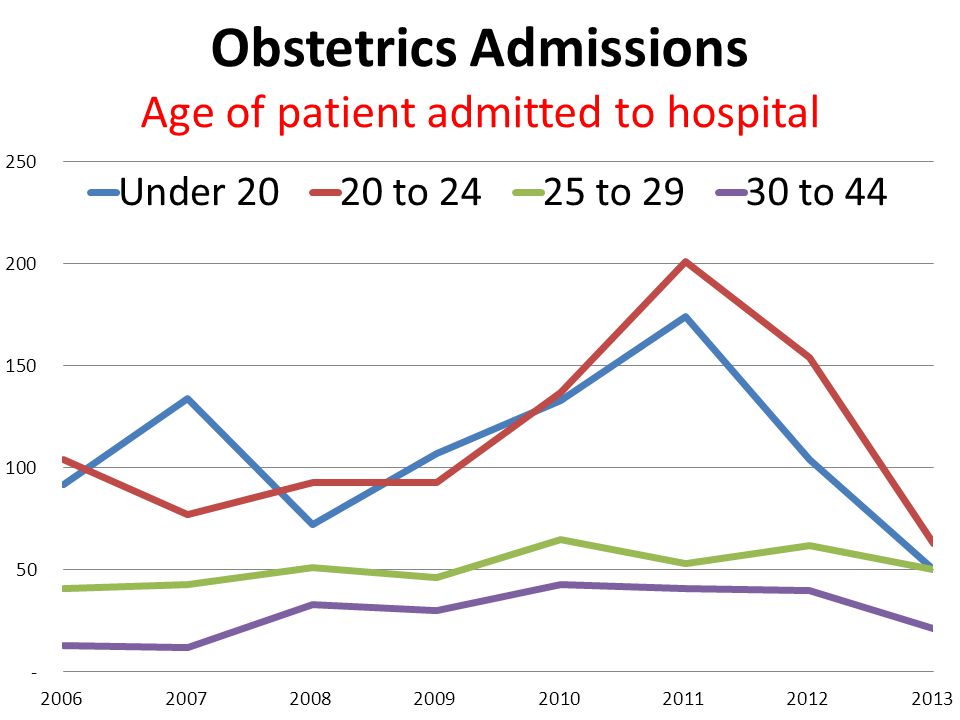
NHS Data (OASIS) A&E (and Minor Injuries Unit [MIU]) Inpatients & Day cases Obstetrics Mental Health Inpatients Outpatients Mental Health Outpatients
![NHS Data (OASIS) A&E (and Minor Injuries Unit [MIU]) Inpatients & Day cases Obstetrics Mental Health Inpatients Outpatients Mental Health Outpatients](http://images.slideplayer.com/13/3946826/slides/slide_14.jpg "NHS Data (OASIS) A&E (and Minor Injuries Unit [MIU]) Inpatients & Day cases Obstetrics Mental Health Inpatients Outpatients Mental Health Outpatients")
19
So far so good but what does this mean? We need a comparator for the homeless populationWe need a comparator for the homeless population Fife’s ‘securely - housed’ populationFife’s ‘securely - housed’ population Try to compare by similar age profileTry to compare by similar age profile Started with Fife population 15-64 as our crude method of ‘standardisation’Started with Fife population 15-64 as our crude method of ‘standardisation’ Further refinements planned in ‘standardisation process’Further refinements planned in ‘standardisation process’ Aiming to compare ‘apples’ with ‘apples’ by security of housing as defined by HL1 registrationAiming to compare ‘apples’ with ‘apples’ by security of housing as defined by HL1 registration

20
The value of shared data analysis ‘Insecurely Housed’‘Securely Housed’

21
Abuse ? Pragmatic ? £££

22
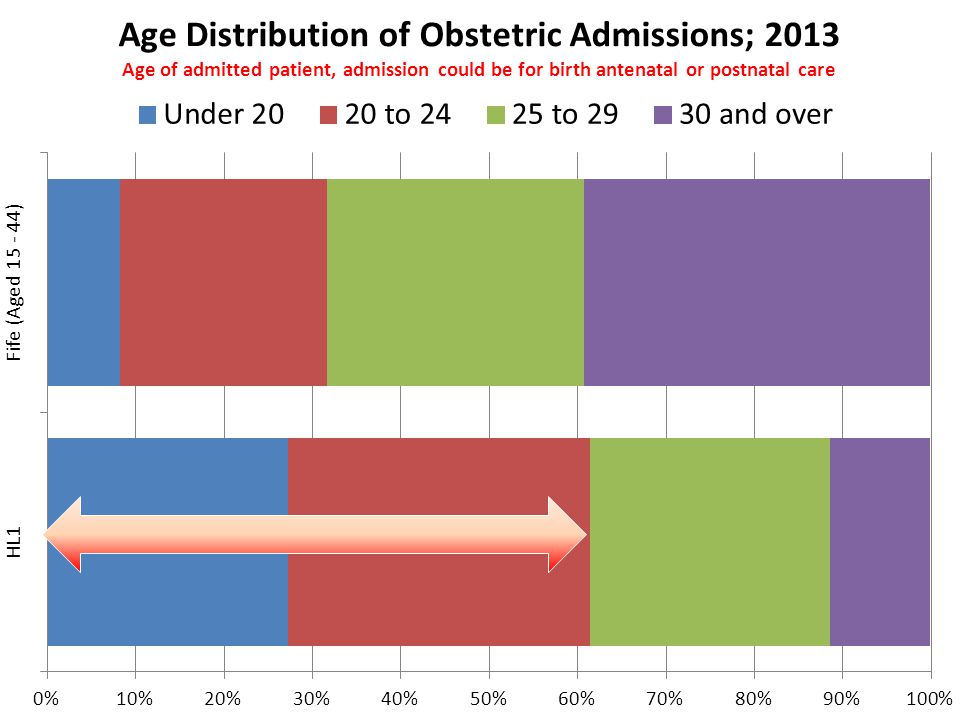
Over 50% are under 30 yrs Over 80% are under 40 yrs

24
£

25
Revolving Hospital Door effect

28
Clear role for Community Safety Partnerships ?

32
Changed address Fearful to open official mail Appointment too early No money for the bus ‘it won’t do any good’ Access / Expectation

33
Inverse Care Law The availability of good medical care tends to vary inversely with the need for it in the population served.” “ The availability of good medical care tends to vary inversely with the need for it in the population served.” “Those who need healthcare least use the services more, and more effectively, than those with the greatest need and those people in the worst health receive the least services.” Julian Tudor Hart 1971

34
What is most and least effective in reducing health inequalities? Least likely to be effective Interventions reliant on people opting in; information based campaigns; written materials; messages designed for the whole population; interventions that involve significant price or other barrier Most likely to be effective Structural changes to the environment; legislation, regulatory and fiscal policies; income support, reduced price barriers; accessibility of public services, prioritising disadvantaged groups and individuals; intensive support for disadvantaged population groups; starting young.

35
Making a Difference On call nurse manager gets a text alert on her work phone when a homeless person is seen in Accident and Emergency Dept. A daily report is now generated listing all the patients in the hospital at 8am who have a temporary homeless accommodation address.

36
'Houseless and Hungry' by Luke Fildes depicting homeless paupers queuing outside the casual ward of a London workhouse Meet needs of safety, nurture, belonging and purpose “We believe that health and homelessness services can work better together to ensure that an individual's health needs are identified and addressed as quickly as possible. NHS acute services currently bear the brunt of the health and other complex problems experienced by those who are homeless. A&E visits per homeless person are four times higher than that of the general public and over a quarter of those surveyed had been admitted to hospital in the previous six months” Rick Henderson, chief executive of Homeless LinkHomeless Link

Similar presentations