Download presentation
Presentation is loading. Please wait.

1
Tumores Ampulares Dr. Alberto Espino Dpto Gastroenterologia UC Sept 02, 2014

3
Es importante examinar la papila? Es recomendado visualizar la segunda porción duodenal incluyendo la papila mayor en toda EDA estándard Detección precoz de enfermedades periampulares y enfermedades pancreatobiliares. Factores de dificultad: – Características anatomicas de D2 – Angulo tangencial – Divertículo periampular – Formación de loop WJG 2013;19: 2037-2043 GIE 2012; 75: 254-260

4
¿Cómo es una papila normal?

5
¿Cuántos de ustedes examinan la papila duodenal durante una EDA ?

7
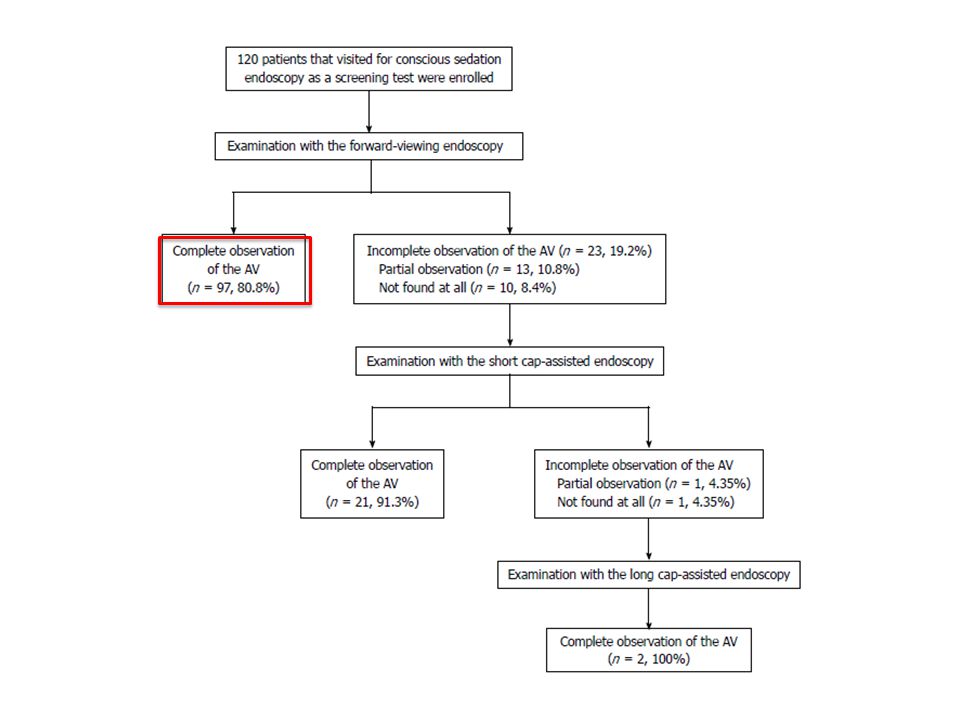
Examen de ampolla de Vater o papila mayor Completo, incompleto y no visualizada WJG 2013

17
Additional short CAE was performed in patients in whom we could not completely visualize the AV. This group included 13 patients (10.9%) with partial observation of the AV and 10 (8.3%) in which the AV was not found. Short CAE permitted a complete observation of the AV in 21 of the 23 patients (91.3%). Patients in whom visualization of the AV failed with short CAE had satisfactory outcomes by replacing the short cap with a long cap. The additional time for CAE took an average of 141 ± 88 s. There were no complications and no significant mucosal trauma.
 with partial observation of the AV and 10 (8.3%) in which the AV was not found. Short CAE permitted a complete observation of the AV in 21 of the 23 patients (91.3%). Patients in whom visualization of the AV failed with short CAE had satisfactory outcomes by replacing the short cap with a long cap. The additional time for CAE took an average of 141 ± 88 s. There were no complications and no significant mucosal trauma..")
18
Periampullary Tumours Relatively rare – Annual incidence of 3000 cases in US 1 – prevalence rates estimated to be 0.04 to 0.12 % in autopsy series 95% adenomas (villous and tubulovillous) – 5% neuroendocrine tumours, paragangliomas etc Occur sporadically or more commonly in the setting of FAP (80% lifetime incidence, 4% risk of malignancy) Stepwise progression to adenocarcinoma – 25 - 80% for sporadic adenomas 2 1. Martin Gastro Intest Clin N A 2003 2. Burke GIE 1999

19
Clinical features – Asymptomatic – particularly in FAP undergoing surveillance – Jaundice, fluctuating LFT’s, nonspecific discomfort, anorexia, pancreatitis, GI bleeding/anaemia

20
Management Surveillance FAP patients with small lesions (<1cm) Surgery – Radical resection – Local excision Endoscopic excision Palliative stenting
 Surgery – Radical resection – Local excision Endoscopic excision Palliative stenting")
21
Pancreaticoduodenectomy Historical gold standard (1909) Definitive Eliminates need for surveillance (sporadic) Outcomes – Recurrence rates for adenoma ≈ 0 – Adverse events Operative mortality 0-9% Morbidity 25-65% (anastomotic dehiscence and fistulae) Related to case volume
 Definitive Eliminates need for surveillance (sporadic) Outcomes – Recurrence rates for adenoma ≈ 0 – Adverse events Operative mortality 0-9% Morbidity 25-65% (anastomotic dehiscence and fistulae) Related to case volume")
22
Local surgical excision Entails mobilization of the duodenum and longitudinal duodenotomy - followed by…. (i) Simple excision of the ampullary neoplasm (ii)Extended excision (including adjacent duodenal and ductal tissue) Lower complications rates(1) – Mortality 0-4% – Morbidity14-27% Recurrence rates up to 30%(2) 1.de Castro Surgery 2004 2.Winter J Gastrointest Surg 2010
 Simple excision of the ampullary neoplasm (ii)Extended excision (including adjacent duodenal and ductal tissue) Lower complications rates(1) – Mortality 0-4% – Morbidity14-27% Recurrence rates up to 30%(2) 1.de Castro Surgery Winter J Gastrointest Surg")
23
Endoscopic ampullectomy Described in the late 1980’s Developed as a less invasive alternative ASGE guideline 2007 – Outcomes Largely retrospective data – Success rates for removal 46-92%

24
Outcomes Ceppa Annals of Surg 2013

25
Complications El Hajj Gastrointest Endos Clin N Am 2013

26
Patient Selection Endoscopy – Suspicious features – induration and rigidity of papilla, ulceration, submucosal mass effect, friability – Biopsy 1,2 High sensitivity (>90%) for detecting the presence of an adenoma Low sensitivity for confirming adenocarcinoma – missing the diagnosis in 30% The frequency of malignant foci in ampullary adenomas is 26-30% Accuracy improved – Number of biopsies > 6 – Biopsies taken after ERCP 1.Artifon GIE 2009 2.Sauvanet Am J Surg 1997
 for detecting the presence of an adenoma Low sensitivity for confirming adenocarcinoma – missing the diagnosis in 30% The frequency of malignant foci in ampullary adenomas is 26-30% Accuracy improved – Number of biopsies > 6 – Biopsies taken after ERCP 1.Artifon GIE Sauvanet Am J Surg 1997")
27
Staging – EUS +/- IDUS Depth of involvement – T stage Intraductal extension Periampullary LN’s – CT/MRI - nodal staging and metastases – ERCP Main role is at the time of resection to assess intraductal extension (PD and CBD)
")
28
Proposed algorithm

Similar presentations














>")









 Lok Hon Ting (Prince of Wales Hospital)>")




