Download presentation
Presentation is loading. Please wait.

1
DURNER L.,BOURDOUMIS A., MASOOD J., BUCHHOLZ N. ROYAL LONDON HOSPITAL, BARTSHEALTH NHS TRUST ROYAL DEVON AND EXETER NHS TRUST HOMERTON UNIVERSITIY HOSPITAL NHS TRUST Handling thromboprophylaxis minimally invasive stone procedures

2
Introduction multiple co-morbidities cardiology procedures get more complex Antiplatelets Anticoagulation cronic bleeding disorder peri- and post- operative thromboprophylaxis low / intermediate / high risk

3
Purpose current evidence practical guide for thromboprophylaxis dosing and duration modifications anticoagulation regimens dependent on planned procedure

4
Materials and Methods systematic review and evidence-based research of the literature. Key words: anticoagulation treatment, antiplatelet agents, stone surgery, lithotripsy, perioperative thromboprophylaxis, perioperative bridging therapy and coagulopathy, alone or in combination. Evidence synthesis and creation of a management protocol.

5
The rationale..... Appropriate indication for stone treatment modality Appropriate patient selection (don’t be a hero...) Risk of thrombosis Risk of bleeding
 Risk of thrombosis Risk of bleeding.")
6
Arterial thromboembolism Venous thromboembolism Mechanical heart valves (risk of arterial thrombosis (CVAs, INR < 2) High risk group (> 10%/year) Patients with mechanical heart valves, especially mitral valve or one of the older generation aortic valves (caged-ball, tilting-disk), and also patients suffering from ischemic stroke or transient ischemic attack within the last 6 months. Intermediate risk group (4-10%/year) Patients with a bileaflet aortic valve and one or more of the following: atrial fibrillation, history of ischemic stroke or transient ischemic attack, hypertension, diabetes, age >75 years and congestive heart failure. Low risk group (<4%/year) Patients with a bileaflet aortic valve with no additional co morbidities. High risk group (> 10%/year) Recent episode of DVT/PE (< 3 months), hereditary thrombophilia (Protein S or C deficiency, antithrombin deficiency, homozygotes for Factor V Leiden and G20210A prothrombin gene mutation), antiphospholipid syndrome and active cancer. Intermediate risk group (5-10%/year) Patients with history of DVT/PE between 3-12 months, heterozygotes for Factor V Leiden and prothrombin gene mutation and patients with previous malignancy. Low risk group (<5%/year) All other patients are considered in the low risk level group (<5%/year). Allocating into risk groups
 Patients with a bileaflet aortic valve and one or more of the following: atrial fibrillation, history of ischemic stroke or transient ischemic attack, hypertension, diabetes, age >75 years and congestive heart failure. Low risk group (<4%/year) Patients with a bileaflet aortic valve with no additional co morbidities. High risk group (> 10%/year) Recent episode of DVT/PE (< 3 months), hereditary thrombophilia (Protein S or C deficiency, antithrombin deficiency, homozygotes for Factor V Leiden and G20210A prothrombin gene mutation), antiphospholipid syndrome and active cancer. Intermediate risk group (5-10%/year) Patients with history of DVT/PE between 3-12 months, heterozygotes for Factor V Leiden and prothrombin gene mutation and patients with previous malignancy. Low risk group (<5%/year) All other patients are considered in the low risk level group (<5%/year). Allocating into risk groups.")
9
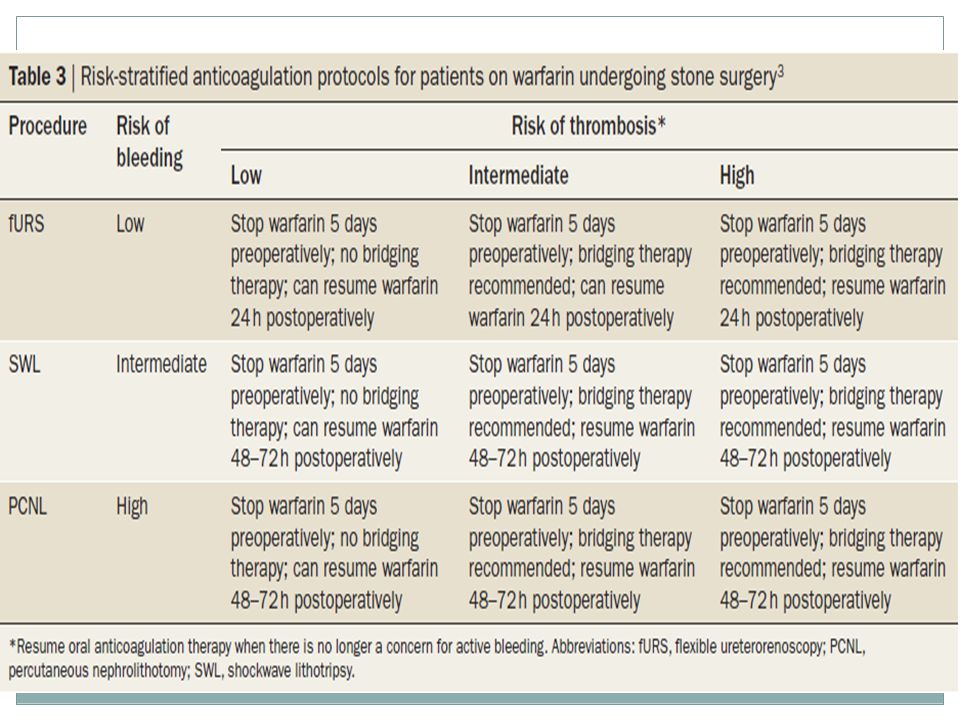
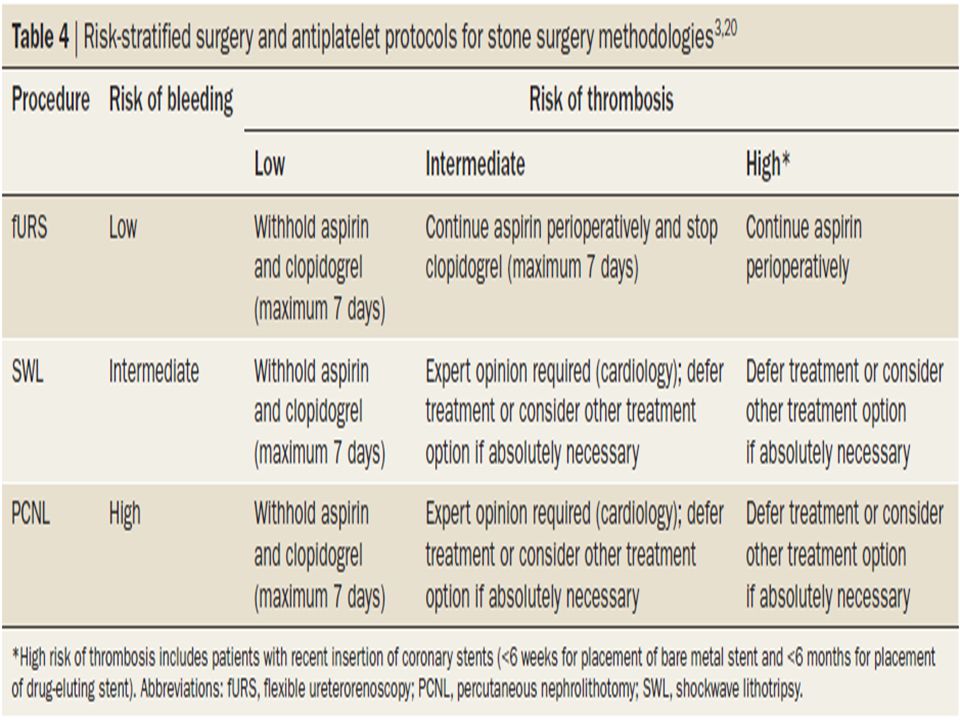
Conclusions The regulation of anticoagulation treatment and the relative risk of thromboembolic events ultimately rest with the operating surgeon in collaboration with the anesthesiology / cardiology / hematology specialists when required. Ureteroscopy is favored in anticoagulated patients, always with respect to stone size and location. Shock wave lithotripsy and PCNL is a form of stone treatment, with strict adherence to bridging protocols and patient risk factors required in most cases. Patients with cardiovascular stents constitute a unique risk group and specialist input should always be sought.

10
Questions-Discussion Thank you for your attention Douketis JD, Spyropoulos AC, Spencer FA, et al. American College of Chest Physicians. Perioperative management of antithrombotic therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 141 (2 Suppl):e326S-50S (2012). Thromboprophylaxis and bleeding diathesis in minimally invasive stone surgery. Bourdoumis A, Stasinou T, Kachrilas S, Papatsoris AG, Buchholz N, Masood J. Nat Rev Urol. 2014 Jan;11(1):51-8.
:e326S-50S (2012). Thromboprophylaxis and bleeding diathesis in minimally invasive stone surgery. Bourdoumis A, Stasinou T, Kachrilas S, Papatsoris AG, Buchholz N, Masood J. Nat Rev Urol Jan;11(1):")
11
Introduction The urologist frequently encounters patients with multiple and complex co-morbidities, who are on regular antiplatelet or anticoagulation medication or suffering from a chronic bleeding disorder. Decisions regarding peri- and post- operative thromboprophylaxis in urological surgery patients and stone surgery patients in particular are frequently met with confusion.

12
The evidence.... - for stones - increased bleeding risk during perioperative antithrombotic drug administration, probably due to urokinase release All lithotripsy options except ureteroscopy are contraindicated in the face of uncorrected bleeding tendency SWL and ureteroscopy performed as day case appear to have very low risk of thromboembolism PCNL and complicated ureteroscopy (prolonged operating time, impacted stone, large stone burden) carry an intermediate risk for thromboembolic events
 carry an intermediate risk for thromboembolic events.")
13
The evidence....- for anticoagulants - day case procedures do not usually require pharmacological thromboprophylaxis. Patients with inherent or acquired risk factors anticoagulation for 10d In low risk for thromboembolism, no bridging of anticoagulation during interruption of warfarin (LE: 2c) Aspirin may be continued up to the time of surgery instead of stopping 7 to 10 days before (LE: 2c)
 Aspirin may be continued up to the time of surgery instead of stopping 7 to 10 days before (LE: 2c).")
Similar presentations