Download presentation
Presentation is loading. Please wait.

1
Implementing the AAP SIDS Prevention Guidelines During Discharge Planning In The NICU Jennifer Sedlmeyer, BSN, RN Inova Fairfax Hospital Director of Perinatal Outreach

2
The Catalyst Two years ago, physicians discharging patients from the Inova Fairfax Hospital For Children NICU identified that infants in the NICU who had grown to term corrected gestational age (CGA) were not following the AAP’s recommendations for infant sleep. At the time of discharge parents were asking inappropriate questions such as, “Where can I purchase a gel pillow for my baby to use at home?” and “How should I prop up the head of the crib at home?”

3
The Catalyst At the same time, a baby who went home from the NICU was placed on his abdomen to sleep and died of SIDS. Mom stated “Even though the written instructions said to place the baby on his back to sleep, I placed the baby how the nurses had placed him, on his tummy”.

4
Taking Action A literature review of the current guidelines for infant sleep was conducted, focusing on premature infants nearing term GCA. Experts in the field of SIDS were contacted to discuss the AAP recommendations and how they pertain to infants born prematurely. The most current recommendations and research were compiled into a report.

5
The Task Force Staff members volunteered for a SIDS Prevention Task Force that developed NICU sleeping guidelines based on the current recommendations, personal experience, standards for supporting developmentally appropriate care, and the opinions of experts in the field. The task force also developed a parent handout to explain the transition process for preterm infants as they grow closer and closer to term CGA.

6
Results Practices in the NICU significantly improved in safety. Surveys of NICU Staff found the guidelines to be helpful and user- friendly. A survey of the NICU Parents showed an increase in knowledge and in satisfaction with care.

7
THE LITERATURE REVIEW

8
Historical Perspective “And this child died in the night; because she over laid it.” 1Kings 3:19-20 In 1291 a German poster forbid mothers from taking their infants under 3 years of age to bed with them. Late 1800’s SIDS was first defined “Sudden and Unexplained Death in Children”

9
Definition of SIDS The sudden death of an infant under 1 year of age, which remains unexplained after Thorough case investigation Complete autopsy Death scene investigation Review of the clinical history

10
Facts About SIDS SIDS is the 3 rd leading cause of death in infants under 12 months of age. 91% of SIDS deaths occur before 6 months of age. The peak is between 2-4 months of age. African American infants are nearly 2 ½ times more likely to die of SIDS than white infants.

11
Facts About SIDS SIDS is not Caused by vomiting and choking Caused by immunization Contagious The result of neglect or child abuse Hereditary Predictable or preventable

12
Which Babies Are at Greatest Risk? Infants of mothers with late/no prenatal care Infants exposed to nicotine Infants with prenatal illicit drug exposure Infants of young mothers (under 20)
.")
13
Which Babies Are at Greatest Risk? Male infants Multiples African Americans and Native Americans Infants who sleep in the prone position Infants who sleep on soft bedding Overheated infants

14
Which Babies Are at Greatest Risk? Premature infants and/or low birth weight infants (under 1000 grams) A recent study showed that premature infants were 17 times more likely to die of SIDS than term infants.
 A recent study showed that premature infants were 17 times more likely to die of SIDS than term infants..")
15
Some Theories… Researchers have identified an area of the brain that is hypoplastic or absent in SIDS babies Medullary arcuate nucleus This abnormality may put an infant at risk for sudden death during sleep This area of the brain regulates autonomic and respiratory control during sleep

16
Some Theories… The Atlas-VSC-SIDS Theory Suggests misalignment of the spine, caused by abnormal positioning in utero or by the birth process, can cause the cardiovascular and respiratory systems to malfunction, leading to sudden death during a vulnerable postnatal period.

17
Triple Risk Model 1. Critical Stage Of Development 2. Vulnerable Infant Highest risk for SIDS Highest risk at 2-4 months External risk factors such as smoking, poor sleep position, etc. Arousal response deficit or subtle brainstem dysfunction SIDS 3. Exogenous Stressors

18
The Importance of NICU Staff in Stopping SIDS A recent national study found that recommendations from the neonatal nursery staff increased the likelihood of parents following through with supine sleeping and other SIDS guidelines.

19
Behaviors That Should Be Taught To Parents To Reduce the Risk of SIDS Always place your baby on his or her back to sleep, even for naps. Place your baby on a firm mattress in a safety-approved crib or bassinet. Remove soft, fluffy bedding and stuffed toys from your baby’s sleep area. Make sure your baby’s head and face remain uncovered during sleep.

20
Behaviors That Should Be Taught To Parents To Reduce the Risk of SIDS Do not allow smoking around your baby. Do not let your baby get too warm during sleep. Talk to childcare providers, grandparents, babysitters and all caregivers about SIDS risk.

21
Always place your baby on his or her back to sleep, even for naps. The American Academy of Pediatrics has recommended since 1992 that infants be placed to sleep on their backs to reduce the risk of sudden infant death syndrome (SIDS). Infants who sleep on their backs are 3 times less likely to die from SIDS than those who sleep on their stomachs.
. Infants who sleep on their backs are 3 times less likely to die from SIDS than those who sleep on their stomachs..")
22
Always place your baby on his or her back to sleep, even for naps. Side sleeping While better than prone sleeping, it still has twice the risk of SIDS as back sleeping. Stomach sleeping Babies sleeping on their stomachs have lower blood pressure, higher heart rate and higher body temperature. Arousal may be diminished in the prone position These babies are also more likely to overheat & to rebreathe CO2.

23
The Back To Sleep Program Since 1994, when the Back To Sleep advisory was first announced, the rate of SIDS deaths in the U.S. has dropped by 50%. When babies all slept on their stomachs, there were approximately 5000-6000 deaths per year. There were just over 2,000 deaths due to SIDS in 2003.

24
What About Aspiration? According to the AAP “there is NO evidence of an increase in aspiration or increased complaints of vomiting since the incidence of supine sleeping has increased dramatically” (AAP, 2000). There is also some “direct and indirect evidence that infants who vomit are at greater risk of choking if they are sleeping face down” (AAP, 2000).
. There is also some direct and indirect evidence that infants who vomit are at greater risk of choking if they are sleeping face down (AAP, 2000)..")
25
Place your baby on a firm mattress in a safety-approved crib or bassinet Never place babies to sleep on a waterbed, sofa, or cushions. A safe crib is in good repair with a firm mattress and the slats are 2 3/8” apart (close enough so that a soda pop can cannot fit between them).
..")
26
What About Bed Sharing? NOT protective against SIDS The AAP discourages bed sharing Bed sharing does become unsafe and confers a higher risk of SIDS when… Parents smoke and bed share Parents are exhausted or under the influence of alcohol or drugs. Encourage rooming in rather than bed sharing.

27
Remove soft, fluffy bedding and stuffed toys from your baby’s sleep area. Eliminate soft bedding such as quilts or pillows from cribs. If using a blanket, use a thin one and tuck it around the mattress so it reaches only as far as the baby’s chest. Remove bumper pads from cribs. Remove wedges from cribs. Do not place stuffed animals or toys inside the sleeping area. Make certain crib sheets fit well.

28
Make sure your baby’s head and face remain uncovered during sleep. Avoid using a blanket or other coverings over your baby's face as a sun or weather screen. Do not swaddle the baby’s head. Consider using a sleep sack as an alternative to a blanket.

29
Do not let your baby get too warm during sleep. Keep the temperature in the baby's room at a level that feels comfortable. Room temperature should be about 70 degrees. Dress a baby in as much or as little as an adult would wear. Remember to remove hats and heavy outerwear when indoors during the cold weather months. Limit layers of clothes and blankets in warmer weather.

30
Do not allow smoking around your baby. Nicotine is a neuroteratogen Causes cell damage May shut off the fetal response to hypoxia May disrupt the rhythmic organization of autonomic function (Zeskind, 2000) Babies whose mothers smoke have 3X the risk of SIDS as babies born to non- smoking mothers. Exposure to other passive smokers increases the risk in a dose-dependent manner (Flemming, et. al, 2000).
 Babies whose mothers smoke have 3X the risk of SIDS as babies born to non- smoking mothers. Exposure to other passive smokers increases the risk in a dose-dependent manner (Flemming, et. al, 2000)..")
31
Talk to childcare providers, grandparents, babysitters and all caregivers about SIDS risk. About 20% of the babies that die of SIDS each year die while being cared for by someone other than their parents. Half of these children die in their first week of day care. Babies unaccustomed to sleeping on their stomachs are at significantly increased risk. Parents should tell caretakers that they want the baby to sleep on his/ her back, even at nap time.

32
Safe Sleeping Ideally this is how an infant under 1 year of age should sleep He is on a firm, flat mattress in a crib that meets safety standards. There are no quilts, pillows or toys in the crib. The baby is placed with his feet at the foot of the crib. The blanket being used is thin and it is tucked around the crib mattress, reaching only as far as the baby's chest.

33
Modeling Proper Behaviors In The NICU Research shows that parents model behaviors seen in the hospital. Stomach sleeping in the hospital = stomach sleeping at home Same is true for nesting, bundling with multiple blankets, stuffed animals in the bed and placing the head of the bed up

34
Modeling Proper Behaviors In The NICU In the study that showed premature infants were 17 times more likely to die of SIDS than term infants, much of the risk was attributed to poor behaviors learned in the nursery.

35
What do parents see in the NICU?

36
The head of the bed is up. The baby is nested with a stuffed animal and quilt in the bed. She is in the side sleeping position.

37
The baby is sleeping prone with multiple layers of soft bedding.

38
There is a covering over the baby’s face and there are multiple objects in the sleeping area.

39
The baby is nested and is in the side sleeping position with his face against the soft bedding.

40
There is a heavy, non-secured covering over the baby’s face and the head of the bed is elevated. This is a baby who never had issues with emesis or reflux.

41
This baby’s bedding is covering her mouth and nares. She had 6 blankets in the crib.

42
Learning from Our Mistakes And Taking Action

43
What We Learned Neonatal hospital staff can unwittingly be poor role models. Prone positioning, elaborate nesting and the use of soft bedding or gel pillows may be quite safe within the confines of the critical care setting but are potentially lethal at home.

44
Taking Action… Staff members were asked to volunteer for a SIDS Prevention Task Force. The multidisciplinary task force met weekly to discuss the current recommendations for preventing SIDS and how we could better incorporate them in to our NICU. The goal of the task force was that all infants would be following the AAP’s recommendations for sleep before their date of discharge.

45
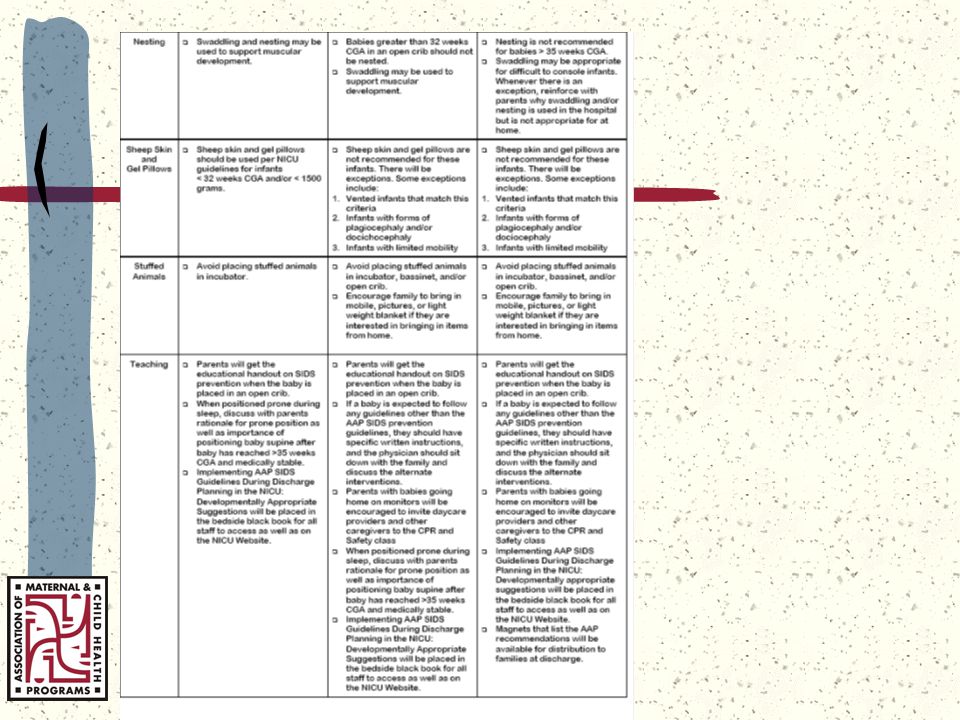
The Guidelines…

48
The Task Force The task force developed these guidelines based on the current recommendations, personal experience, standards for supporting developmentally appropriate care, and the opinions of experts in the field. The task force agreed that guidelines would be more effective than a policy, recognizing that there will always be variations from the norm in our patient population. The guidelines are divided into 3 categories: babies less than 32 weeks CGA and/or 1500 grams, and babies over 35 weeks CGA.

49
Changing Our Practice Sleep position and conditions should be adjusted to follow the AAP guidelines as soon as the baby is physiologically and developmentally ready. If a baby is expected to follow any guidelines for sleeping other than the AAP SIDS Prevention Recommendations, they should have specific written instructions and the physician should discuss the alternate interventions with the family.

50
Sharing Our Wisdom The task force also developed a parent handout to explain the transition process for preterm infants as they grow closer and closer to term CGA If a patient is getting ready to go home and staff is unable to follow the SIDS prevention guidelines, an explain of why alternate practices may be acceptable in the hospital setting but not at home is given. No more waiting until the day of discharge to review the SIDS Prevention Recommendations!

51
What We Learned There is room for both Developmentally Supportive Care and SIDS Prevention Recommendations in the NICU. We need to carefully consider each child’s changing clinical status, gestational maturity and individual readiness for supine sleeping with minimal bedding. The ultimate goal is to help high-risk babies become healthy babies

52
Remember, You Can Make A Difference! Be aware of the risk of SIDS for our vulnerable patients as they transition to home. Use your influence as healthcare professionals, through education and modeling, to minimize the risk!

53
For More Information The National Institute of Child Health and Human Development www.nichd.nih.gov, Back to Sleep SIDS Mid-Atlantic 703-933-9100 www.sidsma.org

54
For More Information American Academy of Pediatrics www.aap.org Association of SIDS and Infant Mortality Programs www.asip1.org

55
For More Information National SIDS Resource Center www.sidscenter.org SIDS Alliance www.sidsalliance.org

56
References American Academy of Pediatrics Task Force on Infant Sleep Position and Sudden Infant Death Syndrome. (2000). Changing concepts of sudden infant death syndrome: implications for infant sleeping environment and sleep position. [on-line]. Pediatrics, 105, (3), 650-656. Hudson Mohawk SIDS Affiliate. (1998). Reducing the risk of SIDS: what public health nurses need to know. Kemp, J. S. & Thach, B. T. (1995). Quantifying the potential of infant bedding to limit CO2 dispersal and factors affecting rebreathing in bedding. American Physiological Society, 740-745. Lockridge, T., Taqino, L. T., Knight, A., (1999). Back to Sleep:Is there room in that crib for both AAP recommendations and developmentally supportive care? Neonatal Network, 18 (5), 29-31.
. Changing concepts of sudden infant death syndrome: implications for infant sleeping environment and sleep position. [on-line]. Pediatrics, 105, (3), Hudson Mohawk SIDS Affiliate. (1998). Reducing the risk of SIDS: what public health nurses need to know. Kemp, J. S. & Thach, B. T. (1995). Quantifying the potential of infant bedding to limit CO2 dispersal and factors affecting rebreathing in bedding. American Physiological Society, Lockridge, T., Taqino, L. T., Knight, A., (1999). Back to Sleep:Is there room in that crib for both AAP recommendations and developmentally supportive care. Neonatal Network, 18 (5),")
57
References Moon, R., (2000). Answering medical questions about SIDS. Presented at the National SIDS Alliance Conference, Salt Lake City, Utah. Willinger, M., Ko, C. W., Hoffman, H. J., Kessler, R. C., Corwin, M. J. (2000) Factors Associated with caregivers’ choice of infant sleep position, 1994-1998. JAMA, 283 (16), 2135-2142. Zeskind, P. S., (2000). Maternal cigarette-use during pregnancy disrupts rhythmic activity in fetal autonomic regulation. Presented at the National SIDS Alliance Conference, Salt Lake City, Utah
 Factors Associated with caregivers’ choice of infant sleep position, JAMA, 283 (16), Zeskind, P. S., (2000). Maternal cigarette-use during pregnancy disrupts rhythmic activity in fetal autonomic regulation. Presented at the National SIDS Alliance Conference, Salt Lake City, Utah.")
Similar presentations