Download presentation
Presentation is loading. Please wait.

1
ECHO ASSESSMENT OF ATRIAL SEPTAL DEFECT
DR JULIAN JOHNY THOTTIAN

2
VARIOUS ECHO MODALITIES
TTE CONTRAST ECHOCARDIOGRAPHY TEE 3D ECHO ICE

3
SINUS VENOSUS-10%- superior and posterior part of septum
4 TYPES OSTIUM SECUNDUM- 66% OSTIUM PRIMUM- 15% SINUS VENOSUS-10%- superior and posterior part of septum DEFECTS NEAR CORONARY SINUS OSTIUM SECUNDUM- MIDDLE OF ATRIAL SEPTUM OSTIUM PRIMUM – LOWER PART OF ATRIAL SEPTUM

4
ASD

5
WHEN TO SUSPECT IN 2D ECHO
RIGHT VENTRICULAR DILATION ABNORMAL MOTION OF IVS- brisk anterior movement in early systole or flattened movement throughout systole ? IAS DROP OUT IN APICAL 4C VIEW RELATIVE ATRIAL INDEX

6
2D ECHO RA RV VOLUME OVERLOAD SEPTAL FLATTENING IN DIASTOLE

7
RELATIVE ATRIAL INDEX Standard apical 4C views- right atrial area divided by left atrial area ROC curve analysis - cutoff value of >0.92 predicted patients with ASDs v/s matched controls with 99.1% sensitivity and 90.5% specificity After closure, significant atrial remodeling occurred immediately, with a reduction in the mean RAI at day 1 to 0.93 ± 0.16 (P < .0001) and complete normalization at early follow-up to 0.81 ± 0.12.
 and complete normalization at early follow-up to 0.81 ±")
8
The Relative Atrial Index (RAI)—A Novel, Simple, Reliable, and Robust Transthoracic Echocardiographic Indicator of Atrial Defects Natalie A Kelly -Journal of the American Society of Echocardiography Volume 23, Issue 3 , Pages , March 2010

9
SUB COSTAL 4C VIEW To go for the subcostal 4C – Keeps the atrial septum perpendicular to the ultrasound beam Distinguishes OS , OP & SV ASDs SV ASD are consistently visualised in the SUBCOSTAL 4C VIEW Measurements of the septum can be taken Anomalous drainage of pulmonary veins Atrial septal aneurysm

10
TTE -views for ASD PSAX-IAS separates Rt &Lt atrium and runs posteriorly from NCC of aortic valve. Not seen in entirety as a result of drop out artefact APICAL 4C- Posterior aspect of Interatrial septum is clearly delineated in this view but drop out artefact is seen in region of fossa ovalis. Pulmonary venous drainage- 3 veins draining to LA APICAL 5C VIEW- Anterior aspect of interatrial septum

11
PSAX VIEW IAS AGAINST NCC OF AORTA APICAL 4C VIEW SHOWING THE IAS AND 3 VEINS DRAINING TO LA, RT LOWER PULMONARY VEIN IS USUALLY NOT SEEN

12
SUB COSTAL 4C VIEW- Useful in patients with COPD and ventilated patients
Viewed with breath held in inspiration- index marker in 3o` clock position. No IAS drop outs SUB COSTAL SHORT AXIS- Index marker at 12o`clock position and sweeping the transducer from midline to Rt side of patient

13
SUBCOSTAL 4C VIEW SUB COSTAL SHORT AXIS VIEW ALSO SHOWS IVC DRAINING TO RA AND EUSTACHIAN VALVE

14
Other important views To visualise SVC- Suprasternal short axis –index marker in 4 o`clock position L-SVC is seen from lt supraclvicular fossa or suprasternal short axis Suprasternal short axis to visualise the the pulmonary veins draining into left atrium Cleft mitral valve in AVCD in 12o`clock position in PSAX

15
SUPRASTERNAL SHORT AXIS

16
`Crab view` showing absent Rt upper and Rt lower pulmonary vein

17
En face view in 2D First the apical 4c view was taken The image index marker was at approximately kept at 1 o'clock Keeping the atrial septum and ASD in the region of interest, the transducer was rotated counterclockwise approximately 45° to 60° Xinseng et al Journal of the American Society of Echocardiography Volume 23, Issue 7 , Pages , July 2010

18
A-4c view & B-En face view

19
Ostium primum ASD Defect in lower part of IAS
Associated sometimes with inlet VSD Cleft mitral valve AV Valve regurgitation Partial attachment of mitral valve to IVS

20
Primum ASD Fig 5 Apical four chamber view demonstrating
LV RV RA LA Apical four chamber view demonstrating a primum atrial septal defect Colour Doppler flow image from same view illustrating left-to-right shunt across the primum atrial septal defect

21
CLEFT MITRAL VALVE IN PSAX VIEW
POSTERIORLY DIRECTED JET OF MR

22
Ostium Secundum ASD 10 morphological variations of defects MC- Deficient aortic rim (42.1%) Central defects (24.2%) Deficient Inferoposterior rim (12.1%) Perforated aneurysm of the septum (7.9%) Multiple defects (7.3%) Combined deficiency of mitral and aortic rims (4.1%), Deficient SVC rim (1%), Deficient coronary sinus rim (1%) Podnar T, Martanovic P, Gavora P,Masura J. Morphological variations of secundum-type atrial septal defects: feasibility for percutaneous closure using Amplatzer septal occluders. Catheter Cardiovasc Interv 2001;53:386 –91.
. Central defects (24.2%) Deficient Inferoposterior rim (12.1%) Perforated aneurysm of the septum (7.9%) Multiple defects (7.3%) Combined deficiency of mitral and aortic rims (4.1%), Deficient SVC rim (1%), Deficient coronary sinus rim (1%). Podnar T, Martanovic P, Gavora P,Masura J. Morphological variations of secundum-type atrial septal defects: feasibility for percutaneous closure using Amplatzer septal occluders. Catheter Cardiovasc Interv 2001;53:386 –91.")
23
Centrally located ASD imaged at 0°

24
ASD with deficient Aortic margin

25
Large ASD with deficient posterior and Aortic margins

26
Multiple ASDs; larger anterior defect (block arrow) and a smaller posterior defect
 and a smaller posterior defect")
27
Sinus venosus ASD A – INTACT IAS B- COLOUR DOPPLER SHOWS DEFECT IN THE
UPPER PART OF IAS AT ENTRANCE OF SVC TEE

29
CORONARY SINUS ASD DILATED CORONARY SINUS TEE 120 DEGREES

30
ATRIAL SEPTAL ANEURYSM
CRITERIA A-PROTRUSION OF ANEURYSM ATLEAST 15MM OF PLANE OF IAS OR IAS SHOWING 15MM OF PHASIC EXCURSION DURING CARDIORESPIRATORY CYCLE B- BASE WIDTH≥ 15MM

31
PATENT FORAMEN OVALE TEE -0 DEGREE TEE-90 DEGREES

32
PFO WITH SECONDARY SEPTUM

33
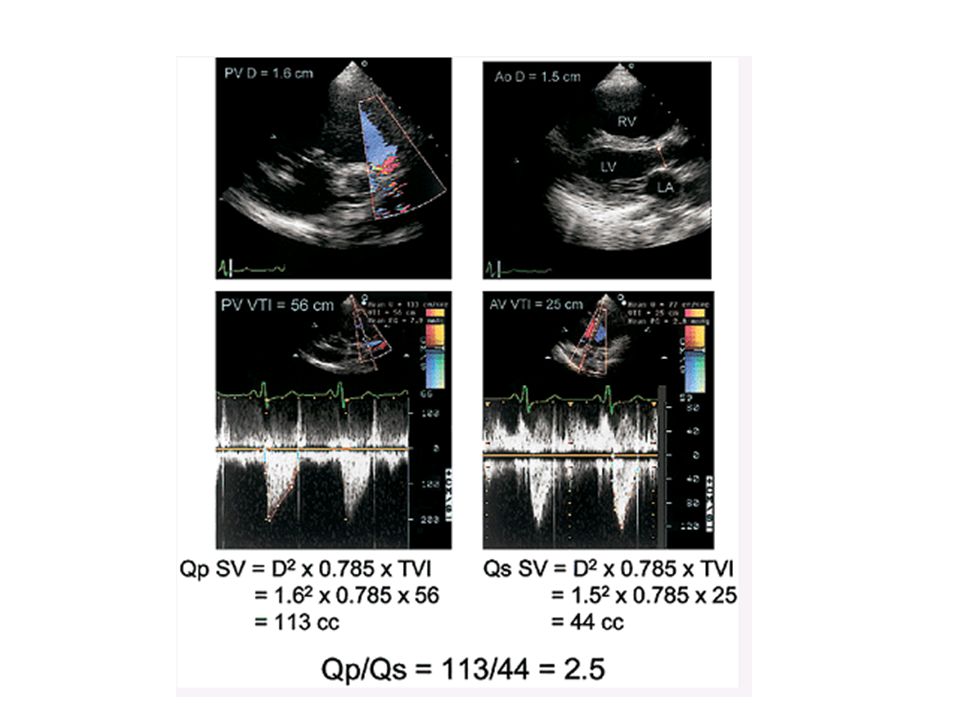
COLOUR DOPPLER Shows the direction of the shunt
Caveat- FP results due to improper gain and caval flow streaming near septum can be misdiagnosed as ASD. PULSED DOPPLER- demonstrates the flow from L to R in mid systole to mid diastole with second phase in atrial systole. Some R to L shunting occurs in early systole QUANTIFICATION OF SHUNT – Qp /Qs

34
OS ASD VIA DOPPLER SINUS VENOSUS ASD VIA DOPPLER

36
CONTRAST ECHOCARDIOGRAPHY
APICAL 4C VIEW IS USED AGITATED SALINE USED- 5ml in each 10ml syringe, 0.5ml of air taken in the syringe and agitated to create microbubbles.

37
ARROW SHOWS NEGATIVE CONTRAST
EFFECT DIRECT EVIDENCE OF SHUNT- NON CONTRAST BLOOD IN RA Extent of shunting tend to focus on numbers of bubbles seen in a single still frame in the left atrium. Shunt grading incorporates : Grade 1: 5 bubbles; Grade 2: 5 to 25 bubbles; Grade 3:25 bubbles; Grade 4: Opacification of chamber Echocardiographic Evaluation of Patent Foramen Ovale Prior to Device Closure Bushra et al JACC 2010 VOL. 3, NO. 7, 2010

39
RIMS OF ASD Aortic - Superoanterior Atrioventricular (AV) valve -mitral or inferoanterior Superior Vena Caval SVC – Superoposterior Inferior venacaval (IVC or Inferoposterior) Posterior (from the posterior free wall of the atria).
 valve -mitral or inferoanterior Superior Vena Caval SVC – Superoposterior Inferior venacaval (IVC or Inferoposterior) Posterior (from the posterior free wall of the atria).")
40
IVC AND SVC RIMS

41
OTHER RIMS TTE TEE

42
TEE 2D & 3D

43
2D TEE at 0o

44
TEE at 0° to Evaluate the Posterior and Anterior Rims of the Defect- SVC RAA level

45
TEE at 0° to Evaluate the Posterior and Anterior Rims of the Defect- mid septum level

46
TEE at 0° to Evaluate the Posterior and Anterior Rims of the Defect- At the level of the AV valves atrioventricular valves

47
TEE at 90° to Evaluate the SVC and IVC Rims
AORTIC RIM IS SEEN IN TEE 45 DEGREES

48
Probe to 30-40o right

49
Probe rotated 30-40o left

50
Special tee views for Inferoposterior rims
No Infero posterior rim with probe in normal position

51
Catheter Closure of Atrial Septal Defects With Deficient IVC Rim Under TEE Guidance K.S. Remadevi, MD, FNB, Edwin Francis, DM, and Raman Krishna Kumar, DM, FACC . Catheterization and Cardiovascular Interventions (2008) Retroflexed probe in the stomach and bought towards the esophagus and viewed In the 70-90o view

52
STOP FLOW METHOD –DEVICE SIZING

53
DEVICE SELECTION

54
TEE IMAGES OF ASD DEVICE CLOSURE

55
3D ECHO Matrix transducers – pyramid shaped volumes
Full volume 3D dataset in 4-7 cardiac cycles Ideal window is the mid esophageal basal long axis (bicaval view) Subcostal 4c view- enface septum Low parasternal 4c view case of suboptimal windows 3D tee overcomes 3D TTE if suboptimal windows
 Subcostal 4c view- enface septum. Low parasternal 4c view case of suboptimal windows. 3D tee overcomes 3D TTE if suboptimal windows.")
56
Real-time 3D imaging demonstrates the changing shape of the ASD during a cardiac cycle, with maximum size in diastole As we take the Bicaval view structures – we first remove the right atrial free wall . Images are taken with suspended respiration and ECG gating with optimal gain settings Low gain – drop outs and high gain – blurring of structural details

57
Gain settings For Best view Cropping to Get the IAS

58
TUPLE (TILT UP & LEFT)-ENFACE VIEW OF IAS FROM LT ATRIAL PERSPECTIVE
-ENFACE VIEW OF IAS FROM LT ATRIAL PERSPECTIVE")
59
RIMS OF ASD ASD IN VARIOUS PHASES OF CARDIAC CYCLE

60
ATRIAL SEPTUM ANEURYSM
WITH ASD MULTIPLE ASDs

61
DEFECT NEAR THE IVC

62
3D echo- En face 3D reconstruction of a secundum ASD with a relatively deficient IVC and posterior rim

63
multiple ASDs with the thin atrial septum (*) separating the 2 defects
 separating the 2 defects")
64
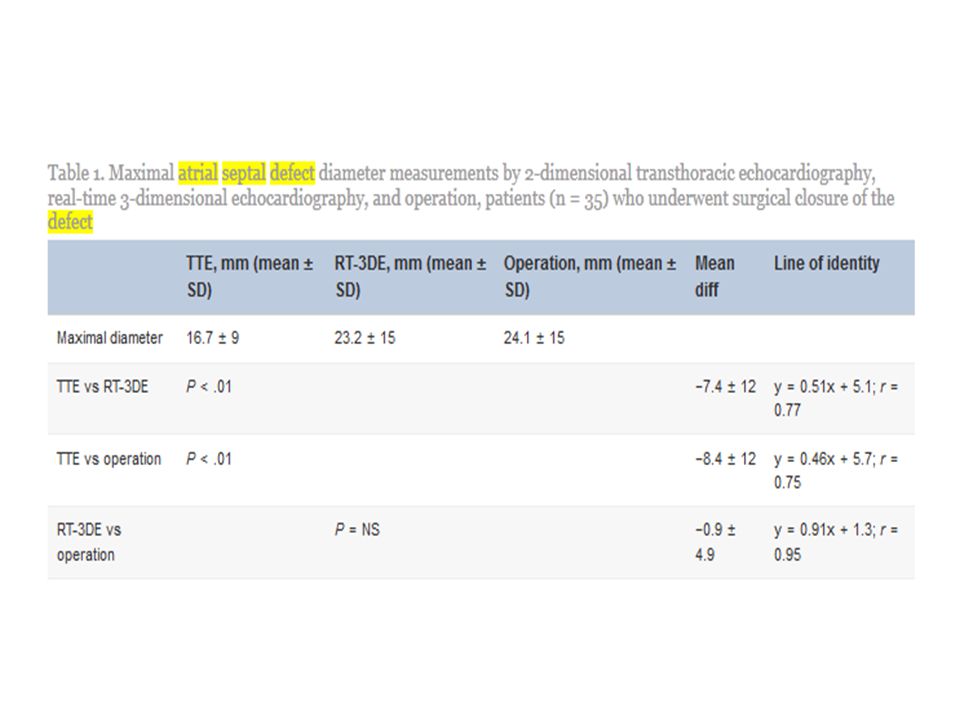
Measuring the ASD Images Paediatr Cardiol. 2011 Jul-Sep; 13(3): 1–18.
Three-dimensional trans-esophageal Echocardiographic Evaluation of Atrial Septal Defects: A Pictorial Essay Vinay K Sharma, S Radhakrishnan, and S Shrivastava

65
Deployment of ASD device

66
INTRACARDIAC ECHO(ICE)
9-10MHz frequency TWO TYPES- ROTATING AND PHASED ARRAY ROTATING TYPE -9F ,9MHz PHASED ARRAY MHz ROTATING – 360o ALONG THE TRANSVERSE PLANE & DEPTH OF IMAGING 5CM PHASED ARRAY MHz, SECTOR OF 90o DEPTH OF IMAGING 12CM SHEATH SIZE 8F,9F,10F

67
IAS between RA & LA Long axis view
Tenting of IAS (long arrow) by needle (short arrow) approaching it from right atrium (RA)
 by needle (short arrow) approaching it from right atrium (RA)")
68
Measurement of ASD size along long axis
Balloon stretched diameter

69
ADVANTAGES Assess ASD size and rims Pulmonary veins assessment
Position of sheath and guide wire can be determined. Additional defects can also be assessed Plan for closure

70
POST PROCEDURE COMPLICATIONS
RESIDUAL SHUNT POST PROCEDURE

71
DEVICE MISPLACEMENT

72
IMPINGEMENT OF THE DEVICE ON AORTIC ANNULUS- CAN LEAD TO EROSION?
CONCEPT OF `MINNESOTA WIGGLE`

73
DEVICE DISLODGEMENT AND ATTEMPETED SNARING

76
The correlations between the ASD maximal diameter by RT-3DE and operation or balloon sizing were excellent (r > 0.95). All surrounding rims of the atrial septum could be assessed on 3D reconstruction; except for the aortic rim, a cross-sectional reconstruction was created mimicking the transesophageal echocardiographic cross section (r > 0.92)
.")
77
THANK YOU

78
MCQ

79
QUESTION 1 To view the IVC rim better we need to keep the TEE probe in
Neutral position in mid esophagus Anteflexed position in mid esophagus Retroflexed position in stomach Neutral position in high esophagus

80
QUESTION 2 Cleft mitral valve is seen in
PSAX with index marker at 12 o` clock position PSAX with index marker at 4 o` clock position Subcostal short axis at 12 o` clock position Subcostal short axis at 12 o`clock position

81
QUESTION 3 Enface view of ASD in 2D echo is seen in Apical 4c view
Parasternal short axis view Subcostal short axis Right parasternal view

82
QUESTION 4 Most common type of ostium secundum ASD
Deficient aortic rim Central defect Deficient posterosuperior rim Combined deficient mitral and aortic rim

83
QUESTION 5 ATRIAL SEPTAL ANEURYSM- FALSE IS
a) Protrusion of aneurysm at least 15mm b) IAS showing 15mm of phasic excursion during cardiorespiratory cycle C) Base WIDTH≥ 15MM D) RA/ RV overload should always be demonstrated
 Protrusion of aneurysm at least 15mm. b) IAS showing 15mm of phasic excursion during cardiorespiratory cycle. C) Base WIDTH≥ 15MM. D) RA/ RV overload should always be demonstrated.")
84
QUESTION 6 IVC rim and SVC rim is evaluated in (TEE) mid esophageal
 mid esophageal")
85
QUESTION 7 Posterior and anterior rims are assessed in (TEE) 0o 50o
 0o 50o")
86
QUESTION 8 Relative atrial index - A cutoff value of predicted patients with ASDs v/s matched controls with 99.1% sensitivity and 90.5% specificity 0.78 0.92 0.62 0.52

87
QUESTION 9 Maximum diameter of ASD is in Early systole Late systole
Early diastole Late diastole

88
QUESTION 10 Aortic rim In TEE is seen in Mid esophageal 0o
Gastroesophageal jn retroflexed

Similar presentations









 FOR MITRIAL REGURGITATION>")






 Transducer position: left sternal edge; 2 nd – 4 th intercostal space Marker dot direction: points towards left shoulder(90.>")





