Download presentation
Presentation is loading. Please wait.

1
ACUTE PULMONARY EMBOLISM Part I Etiology,Clinical features,Diagnosis Dr Vinod G V

2
PE and DVT are two clinical presentations of venous thromboembolism (VTE) and share the same predisposing factors. Most cases of PE occurs as a consequence of DVT Acute case fatality rate for PE ranges from 7 to 11%

3
N=94194; 6 yr follow up. The incidence rate for All first VT events was 1.43 per 1000 person-years [95% confidence interval (CI): 1.33–1.54] Deep-vein thrombosis (DVT) was 0.93 per 1000 person-years (95% CI: 0.85–1.02) Pulmonary embolism (PE) was 0.50 per 1000 person-years (95%CI: 0.44–0.56). J Thromb Haemost 2007; 5: 692–9.
: 1.33–1.54] Deep-vein thrombosis (DVT) was 0.93 per 1000 person-years (95% CI: 0.85–1.02) Pulmonary embolism (PE) was 0.50 per 1000 person-years (95%CI: 0.44–0.56). J Thromb Haemost 2007; 5: 692–9..")
4
Acquired factors Reduced mobility Advanced age Cancer Acute medical illness Major surgery Trauma Spinal cord injury Pregnancy and postpartum period Polycythemia vera Antiphospholipid antibody syndrome Oral contraceptives Hormone-replacement therapy Heparins Chemotherapy Obesity Central venous catheterization Immobilizer or cast

5
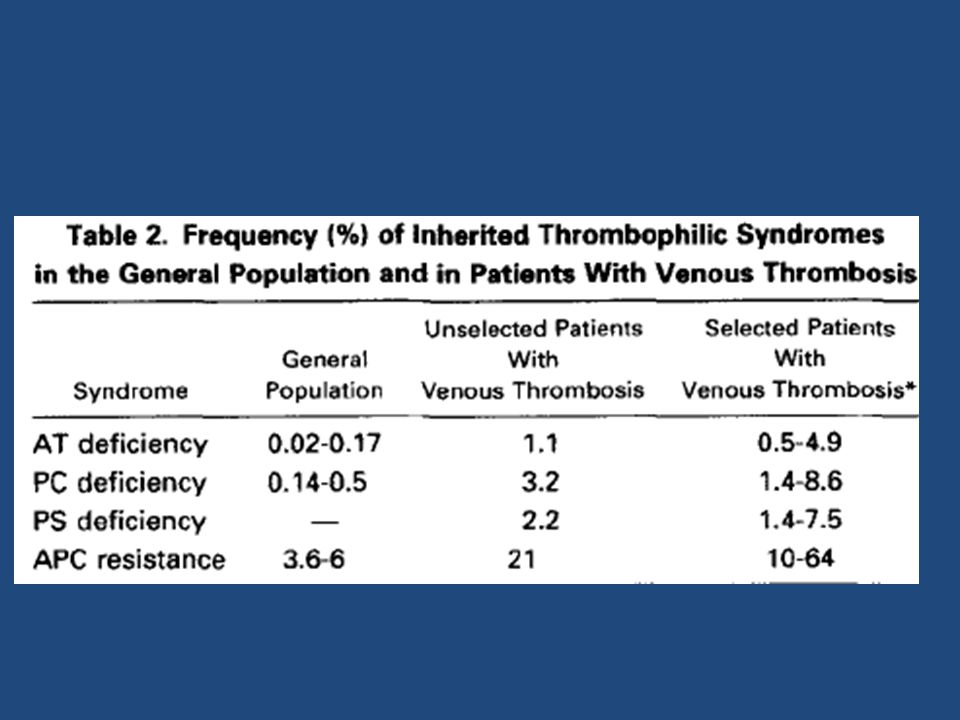
Hypercoagulable states Factor V Leiden resulting in activated protein C resistance Prothrombin gene mutation Antithrombin deficiency Protein C deficiency Protein S deficiency

7
First thrombosis usually at young age (<40 yr) Frequent recurrences Family history of VTE
 Frequent recurrences Family history of VTE")
8
Pathophysiology

9
Clinical features Symptoms unexplained dyspnea Chest pain, either pleuritic or “atypical” Cough Haemoptysis Signs Tachypnea Tachycardia Low-grade fever Left parasternal lift Tricuspid regurgitant murmur Accentuated P2 Hypotension

10
Clinical classification Massive PE: Systolic blood pressure <90 mm Hg Poor tissue perfusion or Multisystem organ failure plus Right or left main pulmonary artery thrombus or “high clot burden” Submassive PE: Hemodynamically stable but moderate or severe right ventricular dysfunction or enlargement Small to moderate PE: Normal hemodynamics and normal right ventricular size and function

11
Classic Well’s criteria SCORE POINTS DVT symptoms or signs -3 An alternative diagnosis is less likely than PE -3 Heart rate >100/min -1.5 Immobilization or surgery within 4 weeks -1.5 Prior DVT or PE -1.5 Hemoptysis -1 Cancer treated within 6 months or metastatic -1 >4 score points = high probability ≤4 score points = non–high probability

13
ECG Sinus tachycardia Incomplete or complete right bundle branch block Right-axis deviation T wave inversions in leads III and aVF or in leads V1-V4 S wave in lead I and a Q wave and T wave inversion in lead III (S1Q3T3) Atrial fibrillation or atrial flutter
 Atrial fibrillation or atrial flutter")
14
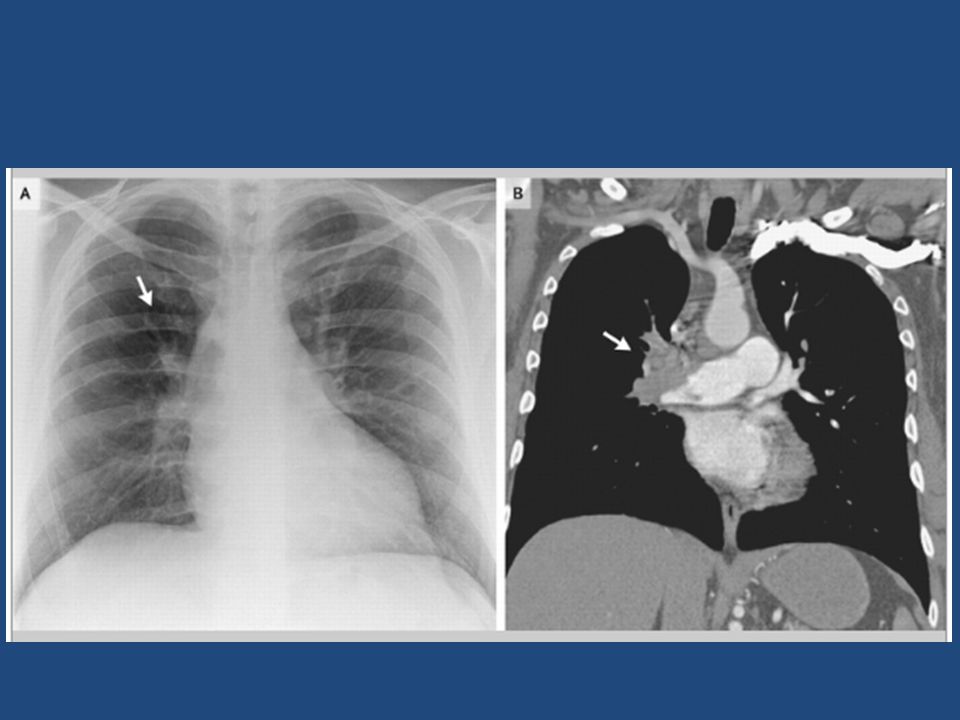
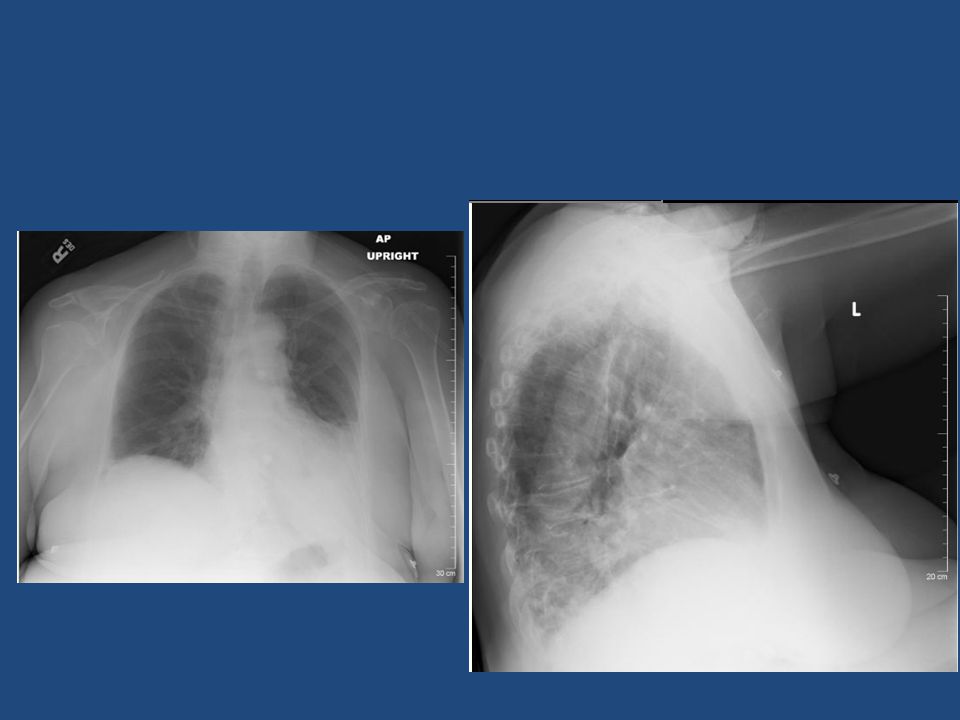
CHEST X RAY Major chest radiographic abnormalities are uncommon. A near-normal radiograph in the setting of severe respiratory compromise is highly suggestive of massive PE. Focal oligemia (Westermark sign) indicates massive central embolic occlusion. A peripheral wedge-shaped density above the diaphragm (Hampton hump) usually indicates pulmonary infarction. Enlargement of the descending right pulmonary artery. The vessel often tapers rapidly after the enlarged portion
 indicates massive central embolic occlusion. A peripheral wedge-shaped density above the diaphragm (Hampton hump) usually indicates pulmonary infarction. Enlargement of the descending right pulmonary artery. The vessel often tapers rapidly after the enlarged portion.")
17
ECHO Right ventricular enlargement or hypokinesis, especially free wall hypokinesis, with sparing of the apex (the McConnell sign) Interventricular septal flattening and paradoxical motion toward the left ventricle, resulting in a D-shaped left ventricle in cross section Tricuspid regurgitation Pulmonary hypertension with a tricuspid regurgitant jet velocity >2.6 m/sec Loss of respiratory-phasic collapse of the inferior vena cava with inspiration Dilated inferior vena cava without physiologic inspiratory collapse Direct visualization of thrombus (more likely with transesophageal echocardiography)
 Interventricular septal flattening and paradoxical motion toward the left ventricle, resulting in a D-shaped left ventricle in cross section Tricuspid regurgitation Pulmonary hypertension with a tricuspid regurgitant jet velocity >2.6 m/sec Loss of respiratory-phasic collapse of the inferior vena cava with inspiration Dilated inferior vena cava without physiologic inspiratory collapse Direct visualization of thrombus (more likely with transesophageal echocardiography)")
19
Computed Tomography Most commom investigation performed SDCT or MDCT MDCT more sensitive for subsegmental level thrombi CT can rule out other causes

22
CT Two clinical studies reported a sensitivity around 70% and a specificity of 90% for single-detector CT (SDCT). Negative SDCT and the absence of a proximal DVT on lower limb venous ultrasonography in non- high clinical probability patients was associated with a 3-month thromboembolic risk of approximately 1%

23
For MDCT a sensitivity of 83% and a specificity of 96%. In patients with a low or intermediate clinical probability of PE as assessed by the Wells score, a negative CT had a high NPV for PE (96 and 89%respectively) and only 60% in those with a high pretest probability. The PPV of a positive CT was high (92–96%) in patients with an intermediate or high clinical probability but much lower (58%) in patients with a low pretest likelihood of PE
 and only 60% in those with a high pretest probability. The PPV of a positive CT was high (92–96%) in patients with an intermediate or high clinical probability but much lower (58%) in patients with a low pretest likelihood of PE.")
24
D-Dimer Assay Endogenous fibrinolysis More sensitive but less specific Negative predictive value Not very useful in hospitalized patients since values may be elevated due to comorbid illness

25
D-dimer ELISA is an excellent screening test for suspected PE A negative D-Dimer assay in low clinical probability case rules out PE D-dimer ELISA was often elevated in the absence of PE like sepsis,cancer,acute medical illness Low specificity and poor positive predictive value

26
Trop I Elevated levels indicates RV dialatation or RV dysfunction Helps to identify patients with massive pulmonary embolism Has prognostic value

28
Pulmonary Angiography Invasive procedure Considered previously as gold standard Now rarely performed as a diagnostic procedure Direct evidence of thrombus seen as filling defect or amputation of an arterial branch.

30
Lung V/Q Scan Not performed routinely In patients with elevated D Dimer and contraindication for CT contrast allergy;renal failure Shows multiple perfusion defects in massive pulmonary embolism

31
Venous Ultrasonography Evidence of DVT in lower limbs Loss of vein compressibility 50% of patients with PE has no evidence of DVT

33
SUMMARY High clinical suspicion is needed for diagnosis No symptoms, signs or test is highly specific for PE Assess pretest clinical probability before applying diagnostic test Integrated diagnostic approach is needed

34
.Most common cause of inherited thrombophilia A.Factor V Leiden B.Prothrombin gene mutation C.protein c defficiency D.protein s defficiency

35
2. Most common ECG finding seen in patients with acue pulmonary embolism A.Sinus tachycardia B.S1Q3T3 C.T inversion in precordial leads D.RBBB

36
Well’s score includes all except A.Cancer treated within 6 months B.Haemoptysis C.Surgery within 4 wks D.Dyspnoea

37
D Dimer assay in acute pulmonary embolism ;wrong statement A.specificity is low B.High NPV in low probability cases C.Values >500ng/ml diagnostic of PE D.Most useful in emergency department than in hospitalised patients

38
Most common symptom in PE A.Pleuritic chest pain B.Haemoptysis C.Sudden onset dyspnoea D.Syncope

39
Most common clinical sign in PE A.Tachypnoea B.RV S3 C.Elevated JVP D.Pleural rub

40
False statement about ECHO IN PE A.Mc connell’s sign most sensitive sign B.RV dilatation indicates poor prognosis C.D shaped LV D.TEE more sensitve for demonstrating thrombus

Similar presentations




















 F.R.C.P. (E) F.R.C.P. (LONDON) F.A.C.C DESIGNED AT A.V. DEPT F.J.M.C.>")





