Download presentation
Presentation is loading. Please wait.

1
DCIS – Are we cutting it? Dr Alex Lemaigre With thanks to:
Mr Richard Boulton Dr Elizabeth Osinibi Mr Oladapo Fafemi

2
Introduction to DCIS Ductal carcinoma in situ
Non invasive neoplasm in the milk ducts of the breast Predisposes to invasive ductal carcinoma 2900 cases of screen-detected DCIS per annum (9)
")
3
DCIS - Treatment Usually wide local excision (lumpectomy) +- radiotherapy. Prognosis improved by greater resection margin, and the use of radiotherapy.(1,2,3) Sentinel node biopsy (SNLB) not recommended (incidence LN metastases <1%). (4,5)
 Sentinel node biopsy (SNLB) not recommended (incidence LN metastases <1%). (4,5)")
4
Aims and Objectives To discover how many of DCIS cases on core biopsy will be found to have invasive cancer on excision histology. Can we predict which these will be? Should we be doing SNLB on these patients? How successful are we at adequately excising the neoplasm with wide local excision?

5
Methods Analysed all new patients diagnosed with DCIS only on core biopsy in 2009, 2010 and 2011. grade of initial DCIS diagnosis on excision specimen closest resection margin need for re-excision

6
Inclusion criteria: all patients newly diagnosed with DCIS ONLY on core biopsy in 2009, 2010 or 2011, regardless of age, sex, or method of detection. Exclusion criteria: Recurrent breast cancer, DCIS + any other diagnosis on core biopsy. Where multiple grades of DCIS were present in a specimen, the highest grade was considered.

7
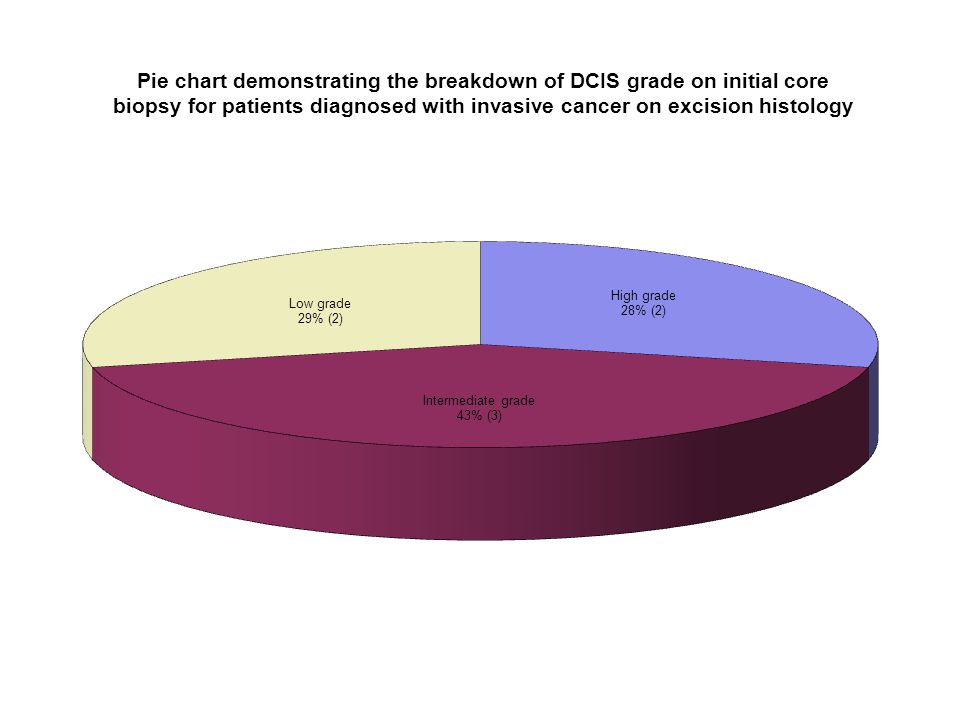
Results Total 36 patients with DCIS only in 3 years

12
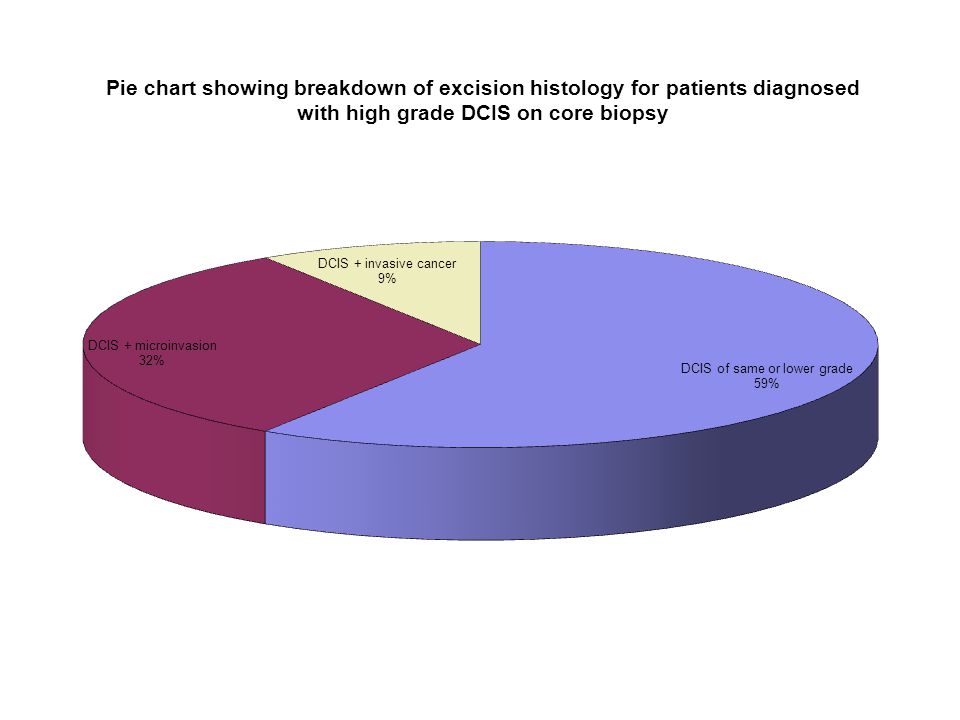
Conclusions 19% of patients with DCIS only on core biopsy were found to have invasive ductal carcinoma on excision histology. These patients cannot be predicted by the initial grade of the DCIS. High grade DCIS does not increase the risk of invasive cancer compared to lower grades.

13
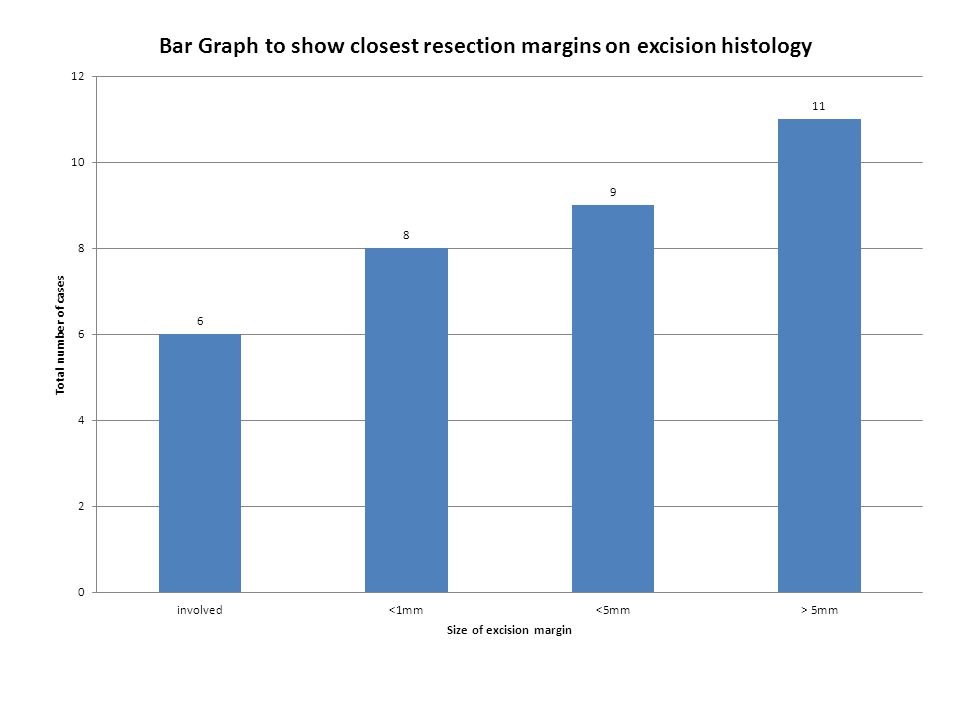
Resection Margins Analysed the resection margins on excision specimens. 1 case was excluded as the patient had a mastectomy for multifocal DCIS 1 case was excluded as the biopsy appeared to have entirely excised the DCIS Total = 34 patients

14
North Middlesex standard “safe” excision margin for DCIS = 5mm
There is some variability between centres on this figure (1mm – 10mm).
.")
16
NB – total number here = 45 as many specimens had >1 margin reported as close

17
Need for Re-excision? According to these data 11 out of 34 cases had wide enough resection margins. Therefore 23/34 (67%) require re-excision to improve margins. However – improving the posterior margin involves resecting the chest wall (including pectoralis major). There is no prognostic benefit to this, and it causes greater morbidity. Excluded those where the posterior margin was the only close margin <5mm (n=3)
 require re-excision to improve margins. However – improving the posterior margin involves resecting the chest wall (including pectoralis major). There is no prognostic benefit to this, and it causes greater morbidity. Excluded those where the posterior margin was the only close margin <5mm (n=3)")
19
The Saga Continues... 20 cases still require re-excision
= 55% of our original population of 36 patients 2 had a mastectomy 1 was referred to Royal Free 2 lost to NMUH follow-up 11 had successful re-excision 4 had inadequate re-excision Inadequate – residual DCIS / residual multifocal

20
Conclusions 55% of DCIS patients required more than one operation to adequately clear the DCIS

21
Discussion – Excision histology + SLNB
SLNB used in invasive cancer to determine lymph node spread. SLNB cannot be performed after WLE due to disruption of lymphatic drainage. DCIS grade does not predict probability of invasive carcinoma. Therefore cannot guide us which patients to select for SLNB. No value in SLNB on DCIS patients as <1% will show LN involvement (4,5). I.E. Our results agree with the current thinking that there is no value in SLNB with DCIS patients.
. I.E. Our results agree with the current thinking that there is no value in SLNB with DCIS patients.")
22
Ductal carcinoma in situ
1.4.5 Do not perform SLNB routinely in patients with a preoperative diagnosis of DCIS who are having breast conserving surgery, unless they are considered to be at a high risk of invasive disease. 1.4.6 Offer SLNB to all patients who are having a mastectomy for DCIS.

23
Discussion – Excision Margins
Surgery for DCIS aims to balance disease clearance (and risk of recurrence) and an acceptable cosmetic appearance. No prospective trials have assessed optimum excision width for in situ disease. Involved margins carry the worst prognosis (6) No consensus on standard acceptable margins How do we decide? Chan et al <1mm bad, >1mm good Dunne et al >2mm good (with radiotherapy) Wong et al >10mm + still experienced a high rate of recurrence.
 and an acceptable cosmetic appearance. No prospective trials have assessed optimum excision width for in situ disease. Involved margins carry the worst prognosis (6) No consensus on standard acceptable margins. How do we decide Chan et al <1mm bad, >1mm good. Dunne et al >2mm good (with radiotherapy) Wong et al >10mm + still experienced a high rate of recurrence.")
24
1.3 Surgery to the breast Ductal carcinoma in situ 1.3.1 For all patients treated with breast conserving surgery for DCIS a minimum of 2 mm radial margin of excision is recommended with pathological examination to NHSBSP reporting standards. Re-excision should be considered if the margin is less than 2 mm, after discussion of the risks and benefits with the patient. 1.3.2 Enter patients with screen-detected DCIS into the Sloane Project (UK DCIS audit)[5]. 1.3.3 All breast units should audit their recurrence rates after treatment for DCIS.
[5] All breast units should audit their recurrence rates after treatment for DCIS.")
25
Discussion – Re-excision rates
55% re-excision seems very high. Wong et al stated a re-excision rate of 84% to achieve margins of >10mm. (7) Holland et al stated a re-excision rate of 43% to achieve margins of >1mm. (8) Re-excision rates will depend on what distance the excision margin is considered safe.
 Holland et al stated a re-excision rate of 43% to achieve margins of >1mm. (8) Re-excision rates will depend on what distance the excision margin is considered safe.")
26
Discussion - Radiotherapy
Post-operative radiotherapy significantly decreases risk of disease recurrence (1,2,3). Julien et al 2000: 4 year recurrence free = 84% vs 91% if treated with radiotherapy (1) Chan et al 2001: Recurrence of 18.6% vs 11.1% if treated with radiotherapy (3) Wong et al 2006: abandoned trial of WLE only (10mm margin) due to high recurrence rate of 2.4% per patient year. (7) NMUH does not routinely offer radiotherapy to DCIS patients Radiotherapy offered for chest wall if posterior margin not clear.
. Julien et al 2000: 4 year recurrence free = 84% vs 91% if treated with radiotherapy (1) Chan et al 2001: Recurrence of 18.6% vs 11.1% if treated with radiotherapy (3) Wong et al 2006: abandoned trial of WLE only (10mm margin) due to high recurrence rate of 2.4% per patient year. (7) NMUH does not routinely offer radiotherapy to DCIS patients. Radiotherapy offered for chest wall if posterior margin not clear.")
27
1.11 Radiotherapy Radiotherapy after breast conserving surgery Patients with early invasive breast cancer who have had breast conserving surgery with clear margins should have breast radiotherapy. Offer adjuvant radiotherapy to patients with DCIS following adequate breast conserving surgery and discuss with them the potential benefits and risks (see recommendation in section 1.3.1)
")
28
Further Work Audit recurrence rates in these patients.
Compare our results with rates of re-excision data from other centres with similar choice of acceptable margins. Compare our data with previous data collected by Mr Fafemi some years ago.

29
Re-assess the treatment we offer for DCIS

30
References Julien J, Bijker et al. Radiotherapy in breast conserving treatment for ductal carcinoma in situ: first results of EORTC randomized phase III trial Lancet 2000; 355: Fisher ER, Dignam J et al. Pathologic findings from the National Surgical Adjucant Breast Project (NSABP) eight-year update of Protocol B-17 intraductal carcinoma. Cancer 1999;86:429-38 Chan KC, Knox WF et al. Extent of excision margin width required in breast conserving surgery for ductal carcinoma in situ. Cancer 2001;91:9-16 Kitchen PR, Cawson JN et al. Axillary dissection and ductal carcinoma in situ of the breast: a change in practice. Aust NZ J Surg 2000;70:419-22 Veronesi P, Intra M et al. Is sentinel node biopsy necessary in conservatively treated DCIS? Ann Surg Oncol 2007;14(8):2202-8 Law, Tsz Ting MBBS; Kwong, Ava FRCS. Surgical Margins in Breast Conservation Therapy: How Much Should We Excise? Southern Medical Journal: December Volume Issue 12 - pp Wong J, Kaelin CM et al. Prospective study of wide local excision alone for ductal carcinoma in situ of the breast. J clin oncol 2008;24(7): Holland PA, Gandi A, et al. The importance of complete excision in the prevention of local recurrence of ductal carcinoma in situ. Br J Cancer 1998; 77(1): Dodwell D, Clements K, Lawrence G, Kearins O, Thomson C, Dewar J, Bishop H, on behalf of the Sloane Project Steering Group. Radiotherapy following breast-conserving surgery for screen-detected ductal carcinoma in situ: indications and utilisation in the UK. Interim findings from the Sloane Project. British Journal of Cancer 2007; 97: NICE guidelines – Feb 2009 – Early and locally advanced breast cancer, diagnosis and treatement.
 eight-year update of Protocol B-17 intraductal carcinoma. Cancer 1999;86: Chan KC, Knox WF et al. Extent of excision margin width required in breast conserving surgery for ductal carcinoma in situ. Cancer 2001;91:9-16. Kitchen PR, Cawson JN et al. Axillary dissection and ductal carcinoma in situ of the breast: a change in practice. Aust NZ J Surg 2000;70: Veronesi P, Intra M et al. Is sentinel node biopsy necessary in conservatively treated DCIS Ann Surg Oncol 2007;14(8): Law, Tsz Ting MBBS; Kwong, Ava FRCS. Surgical Margins in Breast Conservation Therapy: How Much Should We Excise Southern Medical Journal: December Volume Issue 12 - pp Wong J, Kaelin CM et al. Prospective study of wide local excision alone for ductal carcinoma in situ of the breast. J clin oncol 2008;24(7): Holland PA, Gandi A, et al. The importance of complete excision in the prevention of local recurrence of ductal carcinoma in situ. Br J Cancer 1998; 77(1): Dodwell D, Clements K, Lawrence G, Kearins O, Thomson C, Dewar J, Bishop H, on behalf of the Sloane Project Steering Group. Radiotherapy following breast-conserving surgery for screen-detected ductal carcinoma in situ: indications and utilisation in the UK. Interim findings from the Sloane Project. British Journal of Cancer 2007; 97: NICE guidelines – Feb 2009 – Early and locally advanced breast cancer, diagnosis and treatement.")
31
Any questions?

Similar presentations










![ DISCUSSION Number of resected lymph nodes in esophageal surgery has been previously discussed as for its probable impact on patients’ survival [4]. The.](/14/4236498/big_thumb.jpg " DISCUSSION Number of resected lymph nodes in esophageal surgery has been previously discussed as for its probable impact on patients’ survival [4]. The.>")











