Download presentation
Presentation is loading. Please wait.

1
Inborn errors of metabolism: emergency management

2
Classification of inborn errors of metabolism: (IEM) I: Intoxication disorders II: energy metabolism disorders III: complex molecules disorders
 I: Intoxication disorders II: energy metabolism disorders III: complex molecules disorders")
3
Presenting features Acute presentation Vomiting Dehydration Lethargy Coma Rhabdomyolysis Heart failure Liver failure ALTE Respiratory failure (as complication) Chronic presentation FTT Hepatomegaly Cardiomyopathy Developmental delay Developmental regression
 Chronic presentation FTT Hepatomegaly Cardiomyopathy Developmental delay Developmental regression")
4
Triggers for decompensation Increased catabolism Increased consumption Fasting Surgery Trauma infection Increased protein consumption

5
Metabolic Causes of acute decompensation Neurology --------------- MSUD MMA PA IVA MCD UCD FAO RCD SEIZURE -------------- B6 responsive MCD Folonic acid disorders Glucose up-take Liver failure ----------------- GALACTOSEMIA Tyrosinemia Bile acid synthesis RCD GSD Cardiac failure & Cardiac beat, ALTE --------------- Carnitine disorders FAO Storage diseases

6
Neurology decompensation (acute encephalopathy) Definitions: Consciousness: a state of general wakefulness and responsiveness to environment Coma: A state of deep, unarousable, in which the person shows no meaningful response to environment consciousness sleep lethargy stupor coma
 Definitions: Consciousness: a state of general wakefulness and responsiveness to environment Coma: A state of deep, unarousable, in which the person shows no meaningful response to environment consciousness sleep lethargy stupor coma")
7
Background physiology Consciousness requires two components: 1- Arousal or wakefulness, dependent on the function of Reticular Activating System (RAS), a network of neurons located in the brainstem extending from pons to thalamus 2- Awareness, mediated through cerebral neurons Awareness requires wakefulness and not vice versa
, a network of neurons located in the brainstem extending from pons to thalamus 2- Awareness, mediated through cerebral neurons Awareness requires wakefulness and not vice versa")
8
structuralMetabolic-toxic traumaHypoxia-ischemia neoplasmMetabolic disorders Hypoglycemia, hepatic, electrolytes, DKA, uremia Vascular Infarction, haemorrhage, vasculitis infection Focal infection Abscess, cerebritis Paroxysmal disorders Epilepsy, migraine hydrocephalus Classification of causes of acute encephalopathy

10
Patient assessment Primary survey: A B C DISABILITY – Glascow Coma Scale, useful objective tool for the quantification of the consciousness-coma continuum Secondary survey:

11
Glascoma score Eyes open spontaneously +4 Eye opening to verbal command +3 Eye opening to pain +2 Eye opening to pain +1 Not assessable 0 Best Verbal Response Oriented +5 Confused +4 Inappropriate words +3 Incomprehensible sounds +2 No verbal response +1 Intubated 0 Best Motor Response Obeys commands +6 Localizes pain +5 Withdrawal from pain +4 Flexion to pain +3 Extension to pain +2 No motor response +1

12
Investigations of encephalopathy patient Laboratory investigations CBC Electrolytes LFT Coagulation profiles BUN, Cr, Ca, Mg, PO4 Ammonia Lactate CPK Glucose ABG Imaging studies CT/MRI MRI

13
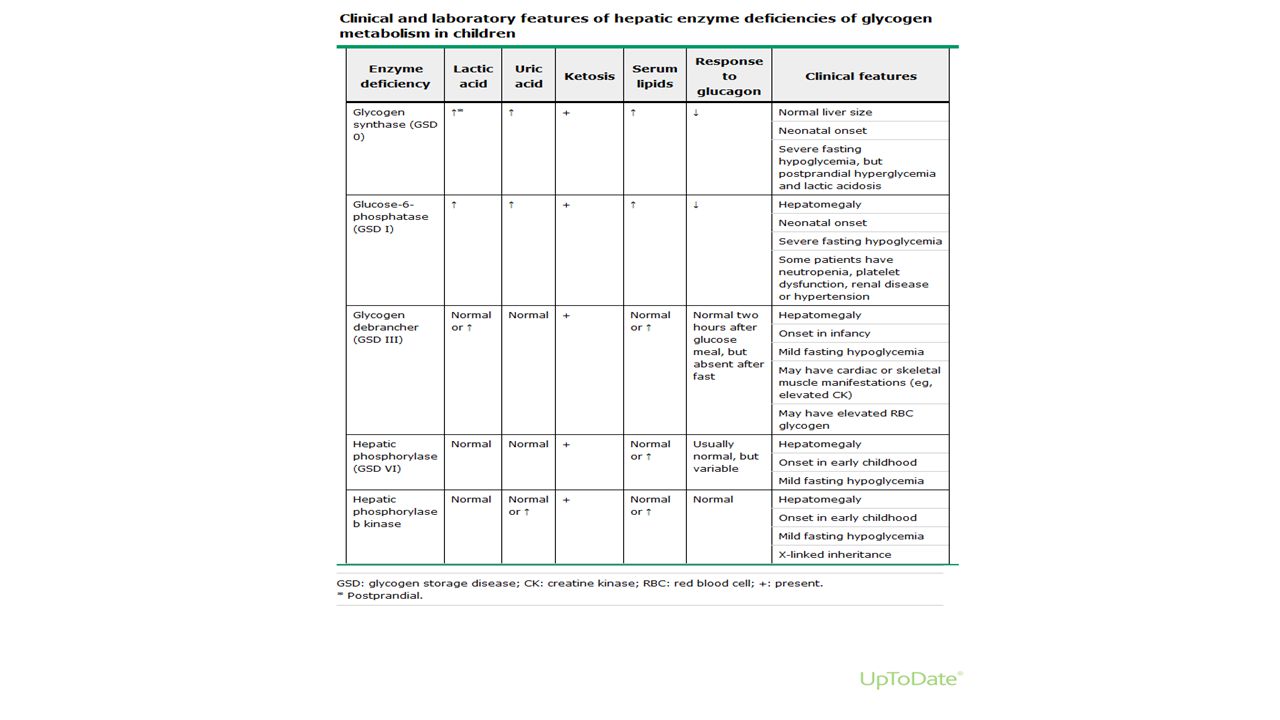
HYPOGLYCEMIA acidemia No acidemia LA KETONES I G6PD F1,6P Normal Ketotic hypoglycemia Debrancher enzyme GH d Cortisol d I FFA ketones FAO FFA ketones hyperinsulinism

14
HYPERAMONEMIA

15
Bedside differential diagnosis of inborn errors of metabolism presenting with hyperammonemia ParameterCondition UCDs Organic acidurias β-Oxidation defects Hyperinsulini sm- hyperammon emia syndrome Pyruvate carboxylase deficiency g Acidosis+/–+ e +/––+ Ketonuria a –+––++ Hypoglycemia b –+/–+++ ↑ Lactic acid c –++/––+ ↑ AST & ALT(+)d(+)d –+–+/– ↑ CPK––+–– ↑ Uric acid–++–– ↓ WBC/RBC/Plt –+––– Weight loss–+f+f ––+ In addition to the conditions indicated in the table, mitochondrial oxidative phosphorylation defects, citrin deficiency, lysinuric protein intolerance or
d(+)d –+–+/– ↑ CPK––+–– ↑ Uric acid–++–– ↓ WBC/RBC/Plt –+––– Weight loss–+f+f ––+ In addition to the conditions indicated in the table, mitochondrial oxidative phosphorylation defects, citrin deficiency, lysinuric protein intolerance or")
16
findingsMSUDOAUCDDCMFAOMDPDLSD Metabolic acidosis +-+- ++-+-+- +-+- +-+- -- Respiratory alkalosis --+----- Hyperammon emia +-+- ++++-+-+- +-+- -- Hypoglycemia +-+- +-+- -+-+-+- -- Ketones A/HHA A/LA/HAA Lactic acidosis =-=- +-+- -++-+- ++-- DISTINGUISHING BIOCHEMICAL FINDINGS OF IEM

17
Emergency treatment Ventilator support Fluid resuscitation with saline Hypoglycemia: 7-10 mg/kg/min, keep blood sugar more than 5.5mmol/l Hyperammonemia: glucose 10mg/kg/min over 2 hours: Arginine 360mg/kg Na benzoate & or phenylacetate 250mg/kg (max 500/kg) carnitine 100mg/kg maintains: as above Carbaglu in organic academia and UCD 100-200/kg stat, then 100 mg/kg/d Metabolic acidosis: PH (more than 7.3) 4-6 meq/kg/d PH (less than 7.3) 1-2 meq/kg/hr to be tapered accordingly
 carnitine 100mg/kg maintains: as above Carbaglu in organic academia and UCD /kg stat, then 100 mg/kg/d Metabolic acidosis: PH (more than 7.3) 4-6 meq/kg/d PH (less than 7.3) 1-2 meq/kg/hr to be tapered accordingly")
18
Disorder Distinctive Features KetosisAcidosisOthercofactor Maple syrup urine diseaseMaple syrup urine disease (MSUD) 1 XMaple syrup odorthiamine Propionic academiaPropionic academia 2 XXNeutropeniabiotin Methylmalonic acidemiaMethylmalonic acidemia (MMA) XXNeutropeniaB12 Methylmalonic aciduria and homocystinuria, cblC type Rare Vomiting, poor feeding, neurologic symptoms B12, pyrodoxin Isovaleric academia 1 XSweaty feet odor Biotin-unresponsive 3-methylcrotonyl- CoA carboxylase deficiency XHypoglycemia 3-hydroxy-3- methylglutaryl-CoA (HMG-CoA) lyase deficiency Reye syndrome, hypoglycemia Ketothiolase deficiency (mitochondrial acetoacetyl-CoA thiolase deficiency) XXHypoglycemia Glutaricacidemia type I (GA I) Basal ganglia injury with movement disorder riboflavin Clinical Findings in Organic Academia's Caused by Abnormal Amino Acid Catabolism
 1 XMaple syrup odorthiamine Propionic academiaPropionic academia 2 XXNeutropeniabiotin Methylmalonic acidemiaMethylmalonic acidemia (MMA) XXNeutropeniaB12 Methylmalonic aciduria and homocystinuria, cblC type Rare Vomiting, poor feeding, neurologic symptoms B12, pyrodoxin Isovaleric academia 1 XSweaty feet odor Biotin-unresponsive 3-methylcrotonyl- CoA carboxylase deficiency XHypoglycemia 3-hydroxy-3- methylglutaryl-CoA (HMG-CoA) lyase deficiency Reye syndrome, hypoglycemia Ketothiolase deficiency (mitochondrial acetoacetyl-CoA thiolase deficiency) XXHypoglycemia Glutaricacidemia type I (GA I) Basal ganglia injury with movement disorder riboflavin Clinical Findings in Organic Academia s Caused by Abnormal Amino Acid Catabolism")
19
Acute management of newborn with suspected organic acidemia 1) The patient is kept nil per orally and intravenous glucose is provided. 2) Supportive care: hydration, treatment of sepsis, seizures, ventilation. 3) Carnitine: 100 mg/kg/day IV or oral. 4) Treat acidosis: Sodium bicarbonate 0.35-0.5mEq/kg/hr (max 1-2mEq/kg/hr) 5) Start Biotin 10 mg/day orally. 6) Start Vitamin B12 1-2 mg/day I/M (useful in B12 responsive forms of methylmalonic acidemias) 7) Start Thiamine 300 mg/day (useful in thiamine- responsive variants of MSUD). 8) If hyperammonemia is present, treat as explained above.
 Supportive care: hydration, treatment of sepsis, seizures, ventilation. 3) Carnitine: 100 mg/kg/day IV or oral. 4) Treat acidosis: Sodium bicarbonate mEq/kg/hr (max 1-2mEq/kg/hr) 5) Start Biotin 10 mg/day orally. 6) Start Vitamin B mg/day I/M (useful in B12 responsive forms of methylmalonic acidemias) 7) Start Thiamine 300 mg/day (useful in thiamine- responsive variants of MSUD). 8) If hyperammonemia is present, treat as explained above..")
20
Discontinue all feeds. Provide adequate calories by intravenous glucose and lipids. Maintain glucose infusion rate 8-10 mg/kg/min. Start intravenous lipid 0.5 g/kg/day (up to 3g/kg/day). After stabilization gradually add protein 0.25 g/kg till 1.5 g/kg/day. 2) Dialysis is the only means for rapid removal of ammonia, and hemodialysis is more effective and faster than peritoneal dialysis, however peritoneal dialysis may be more widely available and feasible. Exchange transfusion is not useful. 3) Alternative pathways for nitrogen excretion-: Sodium benzoate (IV or oral)- loading dose 250 mg/kg then 250-400 mg/kg/day in 4 divided doses. (Intravenous preparation not available in India). Sodium phenylbutyrate (not available in India)-loading dose 250 mg/kg followed by 250-500 mg/kg/day. L-arginine (oral or IV)- 300 mg/kg/day (Intravenous preparation not available in India) L-carnitine (oral or IV)- 200 mg/kg/day 4) Supportive care: treatment of sepsis, seizures, ventilation. Avoid sodium valproate. Treatment of hyperammonemia
. After stabilization gradually add protein 0.25 g/kg till 1.5 g/kg/day. 2) Dialysis is the only means for rapid removal of ammonia, and hemodialysis is more effective and faster than peritoneal dialysis, however peritoneal dialysis may be more widely available and feasible. Exchange transfusion is not useful. 3) Alternative pathways for nitrogen excretion-: Sodium benzoate (IV or oral)- loading dose 250 mg/kg then mg/kg/day in 4 divided doses. (Intravenous preparation not available in India). Sodium phenylbutyrate (not available in India)-loading dose 250 mg/kg followed by mg/kg/day. L-arginine (oral or IV)- 300 mg/kg/day (Intravenous preparation not available in India) L-carnitine (oral or IV)- 200 mg/kg/day 4) Supportive care: treatment of sepsis, seizures, ventilation. Avoid sodium valproate. Treatment of hyperammonemia.")
21
Supportive care: hydration, treatment of sepsis, seizures, ventilation. Avoid sodium valproate. 2) Treat acidosis: sodium bicarbonate 0.35-0.5mEq/kg/hr (max 1-2mEq/kg/hr) 3) Thiamine: up to 300 mg/day in 4 divided doses. Riboflavin: 100 mg/day in 4 divided doses. 5) Add co-enzyme Q: 5-15 mg/kg/day 6) L-carnitine: 50-100 mg/kg orally. 7) Biotin 10 mg/day. (Biotin responsive Multiple carboxylase deficiency may present with unexplained lactic acidosis)12
 Treat acidosis: sodium bicarbonate mEq/kg/hr (max 1-2mEq/kg/hr) 3) Thiamine: up to 300 mg/day in 4 divided doses. Riboflavin: 100 mg/day in 4 divided doses. 5) Add co-enzyme Q: 5-15 mg/kg/day 6) L-carnitine: mg/kg orally. 7) Biotin 10 mg/day. (Biotin responsive Multiple carboxylase deficiency may present with unexplained lactic acidosis)12.")
Similar presentations














.>")





 for last 4 hours. He is.>")
>")