Download presentation
Presentation is loading. Please wait.

1
of Disorders Sodium By Mohammad El-Tahlawi

2
To Understand : The differences between sodium concentration and content. The causes and management of hypernatermia. OBJECTIVES

3
. Effective and ineffective osmoles Effective osmoles NaCl, glucose, mannitol (ECF) Kcl (ICF) contribute to tonicity. Ineffective osmoles urea and ethanol with effective osmoles, contribute to osmolarity. Osmolarity and osmolality Osmolarity number of osmoles per liter. Osmolality number of osmoles per kg of solvent.

4
Plasma Osmolarity (280-295 mOsm/l ) = 2 Na (Na+Cl )+ Glucose + Urea 18 2.8 18 2.8 = 2Na + 10 Plasma Tonicity (285 mOsm/l ) Plasma Tonicity (285 mOsm/l ) = 2Na + Glucose 18 18
 = 2 Na (Na+Cl )+ Glucose + Urea = 2Na + 10 Plasma Tonicity (285 mOsm/l ) Plasma Tonicity (285 mOsm/l ) = 2Na + Glucose 18 18")
5
Na content (hemostasis): determines ECF volume. balance between Na intake and excretion. -Intake < Excretion → -ve balance → ECF shrinks. -Intake > Excretion → +ve balance → ECF expands. Intake : enteral or parenteral.(normally 50-300mEq Na/day) Excretion renal (mainly).(normally 100-70 mEq/day). skin, GIT, burn and diarrhea (less). Na content and concentration
 Excretion renal (mainly).(normally mEq/day). skin, GIT, burn and diarrhea (less). Na content and concentration.")
6
determined by water intake and excretion Intake oral or IV fluids (hospitalized patient) 2500 ml/day. physiologic stimulus is thirst. Excretion 2500 ml. determinants of excretion : EABV - Absolute blood volume. - COP. - SVR. ADH Na concentration

7
HYPERNATERMIA ( > 145 )
")
8
Etiology: I. Decrease in TBW: A. Increase loss: Trough kidney -DI -DI -DM -DM -Dieuretics -Dieuretics Through skin&lung -Heat stroke -Heat stroke -Burns -Burns -Hyperventilation -Hyperventilation Through GIT -Diarrhea -Diarrhea -Hypertonic enema -Hypertonic enema B. Decreased intake: -Impaired thirst mechnism -Impaired thirst mechnism -Coma -Coma

10
II. Increase in Na intake: Infusion of NaHCO3 and other Na salts. Infusion of NaHCO3 and other Na salts. Selective depression of thirst centre (cerebral tumors,polio,meningitis..) Selective depression of thirst centre (cerebral tumors,polio,meningitis..) Essential hypernatraemia: resetting of osmoreceptors from 140 to 150 mEq/L. Essential hypernatraemia: resetting of osmoreceptors from 140 to 150 mEq/L. III. Decreased in Na excretion: Hyperaldosteronism. Hyperaldosteronism. Cushing syndrome. Cushing syndrome.
 Selective depression of thirst centre (cerebral tumors,polio,meningitis..) Essential hypernatraemia: resetting of osmoreceptors from 140 to 150 mEq/L. Essential hypernatraemia: resetting of osmoreceptors from 140 to 150 mEq/L. III. Decreased in Na excretion: Hyperaldosteronism. Hyperaldosteronism. Cushing syndrome. Cushing syndrome..")
11
Effect of hypernatremia Cell volume contraction and dehydration. Cell shrinkage is greatest in the brain (rigid clavarium ). Tearing of the bridging vessels intracranial hemorrhage Cells generate idiogenic osmoles (few hours to days ).
. Tearing of the bridging vessels intracranial hemorrhage Cells generate idiogenic osmoles (few hours to days )..")
12
Ranging from agitation to coma and seizures. clinical picture of : volume overload (hypertonic hypernatremia). volume depletion (loss of hypotonic fluid). Presentation It depends on magnitude and rate of rise.
. volume depletion (loss of hypotonic fluid). Presentation It depends on magnitude and rate of rise..")
13
Hypervolemic hypernatremia: Loop diuretics. Replace water deficit. Hypovolemic hypernatremia Restoring vascular volume quickly. Replace water deficit. Isovolemic hypernatremia Replacing water deficit over 48 -72 hours. Rate of decrease ≤ 0.5 meq/l per hr. Half of free water in the first 24 hours. Remaining half over 24-48 hours. Treatment

14
Fluid replacement. If urine output > 300 ml/hr : - Aqueous vasopressin (5 U Sc/4 hr). - Vasopressin in oil ( 0.3 ml IM/day ). - Desmopressin ( 5-10 U/day ). Central DI
. - Desmopressin ( 5-10 U/day ). Central DI.")
15
Nephrogenic DI Stop offending drugs. Correct electrolyte disorders. Salt and protein restriction. Thiazide. NSAI. Amiloride.

16
Correction of hypernatraemia Thirst=water deficit 2%of wt. Thirst=water deficit 2%of wt. Thirst+ oliguria=water deficit 6%of wt Thirst+ oliguria=water deficit 6%of wt Thirst+oliguria+CNS manif.=water deficit 8% of wt. Thirst+oliguria+CNS manif.=water deficit 8% of wt.

17
To calculate water deficit We can use the follwing formula: We can use the follwing formula: -Measured Na x Actual TBW= Initial(normal)Na x Normal TBW But water deficit=NormalTBW-Measured TBW -So Water deficit= (Measured TBW x Measured sNa/Normal sNa)- Measured TBW -TBW=Bwt x 60%
Na x Normal TBW But water deficit=NormalTBW-Measured TBW -So Water deficit= (Measured TBW x Measured sNa/Normal sNa)- Measured TBW -TBW=Bwt x 60%")
18
Formula for infusate containg sodium (Infusate sodium-serum sodium ) divided by TBW+1 5%D/W 0 INFUSATE SODIUM. 5%D/W 0 INFUSATE SODIUM. 0.2 NaCl 34 infusate sodium. 0.2 NaCl 34 infusate sodium. 0.45 NaCl 77 infusate sodium. 0.45 NaCl 77 infusate sodium. 0.9 NaCl 154 infusate sodium. 0.9 NaCl 154 infusate sodium.

19
Practical approach We should add the daily needs of water. We should add the daily needs of water. Causal management is essential. Causal management is essential. Correction should be gradual (over 2 days) or 2mEq/L/hr. Correction should be gradual (over 2 days) or 2mEq/L/hr. Replacement of water should contain some saline (e.g. D 5%, Saline 0.45) Replacement of water should contain some saline (e.g. D 5%, Saline 0.45) Frequently check for vascular overload Frequently check for vascular overload
 or 2mEq/L/hr. Correction should be gradual (over 2 days) or 2mEq/L/hr. Replacement of water should contain some saline (e.g. D 5%, Saline 0.45) Replacement of water should contain some saline (e.g. D 5%, Saline 0.45) Frequently check for vascular overload Frequently check for vascular overload.")
20
HYPONATERMIA ( <135 meq/l )
")
21
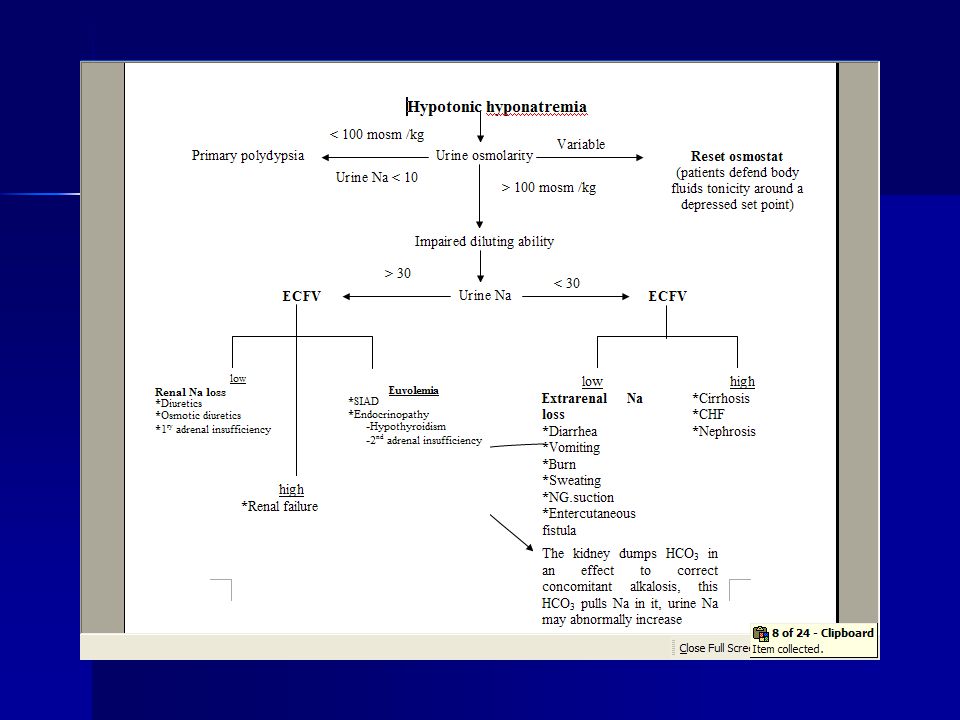
Increased non-aqueous volume of the serum sample. Hypertonic Hyponatermia Large amount of ECF osmotically effective solutes other than Na. Hypotonic hyponatremia Inability of the kidney to excrete sufficient electrolyte free water. Isotonic hyponatremia ( Pseudo-hyponatremia )
.")
23
Etiology Increase in TBW(Dilutional hyponatraemia): Increase in TBW(Dilutional hyponatraemia): 1. Increased intake:e.g excwss infusion of hyponatraemic solutions e.g dextrose in water. 2. Impaired free water clearance: e.g RF, CHF, LCF, SIADH..) Na depletion: Na depletion: 1. Decreased intake 2. Increased loss: -Through kidney: dieuretics, hypoaldosteronism, Addison ’ s disease. -Through kidney: dieuretics, hypoaldosteronism, Addison ’ s disease. -Through GIT: Diarrhea, vomiting.. -Through GIT: Diarrhea, vomiting.. -Through skin: excessive sweating, burns … -Through skin: excessive sweating, burns … K depletion: K leaks outside cells to keep K in plasma and this leads to Na influx to the cells. K depletion: K leaks outside cells to keep K in plasma and this leads to Na influx to the cells.
 Na depletion: Na depletion: 1. Decreased intake 2. Increased loss: -Through kidney: dieuretics, hypoaldosteronism, Addison ’ s disease. -Through kidney: dieuretics, hypoaldosteronism, Addison ’ s disease. -Through GIT: Diarrhea, vomiting.. -Through GIT: Diarrhea, vomiting.. -Through skin: excessive sweating, burns … -Through skin: excessive sweating, burns … K depletion: K leaks outside cells to keep K in plasma and this leads to Na influx to the cells. K depletion: K leaks outside cells to keep K in plasma and this leads to Na influx to the cells..")
24
Definition : Persistent unregulated secretion of ADH. Diagnosis: Hyponatremia Hypotonicity Euvolemia Urine osm. : (> 100 mosm/kg). Water loading test (unnecessary). Absence of endocrinal and diuretic causes. SIAD H
. Water loading test (unnecessary). Absence of endocrinal and diuretic causes. SIAD H.")
25
Conditions Associated with SIAD H: CNS (head trauma, stroke, tumour and meningitis ) Pulmonary (TB, pneumonia and abscess). Neoplastic (pancreatic and bronchogenic). Drugs ( Thiazide and NSAIDs).
. Drugs ( Thiazide and NSAIDs)..")
26
< 110 (seizures, coma and respiratory arrest). < 125 (anorexia, nausea and malaise). < 110-120 (headache, lethargy, confusion and agitation). Focal neurologic finding is unusual. Oedema (overhydration) in dilutional hyponat. but dehydration in Na depletion causes And normal hydration in K depletion causes. Clinical presentation
. Focal neurologic finding is unusual. Oedema (overhydration) in dilutional hyponat. but dehydration in Na depletion causes And normal hydration in K depletion causes. Clinical presentation.")
27
In acute hyponatraemia: Neurological manifestations appear rapidly In acute hyponatraemia: Neurological manifestations appear rapidly In chronic hyponatraemia: the severity of brain edema is less due to the slow compensatory loss of intracellular k, chloride and water thus protecting CNS. In chronic hyponatraemia: the severity of brain edema is less due to the slow compensatory loss of intracellular k, chloride and water thus protecting CNS.

28
Magnitude of rate of development. Age and gender. Nature and severity of underlying diseases. Mortality and Morbidity influenced by:

29
Assessment of hyponatraemia 1. Exclude lab. error (dilution of blood sample by running IV fluid). 2. Exclude pseudohyponatraemia (in cases of hyperglycaemia and hyperlipidaemia). 3. Exclude redistribution: (hyponatraemia due to hyperglycaemia or mannitol infusion: K deficiency. 4. Assess ECF volume. 5. Assess renal function and urine analysis for osmolarity and electrolytes.
. 3. Exclude redistribution: (hyponatraemia due to hyperglycaemia or mannitol infusion: K deficiency. 4. Assess ECF volume. 5. Assess renal function and urine analysis for osmolarity and electrolytes..")
30
Detect osmolarity (serum and urine).. Na (serum and urine). Assess ECF volume.. Necessity of rapid treatment. chronicity. presence or abcence of symptoms. degree of decrease. Management

31
Asymptomatic Hyponatermia (Chronic ) Hypovolemic hyponatermia Replace volume Euvolemic hyponatermia water restriction. Hypervolemic hyponatermia Salt and water restriction. Treatment of the cause : - Heart Failure. - Nephrotic syndrome. - Hepatic cirrhosis. - Renal Failure.

32
Symptomatic Hyponatermia Acute < 48 h. : - Hypertonic Saline 3% - Hypertonic Saline 3% 1-2 ml/kg/hr. 1-2 ml/kg/hr. - Frusemide. - Frusemide. Chronic > 48 h. or Unknown : - Hypertonic Saline - Hypertonic Saline 1-2ml/kg/hr. 1-2ml/kg/hr. - Frusemide. - Frusemide. - Change to water restriction. - Change to water restriction. - Frequent assessment - Frequent assessment - Not exceed 12 meq/l/day. - Not exceed 12 meq/l/day.

33
Practical approach Treatment of the cause Treatment of the cause Aim of correction: is to get a Na level of 120 mEq/L. Aim of correction: is to get a Na level of 120 mEq/L. Rate of correction: Rate of correction: 1. in acute cases:20 mEq/L/day 2. in chronic cases:12 mEq/L/day

34
Dilutional hyponatraemia: Dilutional hyponatraemia: 1. mild/moderate cases: fluid restriction by 600ml/h till clinical improvement or Na level > 130 2. Severe cases: -Lasix -Hypertonic saline -Hypertonic saline 3. Amount of Na needed= wt x 0.6 x (120 - measured Na)in male& wt x 0.5 x (120 - measured Na)in female Absolute hyponatraemia : Absolute hyponatraemia : Na needed = wt x 0.6 x (120 – measured Na) in male& wt x 0.5 x (120 - measured Na)in female
in male& wt x 0.5 x (120 - measured Na)in female Absolute hyponatraemia : Absolute hyponatraemia : Na needed = wt x 0.6 x (120 – measured Na) in male& wt x 0.5 x (120 - measured Na)in female.")
36
E.g: 80 Kg woman with sNa=118mmol/L. E.g: 80 Kg woman with sNa=118mmol/L. -Na deficit=80 x 0.5 x (130-118)=480mmol -Normal isotonic saline contains 154mmol/L of Na -so patient should receive 480/154=3.12L of normal saline in a rate of 0.5 mmol/L/hr -So it needs 24h i.e 130ml/hr
=480mmol -Normal isotonic saline contains 154mmol/L of Na -so patient should receive 480/154=3.12L of normal saline in a rate of 0.5 mmol/L/hr -So it needs 24h i.e 130ml/hr.")
Similar presentations













 = 2x (Na+>")







