Download presentation
Presentation is loading. Please wait.

1
Literature Review on ICH Brain Surgery School M.D. Taylor MD.

2
56 yr. Old Male, known HTN

4
Rationale for Surgical Treatment “Because that’s the way these cases were managed on my last rotation at ___________ “

5
Rationale for Surgical Treatment “ Dr. (insert COC here) is on call tonight and that is the way he manages this type of patient” COC= consultant of choice
 is on call tonight and that is the way he manages this type of patient COC= consultant of choice.")
6
What evidence is there in the literature for / against surgical treatment of HTN related ICH?

7
McKissock, Richardson and Taylor; Lancet 1961; 2: 221-226 Before CT era Clinical symptoms / LP / angiography 89 surgery: 91 conservative treatment

8
McKissock, Richardson and Taylor; Lancet 1961; 2: 221-226 MortalitySurgery65% BMM51% Poor OutcomeSurgery80% BMM66% No significant difference between treatment groups.

9
Juvela et al. J. Neurosurg 1989 ‘The treatment of spontaneous intracerebral hemorrhage’ Inclusion: Unconscious severe hemiparesis dysphasia admitted within 24 hours onset surgery within 48 hrs onset

10
Juvela et al. J. Neurosurg 1989 ‘The treatment of spontaneous intracerebral hemorrhage’ One center 26 pts surgical 26 pts. BMM ProspectiveRandomized No cerebellar, AVM, aneurysm

11
Juvela et al. J. Neurosurg 1989 ‘The treatment of spontaneous intracerebral hemorrhage’ MortalityOverall42% BMM38% Surgery46% ADLOverall 20% BMM31% Surgery7%

12
Juvela et al. J. Neurosurg 1989 ‘The treatment of spontaneous intracerebral hemorrhage’ “Mortality rate of patients with GCS in the range of 7-10 was significantly lower in the surgical group (0/4) than the BMM group (4/5) patients. p<0.05” BUT All survivors from this subgroup had very severe disabilities
 than the BMM group (4/5) patients. p<0.05 BUT All survivors from this subgroup had very severe disabilities.")
13
Juvela et al. J. Neurosurg 1989 ‘The treatment of spontaneous intracerebral hemorrhage’ “It is concluded that spontaneous supratentorial ICH’s should be treated conservatively”

14
Scoreboard Surgery0 BMM 2

15
Auer et al. J. Neurosurg 1989 Endoscopic Surgery vs. Medical Treatment for Spontaneous ICH: a Randomized Trial Randomized?Prospective One center50 surgical 50 BMM

16
Auer et al. J. Neurosurg 1989 Endoscopic Surgery vs. Medical Treatment for Spontaneous ICH: a Randomized Trial Inclusion criteria No underlying structural etiology age 30 to 80 years hematoma >10 cubic cm LOC or neuro deficit Medically stable Surgery within 48 hours of onset Location: subcortical / putaminal/ thalamic

17
Auer et al. J. Neurosurg 1989 Endoscopic Surgery vs. Medical Treatment for Spontaneous ICH: a Randomized Trial Outcomes at 6 months MortalitySurgery30% BMM70% (p<0.05) Good outcomeSurgery40% BMM25%
 Good outcomeSurgery40% BMM25%.")
18
Auer et al. J. Neurosurg 1989 Endoscopic Surgery vs. Medical Treatment for Spontaneous ICH: a Randomized Trial “The outcome of surgical patients with putaminal or thalamic hemorrhage was no better than for those with medical treatment” ?A rationale for operating on subcortical hematomas

19
Scoreboard Surgery0 BMM 3

20
H.H. Batjer et al. Arch Neurol. 1990 “Failure of Surgery to Improve Outcome in Hypertensive Putaminal Hemorrhage. A Prospective Randomized Trial” ProspectiveRandomized One center

21
H.H. Batjer et al. Arch Neurol. 1990 “Failure of Surgery to Improve Outcome in Hypertensive Putaminal Hemorrhage. A Prospective Randomized Trial” Inclusion criteria: Putaminal ICH ICH >3cm in diameter 30-75 years of age History of HTN Present within 24 hours of onset LOC or neuro deficit

22
H.H. Batjer et al. Arch Neurol. 1990 “Failure of Surgery to Improve Outcome in Hypertensive Putaminal Hemorrhage. A Prospective Randomized Trial” 3 Arms 1) BMM and Microsurgery 2) BMM and ICP monitor (CSF drainage) 3) BMM alone
 BMM and Microsurgery 2) BMM and ICP monitor (CSF drainage) 3) BMM alone.")
23
H.H. Batjer et al. Arch Neurol. 1990 “Failure of Surgery to Improve Outcome in Hypertensive Putaminal Hemorrhage. A Prospective Randomized Trial” 3 Arms 1) BMM and Microsurgery8 pts 2) BMM and ICP monitor4 pts 3) BMM alone9 pts
 BMM and Microsurgery8 pts 2) BMM and ICP monitor4 pts 3) BMM alone9 pts.")
24
H.H. Batjer et al. Arch Neurol. 1990 “Failure of Surgery to Improve Outcome in Hypertensive Putaminal Hemorrhage. A Prospective Randomized Trial” ‘Study interrupted after 21 patients had been studied. No differences were found among groups for age, admission BP, time interval to hospital arrival” NO subjects capable of returning to prestroke activity

25
H.H. Batjer et al. Arch Neurol. 1990 “Failure of Surgery to Improve Outcome in Hypertensive Putaminal Hemorrhage. A Prospective Randomized Trial” Outcomes at 6 months MortalitySurgery 78% BMM 67% Poor outcomeSurgery78% BMM83%

26
H.H. Batjer et al. Arch Neurol. 1990 “Failure of Surgery to Improve Outcome in Hypertensive Putaminal Hemorrhage. A Prospective Randomized Trial” “These results suggest that current medical and neurosurgical therapies remain ineffective in preventing the devastating consequences of hypertensive putaminal hemorrhage”

27
Scoreboard Surgery0 BMM 4

28
Chen et al. Acta Acad Med Shanghai 1992. A prospective randomized trial of surgical and conservative treatment of hypertensive intracranial haemorrhage Article in Chinese ProspectiveRandomized

29
Chen et al. Acta Acad Med Shanghai 1992. A prospective randomized trial of surgical and conservative treatment of hypertensive intracranial haemorrhage Inclusion criteria No imminent herniation History of HTN 64 surgical 63 conservative Cohort included patients with cerebellar hematomas

30
Chen et al. Acta Acad Med Shanghai 1992. A prospective randomized trial of surgical and conservative treatment of hypertensive intracranial haemorrhage Outcomes at 3 months Mortality Surgery23% BMM17% Poor outcomeSurgery63% BMM50% “No difference between tx groups” (in spite of including cerebellar ICH)
.")
31
Scoreboard Surgery0 BMM 5

32
L. B. Morgenstern et al. Surgical treatment for intracerebral hemorrhage (STICH) ProspectiveRandomized Includes U of T alumnus P. Shedden But run by a Neurologist (hence cute name for the trial ‘Stich’)
 ProspectiveRandomized Includes U of T alumnus P. Shedden But run by a Neurologist (hence cute name for the trial ‘Stich’).")
33
L. B. Morgenstern et al. Surgical treatment for intracerebral hemorrhage (STICH) Inclusion criteria: >9ml clot GCS 5-15 within 12 hours of ictus Open craniotomy versus BMM
 Inclusion criteria: >9ml clot GCS 5-15 within 12 hours of ictus Open craniotomy versus BMM.")
34
L. B. Morgenstern et al. Surgical treatment for intracerebral hemorrhage (STICH) Outcome at 6 months MortalitySurgery24% BMM18% Poor outcomeSurgery 50% BMM69%
 Outcome at 6 months MortalitySurgery24% BMM18% Poor outcomeSurgery 50% BMM69%.")
35
L. B. Morgenstern et al. Surgical treatment for intracerebral hemorrhage (STICH) Conclusions ‘Early surgery is feasible’ ‘Modest benefit for survival among surgical cohort at one month but not by six months’
 Conclusions ‘Early surgery is feasible’ ‘Modest benefit for survival among surgical cohort at one month but not by six months’.")
36
Scoreboard Surgery0 BMM 6

37
Zuccarello et al. Stroke 1999 Early Surgical Treatment for Supratentorial Intracerebral Hemorrhage: A Randomized Feasibility Study RandomizedProspectiveMulti-centered

38
Inclusion criteria ICH volume >10 cm cubic focal neurologic deficit GCS>4 therapy within 24 hours of onset Surgery within 3 hours random. No aneurysm / AVM

39
Zuccarello et al. Stroke 1999 Early Surgical Treatment for Supratentorial Intracerebral Hemorrhage: A Randomized Feasibility Study Enrolled 9 surgical patients 11 BMM patients Intended to see whether early treatment is feasible

40
Zuccarello et al. Stroke 1999 Early Surgical Treatment for Supratentorial Intracerebral Hemorrhage: A Randomized Feasibility Study Results median time to presentation:3 hrs 17 min med rand to surgery: 1 hr 20 mins Onset to surgery: 8 hours, 35 minutes (it took 4 hours to randomize pts?)
.")
41
Zuccarello et al. Stroke 1999 Early Surgical Treatment for Supratentorial Intracerebral Hemorrhage: A Randomized Feasibility Study Outcomes: Poor outcomeSurgery44% BMM64% MortalitySurgery22% BMM27%

42
Zuccarello et al. Stroke 1999 Early Surgical Treatment for Supratentorial Intracerebral Hemorrhage: A Randomized Feasibility Study Outcomes 3 months GOS: no sig. Difference (primary outcome measure) GOS, Barthel index, Rankin scale: no sig. (secondary outcome measures)
 GOS, Barthel index, Rankin scale: no sig. (secondary outcome measures).")
43
Zuccarello et al. Stroke 1999 Early Surgical Treatment for Supratentorial Intracerebral Hemorrhage: A Randomized Feasibility Study BUT significant difference in NIH stroke scale (4 vs. 14; P=0.04) ? Significance of this finding
 . Significance of this finding.")
44
Zuccarello et al. Stroke 1999 Early Surgical Treatment for Supratentorial Intracerebral Hemorrhage: A Randomized Feasibility Study “Very early surgical treatment for acute ICH is difficult to achieve but feasible at academic medical centers and community hospitals.”

45
Scoreboard Surgery0.5 BMM 6

46
Meta-analysis anyone? If one is good, three must be better 1) Hankey GJ. Et al. Stroke 1997; 28: 2126-2132 2) Prasad K et al. Acta Neurol Scand 1997; 95: 103-110 3) Saver JL. Feldmann E. ed. Intracerebral Hemorrhage 1994: 303- 332
 Prasad K et al. Acta Neurol Scand 1997; 95: ) Saver JL. Feldmann E. ed. Intracerebral Hemorrhage 1994:")
47
Meta-analyses 4 RCTS, 3 meta-analyses Surgery no effect 2/3 Surgery may decrease mortality with poor quality of life 1/3

48
Stroke: A Journal of Cerebral Circulation © 1999 American Heart Association, Inc. Volume 30(4) April 1999 pp 905-915 Guidelines for the Management of Spontaneous Intracerebral Hemorrhage: A Statement for Healthcare Professionals From a Special Writing Group of the Stroke Council, American Heart Association [Aha Scientific Statement] Broderick, Joseph P. MD; Adams, Harold P. MD; Barsan, William MD; Feinberg, William MD; Feldmann, Edward MD; Grotta, James MD; Kase, Carlos MD; Krieger, Derek MD; Mayberg, Marc MD; Tilley, Barbara PhD; Zabramski, Joseph M. MD; Zuccarello, Mario MD
 April 1999 pp Guidelines for the Management of Spontaneous Intracerebral Hemorrhage: A Statement for Healthcare Professionals From a Special Writing Group of the Stroke Council, American Heart Association [Aha Scientific Statement] Broderick, Joseph P. MD; Adams, Harold P. MD; Barsan, William MD; Feinberg, William MD; Feldmann, Edward MD; Grotta, James MD; Kase, Carlos MD; Krieger, Derek MD; Mayberg, Marc MD; Tilley, Barbara PhD; Zabramski, Joseph M. MD; Zuccarello, Mario MD.")
49
AHA Guidelines # of RCT Ischemic stroke>315 SAH78 ICH4

50
AHA Guidelines 37,000 ICH in US in 1997 50% dead at one month half of deaths in first two days 10% living independantly at 1 month 20% living independantly at 6 months

51
AHA Guidelines Estimated 7000 operations a year in the United States for removal of ICH

52
AHA Guidelines

53
AHA Guidelines AHA Guidelines Diagnosis of ICH: Summary and Recommendations n n 1. ICH is a medical emergency of the highest degree with frequent early neurological deterioration or death. Vomiting, early change in level of consciousness, and high elevation of blood pressure in a patient with acute stroke suggest ICH.

54
AHA Guidelines AHA Guidelines Diagnosis of ICH: Summary and Recommendations n n 2. CT of the head is the imaging procedure of choice in the initial evaluation of suspected ICH (level of evidence I, grade A recommendation).
..")
55
AHA Guidelines AHA Guidelines Diagnosis of ICH: Summary and Recommendations n n 3. Angiography should be considered for all patients without a clear cause of hemorrhage who are surgical candidates, particularly young, normotensive patients who are clinically stable (level of evidence V, grade C recommendation).
..")
56
AHA Guidelines AHA Guidelines Diagnosis of ICH: Summary and Recommendations n n 4. Angiography is not required for older hypertensive patients who have a hemorrhage in the basal ganglia, thalamus, cerebellum, or brain stem and in whom CT findings do not suggest a structural lesion. (level of evidence V, grade C recommendation).
..")
57
AHA Guidelines AHA Guidelines Diagnosis of ICH: Summary and Recommendations n n 5. Timing of cerebral angiography depends on the patient's clinical state and the neurosurgeon's judgment concerning the urgency of surgery, if needed.

58
AHA Guidelines AHA Guidelines Diagnosis of ICH: Summary and Recommendations n n 6. MRI and MRA are helpful and may obviate the need for contrast cerebral angiography in selected patients. They should also be considered to look for cavernous malformations in normotensive patients with lobar hemorrhages and normal angiographic results who are surgical candidates (level of evidence V, grade C recommendation).
..")
59
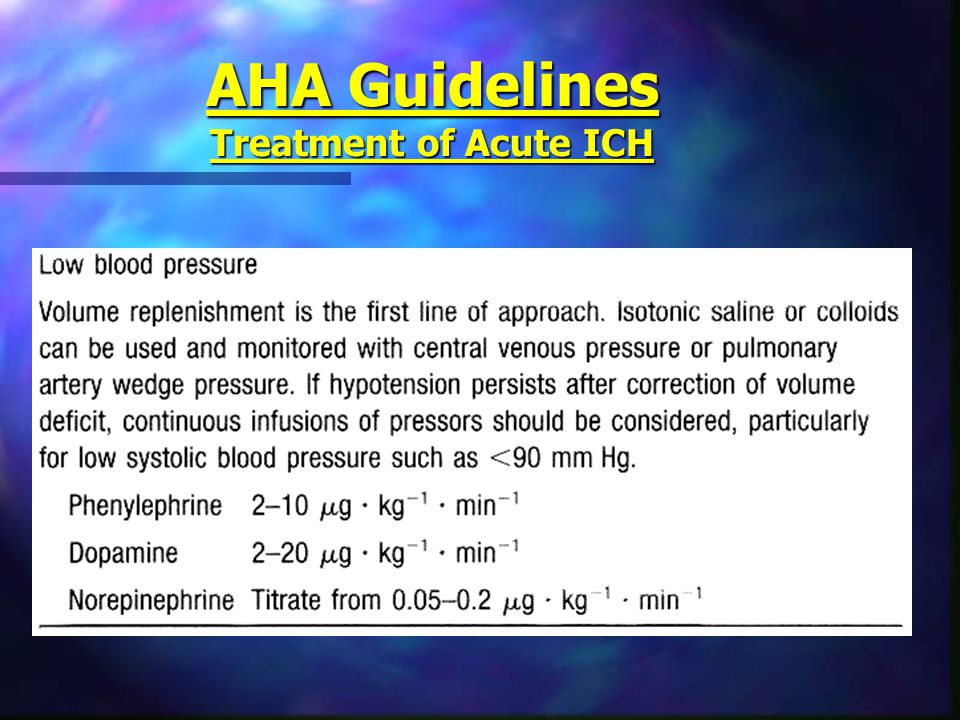
AHA Guidelines Treatment of Acute ICH No role for: SteroidsHemodilutionGlycerol (as per negative RCTs)
")
60
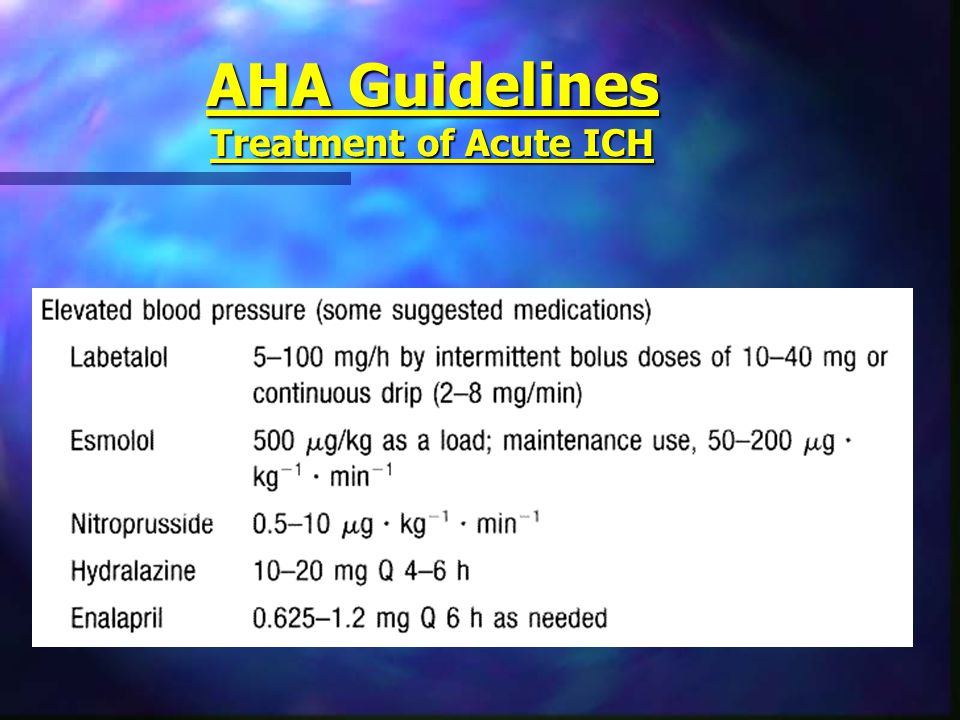
AHA Guidelines Treatment of Acute ICH

63
AHA Guidelines Treatment of ICP secondary to Acute ICH Sometimes Hyperosmolar solutions HyperventilationParalysisNeverCorticosteroids

64
AHA Guidelines Treatment of ICP secondary to Acute ICH ICP monitor for pt GCS <9 Ventricular drain in pts who have or are at risk for hydrocephalus

65
AHA Guidelines Role of Surgery for ICH

66
AHA Guidelines Prevention of ICH Grade ‘A’ Treat HTN Careful anticoagulation Careful thrombolysis Grade ‘C’ Lots of fruits and veggies avoid alcohol and sympathomimetics

67
56 yr. Old Male, known HTN

68
Interesting Papers

69
How do you account for clinical deterioration in the patient with ICH? ?edema?hydrocephalus ?rebleed / ongoing bleeding

70
Deterioration Brott T. et al. Stroke 1997: 28(1); 1-5 ‘Substantial early hemorrhage growth in patients with intracranial hemorrhage is common and is associated with neurological deterioration’
; 1-5 ‘Substantial early hemorrhage growth in patients with intracranial hemorrhage is common and is associated with neurological deterioration’.")
71
Deterioration Kazui S. et al. Stroke 1996: 27(10); 1783-1787 17% of hematomas expand Extremely rare after 24 hours
; % of hematomas expand Extremely rare after 24 hours.")
72
Deterioration Zazulia et al. Stroke 1999: 30(6); 1167-1173 Hematoma enlargement in first 2 days 2nd and 3rd weeks, edema Edema with larger hematomas Only 10/65 CT repeated for clinical deterioration showed increased mass effect
; Hematoma enlargement in first 2 days 2nd and 3rd weeks, edema Edema with larger hematomas Only 10/65 CT repeated for clinical deterioration showed increased mass effect.")
73
Deterioration Fujii Y. et al. Stroke 1998: 29(6); 1160-1166 Hematoma enlargement likely with: admission shortly after onset heavy drinkers irregularly shaped hematoma decreased LOC low serum level of fibrinogen
; Hematoma enlargement likely with: admission shortly after onset heavy drinkers irregularly shaped hematoma decreased LOC low serum level of fibrinogen.")
74
Hydrocephalus Diringer M et al. Stroke 1998: 29(7); 1352-1357 50% of pts with supratentorial ICH Hospital mortality 51% with hydro and only 2% without hydro With hydro only 21% of pts went home, without 35% went home No improvement with ventriculostomy
; % of pts with supratentorial ICH Hospital mortality 51% with hydro and only 2% without hydro With hydro only 21% of pts went home, without 35% went home No improvement with ventriculostomy.")
75
Hydrocephalus Phan T. et al. Stroke 2000: 31(9); 2157-2162 MortalityOverall29% w hydro76% Hydro only predictive of mortality for putaminal bleed, not thalamus etc. Hydro and GCS<8 Survival=11% No hydro, GCS>8Survival=100%
; MortalityOverall29% w hydro76% Hydro only predictive of mortality for putaminal bleed, not thalamus etc. Hydro and GCS<8 Survival=11% No hydro, GCS>8Survival=100%.")
76
Hydrocephalus Shapiro. et al. J. Neurosurg 1994: 80; 805-809 28/28 patients with hemorrhagic dilatation of the 4th ventricle died Some survivors if blood in the fourth but no dilatation

77
A.G. Thrift et al. Stroke 1996: 27(11), 2020-2025 ‘Risk Factors for Cerebral Hemorrhage in the Era of Well Controlled Hypertension’ HTN doubles the risk of ICH Use of aspirin not assoc. with ICH Reduced ICH with: CV disease Arthritis High Cholesterol Moderately overweight Using hormone replacement Drinking coffee
, ‘Risk Factors for Cerebral Hemorrhage in the Era of Well Controlled Hypertension’ HTN doubles the risk of ICH Use of aspirin not assoc. with ICH Reduced ICH with: CV disease Arthritis High Cholesterol Moderately overweight Using hormone replacement Drinking coffee.")
78
‘Blood Pressure Control and Recurrence of Hypertensive Brain Hemorrhage’ S. Arakawa et al. Stroke 1998: 29(9); 1806-1809 Diastolic BP sig higher in group with recurrent ICH (f/u=2.8 years) No effect of systolic BP No patient with DBP <70 mm Hg had a recurrent episode of ICH
; Diastolic BP sig higher in group with recurrent ICH (f/u=2.8 years) No effect of systolic BP No patient with DBP <70 mm Hg had a recurrent episode of ICH.")
79
‘Differing Temporal Patterns of Onset in Subgroups of Patients with ICH’ S. Passero et al. Stroke 2000: 31(7); 1538-1544 Risk of ICH greater on Monday among population with jobs Clustering of ICH in AM due to increase in sympathetic tone and BP on wakening
; Risk of ICH greater on Monday among population with jobs Clustering of ICH in AM due to increase in sympathetic tone and BP on wakening.")
80
‘Prognostic Value and Determinants of First Day Mean Arterial Pressure in Spontaneous Supratentorial Intracerebral Hemorrhage R. Fogelholm. Stroke 1997: 28(7); 1396-1400 Most important predictors of 28 day survival: Level of consciousness First day MAP (bad if >145 mm Hg)
; Most important predictors of 28 day survival: Level of consciousness First day MAP (bad if >145 mm Hg).")
81
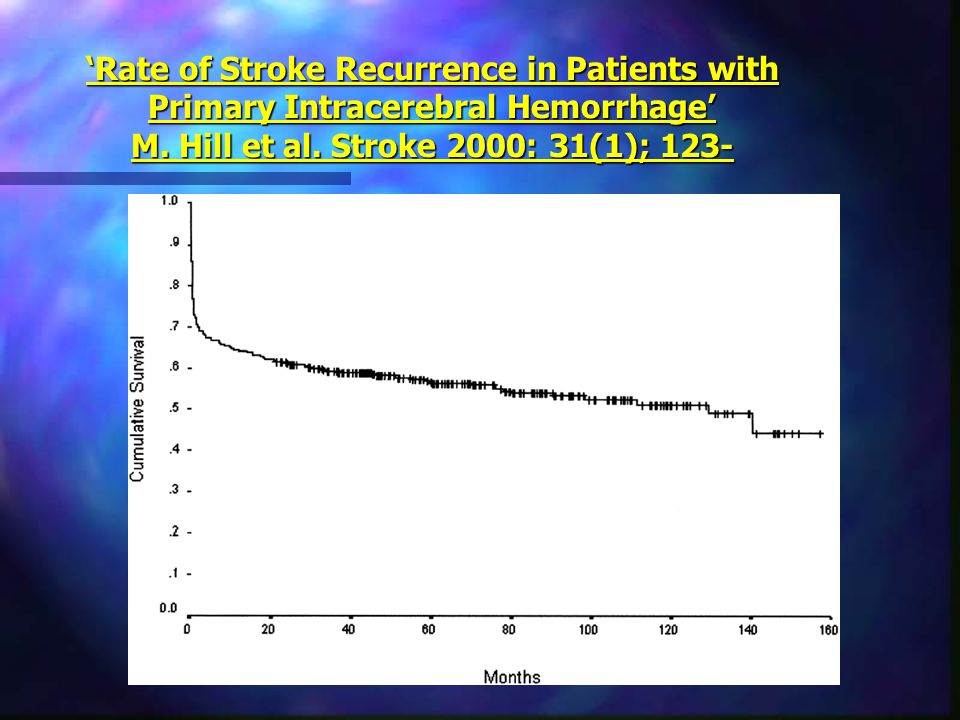
‘Rate of Stroke Recurrence in Patients with Primary Intracerebral Hemorrhage’ M. Hill et al. Stroke 2000: 31(1); 123- Survivors 2.4% risk/year for recurrent ICH 3.0% risk/year for ischemic stroke Nice data set to look at as it consists of 431 cases of ICH, all from TWH
; 123- Survivors 2.4% risk/year for recurrent ICH 3.0% risk/year for ischemic stroke Nice data set to look at as it consists of 431 cases of ICH, all from TWH.")
82
‘Rate of Stroke Recurrence in Patients with Primary Intracerebral Hemorrhage’ M. Hill et al. Stroke 2000: 31(1); 123-
;")
85
‘MRI Features of Intracerebral Hemorrhage Within 2 Hours From Symptom Onset’ I. Linfante et al. Stroke 1999: 30(11); 2263-2267 These authors managed to get an MRI within 23 minutes of symptom onset in one patient.
; These authors managed to get an MRI within 23 minutes of symptom onset in one patient..")
86
‘Spontaneous Intracranial Hemorrhage: Which Patients Need Diagnostic Cerebral Angiography?: A Prospective Study of 206 cases and Review of the Literature’ Zhu et al. Stroke 1997: 28(7); 1406-1409 “Diagnostic cerebral angiography should be considered for all spontaneous ICH patients except those over 45 years old with preexisting HTN in thalamic, putaminal, or post-fossa hemorrhages.”
; Diagnostic cerebral angiography should be considered for all spontaneous ICH patients except those over 45 years old with preexisting HTN in thalamic, putaminal, or post-fossa hemorrhages. .")
87
“Predicting neurologic deterioration in patients with cerebellar hematomas” St. Louis EK. Et al. Neurology 1998: 51; 1364-1369 High risk for deterioration: Hydrocephalus Vermian hematoma

88
‘Apolipoprotein E Genotype and the Risk of Recurrent Lobar Intracerebral Hemorrhage’ O’Donnell et al. New Eng J Med 2000: 342; 240-5 2 year follow-up E3/E3 genotype10% recurrence E2 or E4 allele28% recurrence

Similar presentations




 Prof. Dr. Leónidas M. Quintana Prof. Dr. Leónidas M. Quintana Department.>")







: A Randomised Trial Edward P. Sloan, MD, MPH, FACEP.>")







 Clinical Trial T. Morgan, M. Zuccarello,>")
: Johnston, S Claiborne MD, PhD; Dowd, Christopher F. MD; Higashida, Randall T. MD; Lawton, Michael T. MD; Duckwiler, Gary R. MD; Gress, Daryl.>")