Download presentation
Presentation is loading. Please wait.

1
Anemia management in Haemodialyis patients

3
Life cycle of RBCs

4
Anemia-definition Males: Hb < 13.5 g/dL in Females:
The Kidney Disease Outcomes Quality Initiative (KDOQI) (2006)
 (2006)")
5
Anemia in CKD-Causes Erythropoietin deficiency Iron deficiency
RBC life span is shortened(40% to 60% of normal) Haemolysis Blood loss related to access and dialysis
 Haemolysis. Blood loss related to access and dialysis.")
6
Anemia in CKD-Causes Inadequate dialysis Hyperparathyroidism
Vitamin B12 or folate deficiency Chronic infection or inflammation

7
Why anemia treatment is important ?
Fatigue and impaired cognition Increases hospitalization Increases mortality Left Ventricular Hypertrophy

8
When to work up anaemia in CKD patients?
Males and for post menopausal women Haemoglobin < 12gms%, Haematocrit < 36% Pre menopausal women and Adolescents Haemoglobin < 11gms%, Haematocrit < 33% patients on haemodialysis haemoglobin concentration to be measured from pre-dialysis sample Best Practice Guidelines for management of Renal Anaemia, Indian J Nephrol 2005;15, Supplement 1: S32-S41

9
Anaemia Evaluation Hb concentration
RBC indices / Peripheral smear / Reticulocyte count Tranferrin saturation Stool occult blood Stool parasite test Best Practice Guidelines for management of Renal Anaemia, Indian J Nephrol 2005;15, Supplement 1: S32-S41

10
Anaemia Evaluation Iron / TIBC / Ferritin
Serum B12 and red cell folate concentrations Differential white blood count Tests for haemolysis (hapatoglobin, LDH) Serum and / or urine protein electrophoresis Bone marrow examination in selected cases Best Practice Guidelines for management of Renal Anaemia, Indian J Nephrol 2005;15, Supplement 1: S32-S41
 Serum and / or urine protein electrophoresis. Bone marrow examination in selected cases. Best Practice Guidelines for management of Renal Anaemia, Indian J Nephrol 2005;15, Supplement 1: S32-S41.")
11
Anaemia Evaluation Assessment of occult gastrointestinal blood loss
Intact PTH Chronic Infections Serum Aluminium adequacy of dialysis to be assessed Best Practice Guidelines for management of Renal Anaemia, Indian J Nephrol 2005;15, Supplement 1: S32-S41

16
Iron deficiency True iron deficiency:
caused by blood loss and/or not receiving enough iron. Lab values: Tsat < 20 and ferritin < 200. Functional iron deficiency: Not enough iron is delivered to the marrow. Lab values: falling Tsat and rising ferritin.

17
KDOQI (2006) targets for patients on dialysis
Transferrin saturation (Tsat) > 20%, no upper limit specified Ferritin lower limit > 200 ng/mL. Ferritin>500 ng/ml not routinely recommended.
 > 20%, no upper limit specified. Ferritin lower limit > 200 ng/mL. Ferritin>500 ng/ml not routinely recommended.")
18
Treatment of Anemia with Iron
IV administration of iron is an optimum route of delivery of iron in HD patients Oral iron is poorly absorbed. Best Practice Guidelines for management of Renal Anaemia, Indian J Nephrol 2005;15, Supplement 1: S32-S41

19
IV Iron dose To correct iron deficiency:
1 gram IV iron in divided doses 100 mg doses of iron sucrose injection on 10 consecutive dialysis sessions Reassess iron status and repeat if necessary. Maintenance Treatment: Smaller doses administered at regular intervals to maintain iron status within target. The average IV iron dose needed to maintain a stable ferritin level appears to be in the range of 22 to 65 mg/week.

20
History of IV iron in renal anemia
The regular use of colloidal IV iron preparations in the treatment of the anemia of ESRD patients on maintenance hemodialysis was first reported in 1967 After the beginning of the erythropoietin era, IV iron was continued 1993 very low erythropoietin requirements in a series of patients on maintenance hemodialysis was reported with use of IV iron Iron sucrose was approved for use by the US FDA in November 2000 The regular use of colloidal IV iron preparations in the treatment of the anemia of ESRD patients on maintenance hemodialysis was first reported in After the beginning of the erythropoietin era, use of IV iron was continued very low erythropoietin requirements in a series of patients on maintenance hemodialysis was reported with use of IV iron. Iron sucrose was approved for use by the US FDA in November 2000 Ref: Shaldon S. The use of IV iron in the treatment of anaemia of ESRD patients on maintenance haemodialysis: an historical and personal view. Nephrol Dial Transplant (2007) 22: 23–25. Shaldon S. The use of IV iron in the treatment of anaemia of ESRD patients on maintenance haemodialysis: an historical and personal view. Nephrol Dial Transplant (2007) 22: 23–25. 20
 22: 23–25. Shaldon S. The use of IV iron in the treatment of anaemia of ESRD patients on maintenance haemodialysis: an historical and personal view. Nephrol Dial Transplant (2007) 22: 23–")
21
Problems in anemia management in CKD
Common challenges faced are – Maintenance of stable hemoglobin levels in their patients Avoid overshooting Hb targets Balance intravenous iron & EPO Improve EPO response to use the lowest effective EPO dose A major concern is EPO hyporesponsiveness & insufficient iron replacement IV iron is important in managing these challenges to a large extent Clinicians who manage anemia in patients with chronic kidney disease, both on and off dialysis therapy, face several challenges: maintain stable hemoglobin (Hb) levels in their patients, avoid overshooting Hb targets, balance intravenous (IV) iron and EPO and improve EPO response to use the lowest effective EPO dose. A major concern is EPO hyporesponsiveness & insufficient iron replacement IV iron is important in managing these challenges to a large extent, particularly in hemodialysis patients who have anemia despite adequate EPO doses, was shown in the randomized controlled Dialysis Patients' Response to IV Iron with Elevated Ferritin (DRIVE) clinical trial and its 6-week follow-up extension study, DRIVE-II. These studies provide suggestive evidence of the ability of IV iron to reduce ESA requirements and maintain improved Hb levels in anemic hemodialysis patients with serum ferritin levels of 500 to 1,200 ng/mL and transferrin saturations of 25% or less. Ref: Kapoian T. Challenge of effectively using erythropoiesis-stimulating agents and intravenous iron. Am J Kidney Dis Dec;52(6 Suppl):S21-8. Kapoian T. Challenge of effectively using erythropoiesis-stimulating agents and intravenous iron. Am J Kidney Dis Dec;52(6 Suppl):S21-8. 21
 levels in their patients, avoid overshooting Hb targets, balance intravenous (IV) iron and EPO and improve EPO response to use the lowest effective EPO dose. A major concern is EPO hyporesponsiveness & insufficient iron replacement. IV iron is important in managing these challenges to a large extent, particularly in hemodialysis patients who have anemia despite adequate EPO doses, was shown in the randomized controlled Dialysis Patients Response to IV Iron with Elevated Ferritin (DRIVE) clinical trial and its 6-week follow-up extension study, DRIVE-II. These studies provide suggestive evidence of the ability of IV iron to reduce ESA requirements and maintain improved Hb levels in anemic hemodialysis patients with serum ferritin levels of 500 to 1,200 ng/mL and transferrin saturations of 25% or less. Ref: Kapoian T. Challenge of effectively using erythropoiesis-stimulating agents and intravenous iron. Am J Kidney Dis Dec;52(6 Suppl):S21-8. Kapoian T. Challenge of effectively using erythropoiesis-stimulating agents and intravenous iron. Am J Kidney Dis Dec;52(6 Suppl):S")
22
IV iron in CKD IV iron therapy is superior to oral iron supplementation in CKD Risk factors associated with IV iron therapy include acute allergic reactions as well as long-term complications caused by the generation of powerful oxidant species, initiation and propagation of lipid peroxidation Allergy is to related to dextran moiety Iron dextran is associated with higher incidence of Type I hypersensitivity than Iron sucrose Iron sucrose carries the lowest risk for hypersensitivity IV iron therapy is superior to oral iron supplementation in CKD Risk factors associated with IV iron therapy include acute allergic reactions as well as long-term complications caused by the generation of powerful oxidant species, initiation and propagation of lipid peroxidation Allergy is to relate to dextran moiety Iron dextran is associated with higher incidence of Type I hypersensitivity than Iron sucrose Iron sucrose carries the lowest risk for hypersensitivity Ref: Horl WH. Iron therapy for renal anemia: how much needed, how much harmful? Pediatr Nephrol 2007;22:480–9. 1. Horl WH. Iron therapy for renal anemia: how much needed, how much harmful? Pediatr Nephrol 2007;22:480–9. 22

23
Iron sucrose in kidney disease
Iron deficiency may be corrected by oral iron supplementation but it is limited by – Poor compliance Adverse gastrointestinal reactions IV iron preparations commonly used include iron sucrose, sodium ferric gluconate, & iron dextran Iron sucrose is safer than iron dextran, is generally considered a safe and effective IV iron preparation in renal anemia Although iron deficiency may be corrected by oral iron supplementation in some patients, supplementation is often limited by poor compliance and adverse gastrointestinal reactions. Intravenous (IV) iron can reduce the occurrence of adverse gastrointestinal reactions and overcomes the problem of compliance with oral treatment. Intravenous iron preparations commonly used include iron sucrose, sodium ferric gluconate, and iron dextran. They are similar in the amount of iron they deliver and the degree to which they can improve anemia, but they have different safety profiles and adverse reaction risks. Iron sucrose is safer than iron dextran, is generally considered a safe and effective IV iron preparation. Iron sucrose has been in use for the last 50 years Ref – 1. Li H. Intravenous iron sucrose in peritoneal dialysis patients with renal anemia. Peritoneal Dialysis International 2008;28:149–54. 1. Li H. Intravenous iron sucrose in peritoneal dialysis patients with renal anemia. Peritoneal Dialysis International 2008;28:149–54. 23
 iron can reduce the occurrence of adverse gastrointestinal reactions and overcomes the problem of compliance with oral treatment. Intravenous iron preparations commonly used include iron sucrose, sodium ferric gluconate, and iron dextran. They are similar in the amount of iron they deliver and the degree to which they can improve anemia, but they have different safety profiles and adverse reaction risks. Iron sucrose. is safer than iron dextran, is generally considered a safe and effective IV iron preparation. Iron sucrose has been in use for the last 50 years. Ref – 1. Li H. Intravenous iron sucrose in peritoneal dialysis patients with renal anemia. Peritoneal Dialysis International 2008;28:149– Li H. Intravenous iron sucrose in peritoneal dialysis patients with renal anemia. Peritoneal Dialysis International 2008;28:149–")
24
Iron sucrose in kidney disease
Iron sucrose is a novel and effective addition in the management of ‘Anemia related to kidney diseases’ Iron Sucrose is elemental iron which replenishes body iron stores in patients with iron deficiency Approximately 25% of hemodialysis patients can be maintained on oral iron supplementation; the others require IV iron supplementation Iron sucrose injection is a mineral iron which plays a crucial role for the transport of oxygen in the blood, being a central atom of ‘heme group’ in red blood corpuscles(RBC) Iron sucrose injection is indicated for the treatment of iron deficiency anemia in patients undergoing chronic hemodialysis who are receiving supplemental erythropoetin (EPO) therapy. Adequate iron stores are essential for achieving maximum benefit from erythropoietic agents. Iron deficiency is the most common cause of diminished response with EPO in renal failure patients. Approximately 150mg iron is required for each 1 g/dl increase in haemoglobin concentration. A typical correction of 3–4 g/dl requires 450–600mg of iron Ref: Dennis J. Cada. Iron Sucrose Injection. Drug Reviews From The Formulary, Volume 36, April 2001, W.H. Horl, OPTA-therapy with iron and erythropoiesis-stimulating agents in chronic kidney disease, nephrology dial transplant suppl 3;iii2-iii6 1. Dennis J. Cada. Iron Sucrose Injection. Drug Reviews From The Formulary, Volume 36, April 2001, 2. W.H. Horl, OPTA-therapy with iron and erythropoiesis-stimulating agents in chronic kidney disease, nephrology dial transplant suppl 3;iii2-iii6 24
 Iron sucrose injection is indicated for the treatment of iron deficiency anemia in patients undergoing chronic hemodialysis who are receiving supplemental erythropoetin (EPO) therapy. Adequate iron stores are essential for achieving maximum benefit from erythropoietic agents. Iron deficiency is the most common cause of diminished response with EPO in renal failure patients. Approximately 150mg iron is required for each 1 g/dl increase in haemoglobin concentration. A typical correction of 3–4 g/dl requires 450–600mg of iron. Ref: Dennis J. Cada. Iron Sucrose Injection. Drug Reviews From The Formulary, Volume 36, April 2001, W.H. Horl, OPTA-therapy with iron and erythropoiesis-stimulating agents in chronic kidney disease, nephrology dial transplant suppl 3;iii2-iii6. 1. Dennis J. Cada. Iron Sucrose Injection. Drug Reviews From The Formulary, Volume 36, April 2001, W.H. Horl, OPTA-therapy with iron and erythropoiesis-stimulating agents in chronic kidney disease, nephrology dial transplant suppl 3;iii2-iii")
25
Indications IV iron sucrose is indicated in –
Non-Dialysis Dependent - Chronic Kidney Disease (NDD-CKD) patients receiving an erythropoietin Non-Dialysis Dependent - Chronic Kidney Disease (NDD-CKD) patients not receiving an erythropoietin Hemodialysis Dependent - Chronic Kidney Disease (HDD-CKD) patients receiving an erythropoietin Peritoneal Dialysis Dependent - Chronic Kidney Disease (PDD-CKD) patients receiving an erythropoietin IV iron sucrose is indicated in – 1. Non-Dialysis Dependent - Chronic Kidney Disease (NDD-CKD) patients receiving an erythropoietin 2. Non-Dialysis Dependent - Chronic Kidney Disease (NDD-CKD) patients not receiving an erythropoietin 3. Hemodialysis Dependent - Chronic Kidney Disease (HDD-CKD) patients receiving an erythropoietin 4. Peritoneal Dialysis Dependent - Chronic Kidney Disease (PDD-CKD) patients receiving an erythropoietin Iron sucrose is approved for use in iron deficiency anemia in hemodialysis patients as has recently received Food and Drug Administration (FDA)-approved labeling for the treatment of iron deficiency anemia in NDDCKD patients also. IV iron supplementation is an effective and safe treatment for anemia in predialysis CRF patients as shown in efficacy and safety studies. Ref – 1. Venofer® [package insert]. Shirley, NY: American Regent, Inc.; 2007. 2. Hollands JM et al. Safety of High-Dose Iron Sucrose Infusion in Hospitalized Patients With Chronic Kidney Disease. Am J Health-Syst Pharm. 2006;63(8): 3. Mircescu G et al. Intravenous iron supplementation for the treatment of anaemia in pre-dialyzed chronic renal failure patients. Nephrol Dial Transplant 2006;21:120-4. 1. Venofer® [package insert]. Shirley, NY: American Regent, Inc.; 2007. 2. Hollands JM et al. Safety of High-Dose Iron Sucrose Infusion in Hospitalized Patients With Chronic Kidney Disease. Am J Health-Syst Pharm. 2006;63(8): 3. Mircescu G et al. Intravenous iron supplementation for the treatment of anaemia in pre-dialyzed chronic renal failure patients. Nephrol Dial Transplant 2006;21:120-4. 25
 patients receiving an erythropoietin. Non-Dialysis Dependent - Chronic Kidney Disease (NDD-CKD) patients not receiving an erythropoietin. Hemodialysis Dependent - Chronic Kidney Disease (HDD-CKD) patients receiving an erythropoietin. Peritoneal Dialysis Dependent - Chronic Kidney Disease (PDD-CKD) patients receiving an erythropoietin. IV iron sucrose is indicated in – 1. Non-Dialysis Dependent - Chronic Kidney Disease (NDD-CKD) patients receiving an erythropoietin. 2. Non-Dialysis Dependent - Chronic Kidney Disease (NDD-CKD) patients not receiving an erythropoietin. 3. Hemodialysis Dependent - Chronic Kidney Disease (HDD-CKD) patients receiving an erythropoietin. 4. Peritoneal Dialysis Dependent - Chronic Kidney Disease (PDD-CKD) patients receiving an erythropoietin. Iron sucrose is approved for use in iron deficiency anemia in hemodialysis patients as has recently received Food and Drug Administration (FDA)-approved labeling for the treatment of iron deficiency anemia in NDDCKD patients also. IV iron supplementation is an effective and safe treatment for anemia in predialysis CRF patients as shown in efficacy and safety studies. Ref – 1. Venofer® [package insert]. Shirley, NY: American Regent, Inc.; Hollands JM et al. Safety of High-Dose Iron Sucrose Infusion in Hospitalized Patients With Chronic Kidney Disease. Am J Health-Syst Pharm. 2006;63(8): Mircescu G et al. Intravenous iron supplementation for the treatment of anaemia in pre-dialyzed chronic renal failure patients. Nephrol Dial Transplant 2006;21: Venofer® [package insert]. Shirley, NY: American Regent, Inc.; Hollands JM et al. Safety of High-Dose Iron Sucrose Infusion in Hospitalized Patients With Chronic Kidney Disease. Am J Health-Syst Pharm. 2006;63(8): Mircescu G et al. Intravenous iron supplementation for the treatment of anaemia in pre-dialyzed chronic renal failure patients. Nephrol Dial Transplant 2006;21:")
26
Iron sucrose in pre-dialysis CRF patients
Patients undergoing chronic hemodialysis often present with anemia IV iron therapy is administered in conjunction with EPO as it helps prevent EPO-hypo-responsiveness Study evaluated use of Iron sucrose in pre dialyzed patients of CRF 60 non-diabetic CRF patients were included in the study Patients undergoing chronic hemodialysis (HD) often present with anemia. Intravenous (IV) iron therapy is administered to these patients as part of anemia management therapy, often in conjunction with erythropoietin (EPO). IV iron is used as an adjuvant therapy to EPO as it helps prevent EPO-hyporesponsiveness. 89% of patients starting renal replacement therapy in Romania have Hb < 10 g/dL. Causes of iron deficiency in predialysis patients include reduced iron intake, reduced gastrointestinal iron absorption, GI bleeding, urinary loss of iron and reduced hemapoietic utilization of oral iron. Unlike oral iron, IV iron bypasses the gastrointestinal tract and is therefore immediately available for erythropoiesis in the bone marrow and more rapidly converted into Hb. Studies show that not only does IV iron increase response to EPO, but that IV iron alone can correct anemia in patients with CRF, this allows for important cost savings. In this study Mircescu et al. evaluated the effect of IV iron supplementation in 60 non-diabetic predialysis CRF patients without absolute iron deficiency and not receiving EPO. Ref: Mircescu G et al. Intravenous iron supplementation for the treatment of anaemia in pre-dialyzed chronic renal failure patients. Nephrol Dial Transplant 2006;21:120-4. Mircescu G ,et al. Intravenous iron supplementation for the treatment of anaemia in pre-dialyzed chronic renal failure patients. Nephrol Dial Transplant 2006;21:120-4. 26
 often present with anemia. Intravenous (IV) iron therapy is administered to these patients as part of anemia management therapy, often in conjunction with erythropoietin (EPO). IV iron is used as an adjuvant therapy to EPO as it helps prevent EPO-hyporesponsiveness. 89% of patients starting renal replacement therapy in Romania have Hb < 10 g/dL. Causes of iron deficiency in predialysis patients include reduced iron intake, reduced gastrointestinal iron absorption, GI bleeding, urinary loss of iron and reduced hemapoietic utilization of oral iron. Unlike oral iron, IV iron bypasses the gastrointestinal tract and is therefore immediately available for erythropoiesis in the bone marrow and more rapidly converted into Hb. Studies show that not only does IV iron increase response to EPO, but that IV iron alone can correct anemia in patients with CRF, this allows for important cost savings. In this study Mircescu et al. evaluated the effect of IV iron supplementation in 60 non-diabetic predialysis CRF patients without absolute iron deficiency and not receiving EPO. Ref: Mircescu G et al. Intravenous iron supplementation for the treatment of anaemia in pre-dialyzed chronic renal failure patients. Nephrol Dial Transplant 2006;21: Mircescu G ,et al. Intravenous iron supplementation for the treatment of anaemia in pre-dialyzed chronic renal failure patients. Nephrol Dial Transplant 2006;21:")
27
Results 60 patients included in the study
58% of patients reporting a rise in Hb > 1 g/dL vs. baseline in the study 80% of patients had a Hb > 10 g/dL vs. 44% at baseline 55% had a Hb > 11 g/dL vs. 0% at baseline Mean serum iron concentration increased from – 73.9 µg/dL at baseline 84.2 µg/dL at 6 months 101.8 µg/dL at 12 months of therapy No worsening of renal function, and no adverse events were reported 89% of patients starting renal replacement therapy have Hb < 10 g/dL. IV iron sucrose alone (200 mg per month) results in a significant hematological response in predialysis CRF patients, with a mean increase in Hb of 1.6 g/dL (from 9.7 ± 1.1 at the baseline to ±2.5 g/dL after 12 months of treatment; p < 0.05). IV iron sucrose alone (200 mg per month) enabled 55% of patients to attain a Hb > 11 g/dL, with 36% of patients with Hb < 10g/dL at baseline reaching Hb > 10 g/dL after 12 months thus 80% achieving Hb > 10 g/dL. No worsening of renal function, and no adverse events were reported. Ref: Mircescu G et al. Intravenous iron supplementation for the treatment of anaemia in pre-dialyzed chronic renal failure patients. Nephrol Dial Transplant 2006;21:120-4. Mircescu G et al. Intravenous iron supplementation for the treatment of anaemia in pre-dialyzed chronic renal failure patients. Nephrol Dial Transplant 2006;21:120-4. 27
 results in a significant hematological response in predialysis CRF patients, with a mean increase in Hb of 1.6 g/dL (from 9.7 ± 1.1 at the baseline to 11.3 ±2.5 g/dL after 12 months of treatment; p < 0.05). IV iron sucrose alone (200 mg per month) enabled 55% of patients to attain a Hb > 11 g/dL, with 36% of patients with Hb < 10g/dL at baseline reaching Hb > 10 g/dL after 12 months thus 80% achieving Hb > 10 g/dL. No worsening of renal function, and no adverse events were reported. Ref: Mircescu G et al. Intravenous iron supplementation for the treatment of anaemia in pre-dialyzed chronic renal failure patients. Nephrol Dial Transplant 2006;21: Mircescu G et al. Intravenous iron supplementation for the treatment of anaemia in pre-dialyzed chronic renal failure patients. Nephrol Dial Transplant 2006;21:")
28
Efficacy of Iron sucrose in hemodialysis patients
Schiesser et al conducted a prospective multicentre clinical trial in 50 iron-replete hemodialysis patients to evaluate the efficacy of iron sucrose administration for 6 months Hb level remained stable (12±1.1 at baseline & 12.1±1.5 g/dl at the end of the study) Reduced dose for EPO Schiesser et al conducted a prospective multicentre clinical trial in iron-replete hemodialysis patients to evaluate the efficacy of weekly low-dose (50 mg) intravenous iron sucrose administration for 6 months to maintain the iron status. Forty-two patients (84%) completed the study. After 6 months of intravenous iron sucrose treatment, the mean ferritin value showed a tendency to increase slightly from 405±59 at baseline to 490±275 mg/l at the end of the study, but iron, transferrin levels and transferrin saturation did not change. The haemoglobin level remained stable (12±1.1 at baseline and 12.1±1.5 g/dl at the end of the study). The mean dose of darbepoetin alfa could be reduced from 0.75 to 0.46 mg/kg/week; epoetin alfa was decreased from 101 to 74 IU/kg/week; and the mean dose of epoetin beta could be reduced from 148 to 131 IU/kg/week at the end of treatment. It was concluded that a regular 50 mg weekly dosing schedule of iron sucrose maintains stable iron stores and hemoglobin levels in hemodialysed patients and allows considerable dose reductions for epoetins. Low-dose intravenous iron therapy may represent an optimal approach to treat the continuous loss of iron in dialysis patients Ref: Schiesser et al. Weekly low-dose treatment with intravenous iron sucrose maintains iron status and decreases epoetin requirement in iron-replete haemodialysis patients. Nephrol Dial Transplant (2006) 21: 2841–2845. Schiesser et al. Weekly low-dose treatment with intravenous iron sucrose maintains iron status and decreases epoetin requirement in iron-replete haemodialysis patients. Nephrol Dial Transplant (2006) 21: 2841–5. 28
 Reduced dose for EPO. Schiesser et al conducted a prospective multicentre clinical trial in iron-replete hemodialysis patients to evaluate the efficacy of weekly low-dose (50 mg) intravenous iron sucrose administration for 6 months to maintain the iron status. Forty-two patients (84%) completed the study. After 6 months of intravenous iron sucrose treatment, the mean ferritin value showed a tendency. to increase slightly from 405±59 at baseline to 490±275 mg/l at the end of the study, but iron, transferrin levels and transferrin saturation did not. change. The haemoglobin level remained stable (12±1.1 at baseline and 12.1±1.5 g/dl at the end of the study). The mean dose of darbepoetin alfa could be reduced from 0.75 to 0.46 mg/kg/week; epoetin alfa was decreased from 101 to 74 IU/kg/week; and the mean dose of epoetin beta could be reduced from 148 to 131 IU/kg/week at the end of treatment. It was concluded that a regular 50 mg weekly dosing schedule of iron sucrose maintains stable iron stores and hemoglobin levels in hemodialysed patients and allows considerable dose reductions for epoetins. Low-dose intravenous iron therapy may represent an optimal approach to treat the continuous loss of iron in dialysis patients. Ref: Schiesser et al. Weekly low-dose treatment with intravenous iron sucrose maintains iron status and decreases epoetin requirement in iron-replete. haemodialysis patients. Nephrol Dial Transplant (2006) 21: 2841–2845. Schiesser et al. Weekly low-dose treatment with intravenous iron sucrose maintains iron status and decreases epoetin requirement in iron-replete haemodialysis patients. Nephrol Dial Transplant (2006) 21: 2841–")
29
Results of Schiesser et al study
Hb level remained stable (12±1.1 at baseline & 12.1±1.5 g/dl at the end of the study) Red cell parameters remained stable The mean haemoglobin values did not change from the baseline screening period to the end of the study. The mean haemoglobin of 12.1 g/dl demonstrates that the patients were in the target range, as defined by the EBPG and K/DOQI guidelines. Red cell indices. MCV, MCH and MCHC were in the normal range during the entire study and did not change significantly. Schiesser et al. Weekly low-dose treatment with intravenous iron sucrose maintains iron status and decreases epoetin requirement in iron-replete haemodialysis patients. Nephrol Dial Transplant (2006) 21: 2841–5. 29
 Red cell parameters remained stable. The mean haemoglobin values did not change from the baseline screening period to the end of the study. The mean haemoglobin of 12.1 g/dl demonstrates that the patients were in the target range, as defined by the EBPG and K/DOQI guidelines. Red cell indices. MCV, MCH and. MCHC were in the normal range during the entire study and did not change significantly. Schiesser et al. Weekly low-dose treatment with intravenous iron sucrose maintains iron status and decreases epoetin requirement in iron-replete. haemodialysis patients. Nephrol Dial Transplant (2006) 21: 2841–")
30
Iron sucrose IV reduces EPO demand in dialysis patients
In the study of Iron sucrose in hemodialysis patients conducted by Schiesser et al the dosage for the three different epoetins decreased by – 38.5% with darbepoetin alfa 6.3% with epoetin alfa 8.3% with epoetin beta In the study of Iron sucrose in hemodialysis patients conducted by Schiesser et al the dosage for the three different epoetins decreased by – % with darbepoetin alfa 2. 6.3% with epoetin alfa 3. 8.3% with epoetin beta Ref: Schiesser et al. Weekly low-dose treatment with intravenous iron sucrose maintains iron status and decreases epoetin requirement in iron-replete haemodialysis patients. Nephrol Dial Transplant (2006) 21: 2841–2845. Schiesser et al. Weekly low-dose treatment with intravenous iron sucrose maintains iron status and decreases epoetin requirement in iron-replete haemodialysis patients. Nephrol Dial Transplant (2006) 21: 2841–5. 30
 21: 2841–2845. Schiesser et al. Weekly low-dose treatment with intravenous iron sucrose maintains iron status and decreases epoetin requirement in iron-replete haemodialysis patients. Nephrol Dial Transplant (2006) 21: 2841–")
31
Results showing reduced EPO need with iron sucrose
Schiesser et al showed reduced EPO need with low dose maintenance iron sucrose in their study The mean dose of darbepoetin alfa was reduced with the iron treatment from 0.75 to 0.46 mg/kg/week (38.7%). The mean dose of epoetin alfa was decreased from 101 to 74 IU/kg/week (26.7%). For epoetin beta, the mean dose could be reduced from 148 to 131 IU/kg/week (11.5%) at the end of treatment. Schiesser et al. Weekly low-dose treatment with intravenous iron sucrose maintains iron status and decreases epoetin requirement in iron-replete haemodialysis patients. Nephrol Dial Transplant (2006) 21: 2841–5. 31
. The mean dose of epoetin alfa was decreased from 101 to 74 IU/kg/week (26.7%). For epoetin beta, the mean dose could be reduced from 148 to 131 IU/kg/week (11.5%) at the end of treatment. Schiesser et al. Weekly low-dose treatment with intravenous iron sucrose maintains iron status and decreases epoetin requirement in iron-replete. haemodialysis patients. Nephrol Dial Transplant (2006) 21: 2841–")
32
IV iron reduces EPO demand in dialysis patients
Chang et al studies the beneficial effects of 2 weekly IV iron supplementation compared to once monthly IV iron in 149 iron replete patients EPO requirement reduced by 25% when sereum ferritin & Transferrin saturation was maintained at high levels by administering 2 weekly IV iron compared to IV iron given once monthly Significant decrease in serum albumin, cholesterol & pre-dialysis creatinine when IV iron was administered 2 weekly for 1 year Chang et al conducted a 12-month IV iron substitution trial in 149 iron-replete chronic HD patients receiving s.c. rHuEPO therapy. The available iron pool was maintained with 100 mg iron every 2 weeks or 1 month depending on serum ferritin and transferrin saturation levels, the rHuEPO dosage titrated depending on hematocrit (Hct) levels. After 12-month protocol - - The Hct increased (28.7 +/- 4.1 vs /- 2.6, p = 0.003) - rHuEPO requirement reduced by 25% (46.1 +/ vs / U/kg/week, p = 0.006) - Serum ferritin increased (1,383 +/- 727 vs 930 +/- 857 ng/ml, p < 0.001) - Transferrin saturation increased (36.1 +/ vs /- 12.8%, p < 0.001) - The serum albumin decreased slightly but reached statistical significance (4.1 +/ vs 4.2 +/ g/dl, p = 0.006) - The cholesterol levels decreased (166 +/- 41 vs 173 +/- 38 mg/dl, p = 0.044) - The pre-dialysis creatinine levels decreased (11.3 +/- 2.3 vs /- 2.4 mg/dl, p = 0.015) The authors concluded that maintaining high levels of serum ferritin and transferrin saturation could further reduce the requirement of rHuEPO in chronic HD patients Ref: Chang CH et al. Reduction in erythropoietin doses by the use of chronic intravenous iron supplementation in iron-replete hemodialysis patients. Clin Nephrol. 2002;57: Chang CH et al. Reduction in erythropoietin doses by the use of chronic intravenous iron supplementation in iron-replete hemodialysis patients. Clin Nephrol. 2002;57: 32
 levels. After 12-month protocol - - The Hct increased (28.7 +/- 4.1 vs /- 2.6, p = 0.003) - rHuEPO requirement reduced by 25% (46.1 +/ vs / U/kg/week, p = 0.006) - Serum ferritin increased (1,383 +/- 727 vs 930 +/- 857 ng/ml, p < 0.001) - Transferrin saturation increased (36.1 +/ vs /- 12.8%, p < 0.001) - The serum albumin decreased slightly but reached statistical significance (4.1 +/ vs 4.2 +/ g/dl, p = 0.006) - The cholesterol levels decreased (166 +/- 41 vs 173 +/- 38 mg/dl, p = 0.044) - The pre-dialysis creatinine levels decreased (11.3 +/- 2.3 vs /- 2.4 mg/dl, p = 0.015) The authors concluded that maintaining high levels of serum ferritin and transferrin saturation could further reduce the requirement of rHuEPO in chronic HD patients. Ref: Chang CH et al. Reduction in erythropoietin doses by the use of chronic intravenous iron supplementation in iron-replete hemodialysis patients. Clin Nephrol. 2002;57: Chang CH et al. Reduction in erythropoietin doses by the use of chronic intravenous iron supplementation in iron-replete hemodialysis patients. Clin Nephrol. 2002;57:")
33
IV iron reduces EPO demand in dialysis patients – Results from Meta analysis
Compared to oral iron IV iron preparations significantly reduce the EPO requirement in dialysis patients A 2008 Meta analysis reviewed the efficacy of oral versus IV iron preparations in dialysis patients. Mean end EPO dose or change in EPO dose from baseline at 2 to 3 months was reported in 5 trials studied in the meta analysis. EPO dose (reported as unit per kilogram per week) decreased significantly in the IV iron – treated patients (WMD, U/kg/wk; 95% CI,42.12 to14.3; 5 trials) without significant heterogeneity (P 0.1; I %) Ref: Rozen-Zvi et al. Intravenous Versus Oral Iron Supplementation for the Treatment of Anemia in CKD: Systematic Review and Meta-analysis. American Journal of Kidney Diseases 2008;52: Rozen-Zvi et al. Intravenous Versus Oral Iron Supplementation for the Treatment of Anemia in CKD: Systematic Review and Meta-analysis. American Journal of Kidney Diseases 2008;52: 33
 decreased significantly in the IV iron – treated patients (WMD, U/kg/wk; 95% CI,42.12 to14.3; 5 trials) without significant heterogeneity (P 0.1; I2 44.1%) Ref: Rozen-Zvi et al. Intravenous Versus Oral Iron Supplementation for the Treatment of Anemia in CKD: Systematic Review and Meta-analysis. American Journal of Kidney Diseases 2008;52: Rozen-Zvi et al. Intravenous Versus Oral Iron Supplementation for the Treatment of Anemia in CKD: Systematic Review and Meta-analysis. American Journal of Kidney Diseases 2008;52:")
34
Iron sucrose in CKD patients not on dialysis
Charytan et al compared oral iron with Iron sucrose in 96 NDD-CKD patients More IV iron patients (54.2%) attained hemoglobin values > 11.0 g/dl compared to oral iron patients (31.3%) There were no serious side effects with iron sucrose Charytan et al compared oral iron with Iron sucrose in 96 NDD-CKD patients. More IV iron patients (54.2%) attained hemoglobin values > 11.0 g/dl compared to oral iron patients (31.3%). IV iron patients had greater increases in mean serum ferritin (288 ng/ml, p < ) compared to oral iron patients (-5.1 ng/ml, p = NS). IV iron patients with baseline ferritin < 100 ng/ml had a greater increase in hemoglobin (1.4 g/dl) compared to oral iron patients (0.9 g/dl) (p < 0.05). There were no serious side effects Authors concluded that CKD patients had increases in both hemoglobin and ferritin following IV iron therapy, whereas those treated with oral iron had increases in hemoglobin without increases in iron stores. Iron sucrose, given weekly as 200 mg IV push over 5 min is an effective and safe anemia treatment in this population. Ref: Charytan C et al. Comparison of intravenous iron sucrose to oral iron in the treatment of anemic patients with chronic kidney disease not on dialysis. Nephron Clin Pract. 2005;100(3):c55-62. Charytan C et al. Comparison of intravenous iron sucrose to oral iron in the treatment of anemic patients with chronic kidney disease not on dialysis. Nephron Clin Pract. 2005;100(3):c55-62. 34
 attained hemoglobin values > 11.0 g/dl compared to oral iron patients (31.3%) There were no serious side effects with iron sucrose. Charytan et al compared oral iron with Iron sucrose in 96 NDD-CKD patients. More IV iron patients (54.2%) attained hemoglobin values > 11.0 g/dl compared to oral iron patients (31.3%). IV iron patients had greater increases in mean serum ferritin (288 ng/ml, p < ) compared to oral iron patients (-5.1 ng/ml, p = NS). IV iron patients with baseline ferritin < 100 ng/ml had a greater increase in hemoglobin (1.4 g/dl) compared to oral iron patients (0.9 g/dl) (p < 0.05). There were no serious side effects. Authors concluded that CKD patients had increases in both hemoglobin and ferritin following IV iron therapy, whereas those treated with oral iron had increases in hemoglobin without increases in iron stores. Iron sucrose, given weekly as 200 mg IV push over 5 min is an effective and safe anemia treatment in this population. Ref: Charytan C et al. Comparison of intravenous iron sucrose to oral iron in the treatment of anemic patients with chronic kidney disease not on dialysis. Nephron Clin Pract. 2005;100(3):c Charytan C et al. Comparison of intravenous iron sucrose to oral iron in the treatment of anemic patients with chronic kidney disease not on dialysis. Nephron Clin Pract. 2005;100(3):c")
35
Efficacy & safety of Iron sucrose in peritoneal dialysis patients
Li et al conducted a study to compare the clinical outcomes & safety of IV iron sucrose & oral ferrous succinate in combination with rHuEPO therapy in patients on maintenance PD 46 patients were included – 26 received iron sucrose & 20 oral iron Hb & Hct increased significantly at 2 weeks in the IV group compared with baseline The total response rate at 8 weeks was 94.8% for the IV group - significantly higher than that of the oral group (55.0%) There were no adverse events with IV iron 8 patients in the oral group had adverse GI effects Li et al conducted a randomized, controlled, parallel-group single center trial to explore the safety and efficacy of intravenous (IV) iron sucrose in maintenance peritoneal dialysis (PD). 46 patients on PD were involved in this trial. 26 patients received IV iron sucrose (200 mg iron) once per week for 4 weeks then once every other week for a further 4 weeks. The other 20 patients received oral ferrous succinate, 200 mg three times per day, for 8 weeks. Hemoglobin, hematocrit, serum ferritin (SF) level, and transferrin saturation (TSAT) were assessed at baseline and then again after 2, 4, and 8 weeks of treatment. Results - There were no differences between the IV and oral groups in terms of sex, age, duration of PD, mean dialysate dosage per day, erythropoietin dosage per week, or hematological parameters at baseline. After 4 and 8 weeks of treatment, mean Hb and Hct were significantly increased in the IV group and were also significantly higher than those in the oral group. Levels of SF and TSAT were also significantly increased in the IV group, and significantly higher than in the oral group. After 8 weeks, the response rate in the IV group was 94.8%, which was significantly higher than that in the oral group. The mean erythropoietin dose was significantly lower in the IV group than in the oral group. There were no adverse events with IV iron. Eight patients in the oral group had adverse gastrointestinal effects. It was concluded that IV iron sucrose is safe in PD patients. It increases Hb levels and serum iron parameters more effectively than oral iron; it is well tolerated and can permit reductions in the required dose of erythropoietin. Ref: Li H. Intravenous iron sucrose in peritoneal dialysis patients with renal anemia. Peritoneal Dialysis International 2008;28:149–54. Li H. Intravenous iron sucrose in peritoneal dialysis patients with renal anemia. Peritoneal Dialysis International 2008;28:149–54. 35
 There were no adverse events with IV iron. 8 patients in the oral group had adverse GI effects. Li et al conducted a randomized, controlled, parallel-group single center trial to explore the safety and efficacy of intravenous (IV) iron sucrose in maintenance peritoneal dialysis (PD). 46 patients on PD were involved in this trial. 26 patients received IV iron sucrose (200 mg iron) once per week for 4 weeks then once every other week for a further 4 weeks. The other 20 patients received oral ferrous succinate, 200 mg three times per day, for 8 weeks. Hemoglobin, hematocrit, serum ferritin (SF) level, and transferrin saturation (TSAT) were assessed at baseline and then again after 2, 4, and 8 weeks of treatment. Results - There were no differences between the IV and oral groups in terms of sex, age, duration of PD, mean dialysate dosage per day, erythropoietin dosage per week, or hematological parameters at baseline. After 4 and 8 weeks of treatment, mean Hb and Hct were significantly increased in the. IV group and were also significantly higher than those in the oral group. Levels of SF and TSAT were also significantly increased in the IV group, and significantly higher than in the oral group. After 8 weeks, the response rate in the IV group was 94.8%, which was significantly higher than that in the oral group. The mean erythropoietin dose was significantly lower in the IV group than in the oral group. There were no adverse events with IV iron. Eight patients in the oral group had adverse gastrointestinal effects. It was concluded that IV iron sucrose is safe in PD patients. It increases Hb levels and serum iron parameters more effectively than oral iron; it is well tolerated and can permit reductions in the required dose of erythropoietin. Ref: Li H. Intravenous iron sucrose in peritoneal dialysis patients with renal anemia. Peritoneal Dialysis International 2008;28:149–54. Li H. Intravenous iron sucrose in peritoneal dialysis patients with renal anemia. Peritoneal Dialysis International 2008;28:149–")
36
Results of Iron sucrose in PD patients contd.
Response rates to IV iron sucrose therapy compared to Oral iron therapy Table shows response rates to IV iron sucrose therapy compared to Oral iron therapy. Ref: Li H. Intravenous iron sucrose in peritoneal dialysis patients with renal anemia. Peritoneal Dialysis International 2008;28:149–54. Li H. Intravenous iron sucrose in peritoneal dialysis patients with renal anemia. Peritoneal Dialysis International 2008;28:149–54. 36

37
Efficacy of Iron sucrose in ESRD
Iron sucrose in apparently iron-replete patients will decrease the EPO requirements for a given target hematocrit in patients on maintenance hemodialysis with end-stage renal disease (ESRD) Intravenous (IV) iron sucrose in apparently iron-replete patients will decrease the epoetin requirements for a given target haematocrit in patients on maintenance haemodialysis with end-stage renal disease (ESRD). Ref: Schiesser et al. Weekly low-dose treatment with intravenous iron sucrose maintains iron status and decreases epoetin requirement in iron-replete haemodialysis patients. Nephrol Dial Transplant (2006) 21: 2841–2845. Shaldon S. The use of IV iron in the treatment of anaemia of ESRD patients on maintenance haemodialysis: an historical and personal view. Nephrol Dial Transplant (2007) 22: 23–25. 1. Schiesser et al. Weekly low-dose treatment with intravenous iron sucrose maintains iron status and decreases epoetin requirement in iron-replete haemodialysis patients. Nephrol Dial Transplant (2006) 21: 2841–2845. 2. Shaldon S. The use of IV iron in the treatment of anaemia of ESRD patients on maintenance haemodialysis: an historical and personal view. Nephrol Dial Transplant (2007) 22: 23–25. 37
 Intravenous (IV) iron sucrose in apparently iron-replete patients will decrease the epoetin requirements for a given target haematocrit. in patients on maintenance haemodialysis with end-stage renal disease (ESRD). Ref: Schiesser et al. Weekly low-dose treatment with intravenous iron sucrose maintains iron status and decreases epoetin requirement in iron-replete haemodialysis patients. Nephrol Dial Transplant (2006) 21: 2841–2845. Shaldon S. The use of IV iron in the treatment of anaemia of ESRD patients on maintenance haemodialysis: an historical and personal view. Nephrol Dial Transplant (2007) 22: 23– Schiesser et al. Weekly low-dose treatment with intravenous iron sucrose maintains iron status and decreases epoetin requirement in iron-replete haemodialysis patients. Nephrol Dial Transplant (2006) 21: 2841– Shaldon S. The use of IV iron in the treatment of anaemia of ESRD patients on maintenance haemodialysis: an historical and personal view. Nephrol Dial Transplant (2007) 22: 23–")
38
Safety of Iron sucrose Aronoff et al studied the safety of iron sucrose in hemodialysis patients 665 hemodialysis patients with 80 who had experienced previous intolerance to other IV iron preparations were given iron sucrose There were no serious or life-threatening drug-related adverse events Serious adverse events have been reported after single doses of some intravenous iron products. This multicenter phase IV clinical trial examined the safety of iron sucrose for the treatment of iron deficiency and for the maintenance of iron sufficiency in hemodialysis patients. In this safety study, iron sucrose was given in two dosing regimens. Iron deficient patients were treated with intravenous iron sucrose, 100 mg, during 10 consecutive hemodialysis sessions (replacement regimen). Iron replete patients were given iron sucrose, 100 mg intravenous (iv) over 5 minutes, weekly for 10 weeks (maintenance regimen). At the end of each 10-dose cycle, iron status was reassessed, and dosing during the subsequent cycle was based on the adequacy of iron stores as per Dialysis Outcome Quality Initiative (K/DOQI) Guidelines. With each dosing regimen, adverse events, if any, were recorded and described. Six hundred and sixty-five hemodialysis patients, including 80 who had experienced previous intolerance to other parenteral iron preparations, received a total of 8583 doses of iron sucrose. One hundred eighty-eight patients received more than one iv iron cycle (replacement, maintenance, or both). There were no serious or life-threatening drug-related adverse events. It was concluded that Iron sucrose is safe when given as treatment for iron deficiency or for maintenance of iron stores in EPO-treated dialysis patients, including those sensitive to iron dextran, ferric gluconate, or both. Ref: Aronoff GR et al. Iron sucrose in hemodialysis patients: Safety of replacement and maintenance regimens. Kidney International, 2004;66:1193–8. Aronoff GR et al. Iron sucrose in hemodialysis patients: Safety of replacement and maintenance regimens. Kidney International, 2004;66:1193–8. 38
. Iron replete patients were given iron sucrose, 100 mg intravenous (iv) over 5 minutes, weekly for 10 weeks (maintenance regimen). At the end of each 10-dose cycle, iron status was reassessed, and dosing during the. subsequent cycle was based on the adequacy of iron stores as per Dialysis Outcome Quality Initiative (K/DOQI) Guidelines. With each dosing regimen, adverse events, if any, were recorded and described. Six hundred and sixty-five hemodialysis patients, including 80 who had experienced previous intolerance to other parenteral iron preparations, received a total of 8583 doses of iron sucrose. One hundred eighty-eight patients received more than one iv iron cycle (replacement, maintenance, or both). There were no serious or life-threatening drug-related adverse events. It was concluded that Iron sucrose is safe when given as treatment for iron deficiency or for maintenance of iron stores in EPO-treated dialysis patients, including those sensitive to iron dextran, ferric gluconate, or both. Ref: Aronoff GR et al. Iron sucrose in hemodialysis patients: Safety of replacement and maintenance regimens. Kidney International, 2004;66:1193–8. Aronoff GR et al. Iron sucrose in hemodialysis patients: Safety of replacement and maintenance regimens. Kidney International, 2004;66:1193–")
39
Iron sucrose in patients hypersensitive to iron dextran
Iron dextran has been the only available parenteral iron preparation for a long time Its use has been associated with increased risk of allergic reactions, even after reaction-free previous use Iron dextran has been the only available parenteral iron preparation for a long time Its use has been associated with increased risk of allergic reactions, even after reaction-free previous use Ref: Haddad A et al. Use of Iron Sucrose in Dialysis Patients Sensitive to Iron Dextran. Saudi J Kidney Dis Transpl 2009;20(2): Haddad A et al. Use of Iron Sucrose in Dialysis Patients Sensitive to Iron Dextran. Saudi J Kidney Dis Transpl 2009;20(2): 39
: Haddad A et al. Use of Iron Sucrose in Dialysis Patients Sensitive to Iron Dextran. Saudi J Kidney Dis Transpl 2009;20(2):")
40
Iron sucrose in patients hypersensitive to iron dextran
Of 205 patients of hemodialysis, 7.3% were hypersensitive Hypersensitive patients were given iron sucrose for 8 weeks None of them developed hypersensitivity Mean hematocrit increased from 23.8% to 32.27% Mean serum iron increased from 29.3 ng/dL to 76.8 ng/dL The patients hypersensitive to iron dextran were treated with iron sucrose (100 mg administered as an intravenous push over 5-10 minutes once a week) for 8 weeks. Complete blood count, serum iron, serum ferritin, and parathyroid hormone were measured at the beginning and at the end of the study (except parathyroid hormone). All patients received subcutaneous erythropoietin at a constant dose of 5000 IU twice weekly unless a change was required. All the patients completed the study period and none of them developed hypersensitivity reactions to iron sucrose. The mean hematocrit increased from 23.8% to 32.27% (p < ), the mean serum ferritin from 185 ng/mL to 599 ng/mL (p < ), and the mean serum iron from 29.3 ng/dL to 76.8 ng/dL (p = 0.01). Authors concluded that iron sucrose is safe and effective in HD patients with documented hypersensitivity reactions to low molecular weight iron dextran. Ref: Haddad A et al. Use of Iron Sucrose in Dialysis Patients Sensitive to Iron Dextran. Saudi J Kidney Dis Transpl 2009;20(2): Haddad A et al. Use of Iron Sucrose in Dialysis Patients Sensitive to Iron Dextran. Saudi J Kidney Dis Transpl 2009;20(2): 40
 for 8 weeks. Complete blood count, serum iron, serum ferritin, and parathyroid hormone were measured at the beginning and at the end of the study (except parathyroid hormone). All patients received subcutaneous erythropoietin at a constant dose of 5000 IU twice weekly unless a change was required. All the patients completed the study period and none of them developed hypersensitivity reactions to iron sucrose. The mean hematocrit increased from 23.8% to 32.27% (p < ), the mean serum ferritin from 185 ng/mL to 599 ng/mL (p < ), and the mean serum iron from 29.3 ng/dL to 76.8 ng/dL (p = 0.01). Authors concluded that iron sucrose is safe and effective in HD patients with documented hypersensitivity reactions to low molecular weight iron dextran. Ref: Haddad A et al. Use of Iron Sucrose in Dialysis Patients Sensitive to Iron Dextran. Saudi J Kidney Dis Transpl 2009;20(2): Haddad A et al. Use of Iron Sucrose in Dialysis Patients Sensitive to Iron Dextran. Saudi J Kidney Dis Transpl 2009;20(2):")
41
Safety of Iron sucrose compared to other iron preparations
Rates of life-threatening ADEs – 0.6 per million for iron sucrose 0.9 per million for sodium ferric gluconate complex 3.3 per million for lower molecular weight iron dextran 11.3 per million per million for higher molecular weight iron dextran Data from the United States Food and Drug Administration (FDA) on ADEs attributed to the provision of four formulations of intravenous iron during 2001–2003, including higher and lower molecular weight iron dextran, sodium ferric gluconate complex and iron sucrose was evaluated. The total number of reported parenteral iron related ADEs was 1141 among approximately doses administered, yielding a rate of 3.8x10-5, or roughly 38 per million. Rates of life-threatening ADEs – 0.6 per million for iron sucrose 0.9 per million for sodium ferric gluconate complex 3.3 per million for lower molecular weight iron dextran 11.3 per million per million for higher molecular weight iron dextran Ref: Chertow GM et al. Update on adverse drug events associated with parenteral iron. Nephrol Dial Transplant (2006) 21: 378–382. Chertow GM et al. Update on adverse drug events associated with parenteral iron. Nephrol Dial Transplant (2006) 21: 378–382. 41
 on ADEs attributed to the provision of four formulations of intravenous iron during 2001–2003, including higher and lower molecular weight iron dextran, sodium ferric gluconate complex and iron sucrose was evaluated. The total number of reported parenteral iron related ADEs was 1141 among approximately doses administered, yielding a rate of. 3.8x10-5, or roughly 38 per million. Rates of life-threatening ADEs – 0.6 per million for iron sucrose. 0.9 per million for sodium ferric gluconate complex. 3.3 per million for lower molecular weight iron dextran per million per million for higher molecular weight iron dextran. Ref: Chertow GM et al. Update on adverse drug events associated with parenteral iron. Nephrol Dial Transplant (2006) 21: 378–382. Chertow GM et al. Update on adverse drug events associated with parenteral iron. Nephrol Dial Transplant (2006) 21: 378–")
42
Dosing and administration
NDD-CKD - Administered as a total cumulative dose of 1,000 mg over a 14 days as a 200 mg slow IV injection undiluted over 2 to 5 minutes on 5 different occasions HDD-CKD - Administered undiluted as a 100 mg slow IV over 2 to 5 minutes or as an infusion of 100 mg, diluted in a maximum of 100 mL of NS over 15 minutes per consecutive hemodialysis session for a total cumulative dose of 1,000 mg Recommended dosing1 – NDD-CKD - Administered as a total cumulative dose of 1,000 mg over a 14 days as a 200 mg slow IV injection undiluted over 2 to 5 minutes on 5 different occasions HDD-CKD - Administered undiluted as a 100 mg slow IV over 2 to 5 minutes or as an infusion of 100 mg, diluted in a maximum of 100 mL of NS over 15 minutes per consecutive hemodialysis session for a total cumulative dose of 1,000 mg Ref: Venofer® [package insert]. Shirley, NY: American Regent, Inc.; 2007. 1. Venofer® [package insert]. Shirley, NY: American Regent, Inc.; 2007. 42

43
Dosing and administration contd.
PDD-CKD - Administered undiluted as a total cumulative dose of 1,000 mg in 3 divided doses, given by slow IV infusion, over 28 days: 2 infusions of 300 mg over 1.5 hs 14 days apart Followed by mg infusion over 2.5 h 14 days later Should be diluted in 250 mL of NS Low maintenance doses in hemodialysis patients include 50mg injected into the venous limb of the haemodialysis tubing system (slow intravenous push at a rate of 10 mg/min) PDD-CKD1 - Administered undiluted as a total cumulative dose of 1,000 mg in 3 divided doses, given by slow intravenous infusion, within a 28 day period: 2 infusions of 300 mg over 1.5 hours 14 days apart followed by one 400 mg infusion over 2.5 hours 14 days later. Should be diluted in a maximum of 250 mL of NS Low maintenance doses in hemodialysis patients include 50mg injected into the venous limb of the haemodialysis tubing system (slow intravenous push at a rate of 10 mg/min)2 High dose iron sucrose included the drug containing elemental iron 300 mg diluted in mL of NS, infused over 1-2 hours3 Ref: Venofer® [package insert]. Shirley, NY: American Regent, Inc.; 2007. Schiesser et al. Weekly low-dose treatment with intravenous iron sucrose maintains iron status and decreases epoetin requirement in iron-replete haemodialysis patients. Nephrol Dial Transplant (2006) 21: 2841–2845. Hollands JM et al. Safety of High-Dose Iron Sucrose Infusion in Hospitalized Patients With Chronic Kidney Disease. Am J Health-Syst Pharm. 2006;63(8): 1. Venofer® [package insert]. Shirley, NY: American Regent, Inc.; 2007. 43
 PDD-CKD1 - Administered undiluted as a total cumulative dose of 1,000 mg in 3 divided doses, given by slow intravenous infusion, within a 28 day period: 2 infusions of 300 mg over 1.5 hours 14 days apart followed by one 400 mg infusion over 2.5 hours 14 days later. Should be diluted in a maximum of 250 mL of NS. Low maintenance doses in hemodialysis patients include 50mg injected into the venous limb of the haemodialysis tubing system (slow intravenous push at a rate of 10 mg/min)2. High dose iron sucrose included the drug containing elemental iron 300 mg diluted in mL of NS, infused over 1-2 hours3. Ref: Venofer® [package insert]. Shirley, NY: American Regent, Inc.; Schiesser et al. Weekly low-dose treatment with intravenous iron sucrose maintains iron status and decreases epoetin requirement in iron-replete haemodialysis patients. Nephrol Dial Transplant (2006) 21: 2841–2845. Hollands JM et al. Safety of High-Dose Iron Sucrose Infusion in Hospitalized Patients With Chronic Kidney Disease. Am J Health-Syst Pharm. 2006;63(8): Venofer® [package insert]. Shirley, NY: American Regent, Inc.;")
44
Dosing and administration contd.
The usual dose is 100 mg administered one to three times per week. Most patients will require a minimum cumulative dose of 1000 mg of elemental iron administered over 10 sequential dialysis sessions to achieve a favorable response Patients may continue to receive IV iron therapy at the lowest dose necessary to maintain target levels of hemoglobin, hematocrit & iron storage parameters The usual dose is 100 mg administered one to three times per week. It should not be administered more than three times weekly. Most patients will require a minimum cumulative dose of 1000 mg of elemental iron administered over 10 sequential dialysis sessions to achieve a favorable response. Patients may continue to receive IV iron therapy at the lowest dose necessary to maintain target levels of hemoglobin, hematocrit, and iron storage parameters. Ref: Cada DJ. Iron Sucrose Injection. Hospital Pharmacy 2001;36:404–12. Cada DJ. Iron Sucrose Injection. Hospital Pharmacy 2001;36:404–12. 44

45
Monitoring parameters
Patients receiving regular IV iron therapy require monitoring of hematologic parameters & iron indices (Hb, Hct, TSAT, & ferritin) Maintain TSAT between 20% and 50% Iron therapy should be withheld in patients with TSAT ≥50% Iron therapy should be withheld in patients with ferritin values ≥800 ng/mL Since transferrin saturation values increase rapidly after IV administration of iron sucrose, serum iron values may be reliably obtained 48 hours after IV iron sucrose dosing Hemoglobin, hematocrit, and iron status should be monitored periodically in patients receiving iron sucrose therapy. Iron status in patients receiving epoetin alfa should be monitored by the percent transferrin saturation (TSAT) and the serum ferritin level. In patients receiving epoetin alfa, iron supplementation should be administered to maintain serum ferritin at > 100 mcg/L but not exceeding 800 mcg/L and transferrin saturation at > 20% but not exceeding 50%. Hypochromic red blood cells should be maintained at less than 10%. Iron status should be monitored monthly initially, then every 2 to 3 months. Because transferrin saturation increases rapidly after the IV administration of iron sucrose, reliable serum iron values can be obtained 48 hours after administration. Iron therapy should be withheld in patients with evidence of iron overload. Ref: Cada DJ. Iron Sucrose Injection. Hospital Pharmacy 2001;36:404–12. Cada DJ. Iron Sucrose Injection. Hospital Pharmacy 2001;36:404–12. 45
 Maintain TSAT between 20% and 50% Iron therapy should be withheld in patients with TSAT ≥50% Iron therapy should be withheld in patients with ferritin values ≥800 ng/mL. Since transferrin saturation values increase rapidly after IV administration of iron sucrose, serum iron values may be reliably obtained 48 hours after IV iron sucrose dosing. Hemoglobin, hematocrit, and iron status should be monitored periodically in patients receiving iron sucrose therapy. Iron status in patients receiving epoetin alfa should be monitored by the percent transferrin saturation (TSAT) and the serum ferritin level. In patients receiving epoetin alfa, iron supplementation should be administered to maintain serum ferritin at > 100 mcg/L but not exceeding. 800 mcg/L and transferrin saturation at > 20% but not exceeding 50%. Hypochromic red blood cells should be maintained at less than 10%. Iron. status should be monitored monthly initially, then every 2 to 3 months. Because transferrin saturation increases rapidly after the IV administration. of iron sucrose, reliable serum iron values can be obtained 48 hours after administration. Iron therapy should be withheld in patients with evidence of iron overload. Ref: Cada DJ. Iron Sucrose Injection. Hospital Pharmacy 2001;36:404–12. Cada DJ. Iron Sucrose Injection. Hospital Pharmacy 2001;36:404–")
46
Anemia management in CKD – NKF K/DOQI GUIDELINES
Both iron & EPO need to be given Most patients need IV iron Iron deficiency is detected when TSAT is <20% and the serum ferritin is <100 ng/mL Withhold IV iron if TSAT is ≥50% & Ferritin is ≥ 800ng/ml 1. Both iron and erythropoietin are needed to produce red blood cells; as a result, unless adequate iron is available, Epoetin will be relatively ineffective. 2. In the absence of provision of supplemental iron, iron deficiency is almost always present in nontransfused hemodialysis patients receiving Epoetin. 3. Although some hemodialysis patients have been able to avoid absolute and functional iron deficiency by taking only oral iron supplements, most hemodialysis patients require IV iron to maintain sufficient iron to achieve and maintain an Hgb (Hct) of 11 to 12 g/dL (33% to 36%). 4. Just as there is risk associated with the failure to use IV iron (because many patients will be anemic unless they receive IV iron, and anemia is associated with increased morbidity and mortality), there also is some risk associated with the use of IV iron dextran and ferric sodium gluconate 5. Although no tests are perfect indicators of the adequacy of iron stores, the TSAT and serum ferritin are the best measures of the body’s iron status that we currently have. The probability that iron deficiency is present increases as the values of these measures decrease. 6. Given the prevalence of iron deficiency in CKD patients, and the sensitivity and specificity of TSAT and serum ferritin in detection of iron deficiency, the likelihood of iron deficiency is sufficiently high when TSAT is <20% and the serum ferritin is <100 ng/mL. Therefore, the TSAT and serum ferritin should be maintained at a level of >20% and >100 ng/mL, respectively, in all patients. 7. Because many patients will still be functionally iron deficient even with a TSAT >20%, and/or serum ferritin >100 ng/mL, additional iron should be given to patients whose TSAT is >20% and/or serum ferritin is >100 ng/mL, whenever the Hct is <33% and/or Epoetin doses are greater than anticipated, so long as administration of such iron does not chronically maintain the TSAT at >50% or serum ferritin at >800 ng/mL. There is no single level of TSAT or serum ferritin that is optimal for all patients. The goal of iron therapy is to improve erythropoiesis, not to attain specific levels of TSAT and/or serum ferritin. The probability that functional iron deficiency exists despite a TSAT >20% is greater in patients who require higher doses of Epoetin. 8. The levels of TSAT or serum ferritin above which patients will have iron overload is not known. Patients with transfusional hemosiderosis have a TSAT >80%. There is no known risk associated with a TSAT that is 50%. Conversely, there is no physiologic or clinical rationale for maintaining TSAT >50%. Serum ferritin levels between 300 and 800 ng/mL have been common in dialysis patients, and there has been no evidence that such levels are associated with adverse, iron-mediated effects. 9. Because of the repetitive dialyzer-related blood losses in hemodialysis patients, iron overload can be avoided by temporarily withholding IV iron administration if TSAT or ferritin levels temporarily become too high. 10. By monitoring the TSAT and serum ferritin at least once every 3 months, erythropoiesis can be optimized in hemodialysis patients by adjusting the pro-rated weekly dose of IV iron to maintain adequate iron status. 46
 of 11 to 12 g/dL (33% to 36%). 4. Just as there is risk associated with the failure to use IV iron (because many patients will be anemic unless they receive IV iron, and anemia is associated with increased morbidity and mortality), there also is some risk associated with the use of IV iron dextran and ferric sodium gluconate. 5. Although no tests are perfect indicators of the adequacy of iron stores, the TSAT and serum ferritin are the best measures of the body’s iron status that we currently have. The probability that iron deficiency is present increases as the values of these measures decrease. 6. Given the prevalence of iron deficiency in CKD patients, and the sensitivity and specificity of TSAT and serum ferritin in detection of iron deficiency, the likelihood of iron deficiency is sufficiently high when TSAT is <20% and the serum ferritin is <100 ng/mL. Therefore, the TSAT and serum ferritin should be maintained at a level of >20% and >100 ng/mL, respectively, in all patients. 7. Because many patients will still be functionally iron deficient even with a TSAT >20%, and/or serum ferritin >100 ng/mL, additional iron should be given to patients whose TSAT is >20% and/or serum ferritin is >100 ng/mL, whenever the Hct is <33% and/or Epoetin doses are greater than anticipated, so long as administration of such iron does not chronically maintain the TSAT at >50% or serum ferritin at >800 ng/mL. There is no single level of TSAT or serum ferritin that is optimal for all patients. The goal of iron therapy is to improve erythropoiesis, not to attain specific levels of TSAT and/or serum ferritin. The probability that functional iron deficiency exists despite a TSAT >20% is greater in patients who require higher doses of Epoetin. 8. The levels of TSAT or serum ferritin above which patients will have iron overload is not known. Patients with transfusional hemosiderosis have a TSAT >80%. There is no known risk associated with a TSAT that is 50%. Conversely, there is no physiologic or clinical rationale for maintaining TSAT >50%. Serum ferritin levels between 300 and 800 ng/mL have been common in dialysis patients, and there has been no evidence that such levels are associated with adverse, iron-mediated effects. 9. Because of the repetitive dialyzer-related blood losses in hemodialysis patients, iron overload can be avoided by temporarily withholding IV iron administration if TSAT or ferritin levels temporarily become too high. 10. By monitoring the TSAT and serum ferritin at least once every 3 months, erythropoiesis can be optimized in hemodialysis patients by adjusting the pro-rated weekly dose of IV iron to maintain adequate iron status. 46.")
47
Monitoring iron stores in CKD
During initiation of EPO & increased dose: TSAT / serum ferritin to be checked every month in patients not receiving IV iron or once in three months in those receiving IV iron . Once target Hb% achieved: Check iron stores once in 3 months Best Practice Guidelines for management of Renal Anaemia, Indian J Nephrol 2005;15, Supplement 1: S32-S41

48
When should IV iron be discontinued?
IV iron should be discontinued when TSAT is >50% and Ferritin is > 800ng / ml. Best Practice Guidelines for management of Renal Anaemia, Indian J Nephrol 2005;15, Supplement 1: S32-S41

50
Initiation of Erythropoietin
Hb <12g/dl documented 2 weeks apart with minimum two hemoglobin estimations. EPO therapy should be initiated only after correcting iron, Vitamin B12 and Folic acid deficiency, and other possible factors contributing to anaemia. Best Practice Guidelines for management of Renal Anaemia, Indian J Nephrol 2005;15, Supplement 1: S32-S41

51
Treatment with Erythropoietin
EPO should be started at a dose of IU/Kg / week. IV administration preferred in HD patients Once the target Hb is achieved, Hb monitoring should be performed once every month Best Practice Guidelines for management of Renal Anaemia, Indian J Nephrol 2005;15, Supplement 1: S32-S41

52
Treatment with Erythropoietin
1gm/dl rise in Hb is necessary with EPO therapy at the end of 2 weeks. EPO dosage can be increased by 50% till the target Hb is achieved. If the rise in Hb is > 1.5Gms% at the end of 2 weeks, the dose of EPO to be reduced by 25% Best Practice Guidelines for management of Renal Anaemia, Indian J Nephrol 2005;15, Supplement 1: S32-S41

53
KDOQI (2006) targets for patients on dialysis
Hemoglobin (Hb) > 11 g/dL, caution when intentionally maintaining Hb 13 g/dL.
 > 11 g/dL, caution when intentionally maintaining Hb 13 g/dL.")
54
Inadequate response to EPO
Most common causes: iron deficiency non-compliance to EPO therapy Dialysis inadequacy Best Practice Guidelines for management of Renal Anaemia, Indian J Nephrol 2005;15, Supplement 1: S32-S41

55
Inadequate response to EPO
Other causes: Folate or Vitamin B 12 deficiency Chronic blood loss Infection / inflammation (e.g., access infections, surgical inflammation, AIDS, SLE, Occult Tuberculosis/Chronic Malaria / Kalazar) Malnutrition, Hemolysis, Hyperparathyroidism, Aluminium toxicity Haemoglobinopathies Multiple myeloma & other malignancies. Use of ACE-1 / ARB agents Best Practice Guidelines for management of Renal Anaemia, Indian J Nephrol 2005;15, Supplement 1: S32-S41
 Malnutrition, Hemolysis, Hyperparathyroidism, Aluminium toxicity. Haemoglobinopathies. Multiple myeloma & other malignancies. Use of ACE-1 / ARB agents. Best Practice Guidelines for management of Renal Anaemia, Indian J Nephrol 2005;15, Supplement 1: S32-S41.")
56
Adequacy of Dialysis During thrice weekly maintenance haemodialysis KT/V of >1.2 is to be achieved to ensure optimal dialysis. Best Practice Guidelines for management of Renal Anaemia, Indian J Nephrol 2005;15, Supplement 1: S32-S41

57
Resistance to EPO Failure to achieve target Hb concentration while receiving more than 300IU/kg/week and continued need for such dosage to maintain target in presence of adequate iron stores and absence of functional deficiency of iron. Best Practice Guidelines for management of Renal Anaemia, Indian J Nephrol 2005;15, Supplement 1: S32-S41

58
Pure Red Cell Aplasia Suspect pure red cell aplasia
In patients treated with EPO > 4 weeks who develop sudden and rapid decline in Hb concentration > g/dl/week. Or requires transfusion of units of red cells with normal platelets and white cell counts, in the absence of any other obvious clinical cause. Confirmation of diagnosis Severe non regenerative anaemia with erythroid hypoplasia of the bone marrow and normal cellularity of the other elements. Less than 5 % erythroblasts in the marrow with evidence of red cell precursor block. Demonstration of anti erythropoietin antibodies in the patients serum. Best Practice Guidelines for management of Renal Anaemia, Indian J Nephrol 2005;15, Supplement 1: S32-S41

59
Adjuvant Therapies for treatment of anaemia
L-carnitine L-carnitine may enhance response to Epoetin when used as adjuvant. Vitamins Oral vitamin E 1200IU given 6 hrs before a HD session along with intensive iron may protect patients against oxidative stress related diseases. Hypo responsiveness to EPO therapy can be reduced by correcting depleted vitamin C levels administered along with vitamin E Best Practice Guidelines for management of Renal Anaemia, Indian J Nephrol 2005;15, Supplement 1: S32-S41

60
Red Cell Transfusions in CKD
Transfusions should be avoided as far as possible. Indications for transfusion are Severely anaemic patient with recognized symptoms or signs of anaemia. (acute blood loss with angina / haemodynamic instability) EPO resistant patient with chronic blood loss If transfusion is mandatory in patients for renal transplant, use leucocyte filters and irradiated blood. Best Practice Guidelines for management of Renal Anaemia, Indian J Nephrol 2005;15, Supplement 1: S32-S41
 EPO resistant patient with chronic blood loss. If transfusion is mandatory in patients for renal transplant, use leucocyte filters and irradiated blood. Best Practice Guidelines for management of Renal Anaemia, Indian J Nephrol 2005;15, Supplement 1: S32-S41.")
61
Other indications for Iron Sucrose

62
Fetal Diagn Ther 2009 June 5;25(2):239-245
Selective Use of Recombinant Human Erythropoietin in Pregnant Patients with Severe Anemia or Nonresponsive to Iron Sucrose Alone Krafft A, Bencaiova G, Breymann C. Feto-Maternal Hematology Group, Division of Obstetrics, Department of Obstetrics and Gynecology, University Hospital Zurich, Zurich, Switzerland. This study shows an effective treatment regimen for patients with various degrees of anemia in pregnancy. Iron sucrose is a safe and effective treatment option. In cases of severe iron deficiency anemia or poor response to parenteral iron therapy additional administration of rhEPO might be considered. However, the mechanism for not responding to intravenous iron therapy despite iron deficiency anemia still remains unclear to a large extent. Fetal Diagn Ther June 5;25(2):
:")
63
Am J Obstet Gynecol 2001 Mar;184(4):662-7
Efficacy and safety of intravenously administered iron sucrose with and without adjuvant recombinant human erythropoietin for the treatment of resistant iron-deficiency anemia during pregnancy Breymann C, Visca E, Huch R, Huch A. Department of Obstetrics and Gynecology, the Clinic of Obstetrics, and the Division of Perinatal Physiology, University of Zurich, Switzerland. Adjuvant recombinant human erythropoietin safely enhanced the efficacy of iron sucrose in the treatment of gestational iron-deficiency anemia resistant to orally administered iron alone. Am J Obstet Gynecol Mar;184(4):662-7
:")
64
A randomized, double-blind, placebo controlled, multi-center study of intravenous iron sucrose and placebo in the treatment of restless legs syndrome Grote L, Leissner L, Hedner J, Ulfberg J. Sleep Disorders Center, Department of Pulmonary Medicine, Sahlgrenska University Hospital, Gothenburg, Sweden. This study showed a lack of superiority of iron sucrose at 11 weeks but found evidence that iron sucrose reduced RLS symptoms both in the acute phase (7 weeks) and during long-term follow up in patients with variable degree of iron deficiency. Further studies on target patient groups, dosing and dosing intervals are warranted before iron sucrose could be considered for treatment of iron deficient patients with RLS. Moy Disord 2009 June 1
 and during long-term follow up in patients with variable degree of iron deficiency. Further studies on target patient groups, dosing and dosing intervals are warranted before iron sucrose could be considered for treatment of iron deficient patients with RLS. Moy Disord 2009 June 1.")
65
Safety and usefulness of intravenous iron sucrose in the management of preoperative anemia in patients with menorrhagia: a phase IV, open-label, prospective, randomized study Kim YH, Chung HH, Kang SB, Kim SC, Kim YT. Department of Obstetrics and Gynecology, College of Medicine, Seoul National University, Seoul, Korea. Preoperative intravenous iron sucrose administration is more effective than oral iron and is as safe as oral iron therapy in the correction of preoperative anemia due to menorrhagia. Acta Haematol 2009;121(1):37-41
:")
66
Scand J Gastroenterol 2009 Mar 27:1-8
Intravenous iron sucrose is superior to oral iron sulphate for correcting anaemia and restoring iron stores in IBD patients: A randomized, controlled, evaluator-blind, multicentre study Lindgren S, Wikman O, Befrits R, Blom H, Eriksson A, Granno C, Ung KA, Hjortswang H, Lindgren A, Unge P. Department of Medicine, Gastroenterology-Hepatology Division, University Hospital MAS, Malmo. Treatment with intravenous iron sucrose is effective, safe, well tolerated and superior to oral iron in correcting haemoglobin and iron stores in patients with IBD. Scand J Gastroenterol Mar 27:1-8

67
Med Clin (Barc) 2009 Mar7;132(8):303-6
Usefulness of the administration of intravenous iron sucrose for the correction of preoperative anemia in major surgery patients Muñoz M, García-Erce JA, Díez-Lobo AI, Campos A, Sebastianes C, Bisbe E; Anaemia Working Group España (AWGE). Because of the low incidence of side effects and the rapid increase of hemoglobin levels, IVIS emerges as a safe, effective drug for treating preoperative anemia in surgery patient populations. Med Clin (Barc) Mar7;132(8):303-6
. Because of the low incidence of side effects and the rapid increase of hemoglobin levels, IVIS emerges as a safe, effective drug for treating preoperative anemia in surgery patient populations. Med Clin (Barc) 2009 Mar7;132(8):")
68
Isr Med Assoc J 2008 May;10(5):335-8
Efficacy and safety of intravenous iron sucrose therapy in a group of children with iron deficiency anemia Pinsk V, Levy J, Moser A, Yerushalmi B, Kapelushnik J. Pediatric Day Care Unit, Soroka University Medical Center, Faculty of Health Sciences, Ben-Gurion University of the Negev, Beer Sheva, Israel. These preliminary data suggest that administration of intravenous iron sucrose in pediatric patients is well tolerated and has a good clinical result, with minimal adverse reactions. Isr Med Assoc J May;10(5):335-8
:")
69
Acta Obstet Gynecol Scand 2008;87(9):916-23
A 12-week randomised study comparing intravenous iron sucrose versus oral ferrous sulphate for treatment of postpartum anemia. Westad S, Backe B, Salvesen KA, Nakling J, Økland I, Borthen I, Rognerud Jensen OH, Kolås T, Løkvik B, Smedvig E. Department of Obstetrics and Gynecology, Innlandet Hospital Trust, Lillehammer, Norway. Women who received 600 mg intravenous iron sucrose followed by standard oral iron after four weeks, replenished their iron stores more rapidly and had a more favorable development of the fatigue score indicating improved quality of life. Acta Obstet Gynecol Scand 2008;87(9):916-23
:")
70
Journal of Clinical Oncology, 2007,Vol 25, No.18S,9109
A phase III randomized controlled study comparing iron sucrose intravenously (IV) to no iron treatment of anemia in cancer patients undergoing chemotherapy and erythropoietin stimulating agent (ESA) therapy R. E. Bellet, H. Ghazal, M. Flam, A. Drelichman, N. Gabrail, D. Woytowitz, D. Loesch, D. Niforos, A. Mangione, L. Anthony and Iron Sucrose Study Group IV iron sucrose increased Hgb levels and iron stores significantly and is well tolerated in doses up to 500 mg increments in ESA treated patients with cancer chemotherapy- related anemia. IV iron sucrose should be considered in combination with erythropoietic therapy in anemic cancer patients receiving chemotherapy. Journal of Clinical Oncology, 2007,Vol 25, No.18S,9109
 to no iron treatment of anemia in cancer patients undergoing chemotherapy and erythropoietin stimulating agent (ESA) therapy. R. E. Bellet, H. Ghazal, M. Flam, A. Drelichman, N. Gabrail, D. Woytowitz, D. Loesch, D. Niforos, A. Mangione, L. Anthony and Iron Sucrose Study Group. IV iron sucrose increased Hgb levels and iron stores significantly and is well tolerated in doses up to 500 mg increments in ESA treated patients with cancer chemotherapy- related anemia. IV iron sucrose should be considered in combination with erythropoietic therapy in anemic cancer patients receiving chemotherapy. Journal of Clinical Oncology, 2007,Vol 25, No.18S,9109.")
71
Summary Iron (blood) losses are high in HD patients
Regular use of intravenous (IV) iron improves sensitivity to Erythropoietin maintain TSAT >20% and ferritin >200 ng/mL Adequate and appropriate dosing of Erythropoietin is necessary Aim for Hemoglobin (Hb) > 11 g/dL, caution when intentionally maintaining Hb 13 g/dL.
 iron improves sensitivity to Erythropoietin. maintain TSAT >20% and ferritin >200 ng/mL. Adequate and appropriate dosing of Erythropoietin is necessary. Aim for Hemoglobin (Hb) > 11 g/dL, caution when intentionally maintaining Hb 13 g/dL.")
72
Key points Anemia in CKD patients is common
EPO therapy forms the mainstay of treatment EPO therapy alone may be ineffective unless supplemented by iron Oral iron supplementation has problems of intolerance IV iron forms the best adjunct with EPO in CKD patients Anemia in CKD patients is common. EPO therapy forms the mainstay of treatment. EPO therapy alone may be ineffective unless supplemented by iron. Oral iron supplementation has problems of intolerance. IV iron forms the best adjunct with EPO in CKD patients 72

73
Key points IV iron sucrose is one of the iron preparations
It is indicated in hemodialysis patients, non hemodialysis patients with or without EPO and peritoneal dialysis patients Efficacy is proved in each of these indications Low maintenance dose of Iron sucrose keeps Hb and Hct stable in hemodialysis patients IV iron sucrose is one of the iron preparations. It is indicated in hemodialysis patients, non hemodialysis patients with or without EPO and peritoneal dialysis patients. Efficacy is proved in each of these indications. Low maintenance dose of Iron sucrose keeps Hb and Hct stable in hemodialysis patients. 73

74
Key points Iron sucrose administration along with EPO reduces the dose requirement of EPO Iron sucrose can be safely given to patients hypersensitive to iron dextran Iron sucrose is safer than other IV iron preparations Iron sucrose administration along with EPO reduces the dose requirement of EPO. Iron sucrose can be safely given to patients hypersensitive to iron dextran. Iron sucrose is safer than other IV iron preparations. 74

75
Thank You

Similar presentations




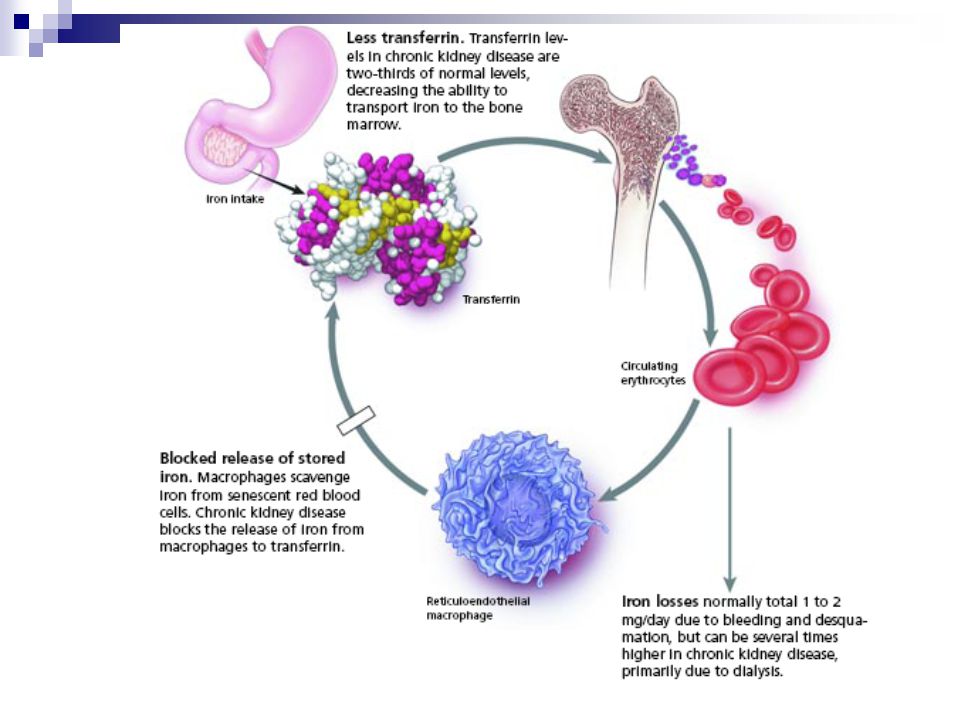







 Sofia Medical University. Background Erythropoiesis-stimulating agents are man-made versions of a natural protein known as erythropoietin.>")






 Kingsbrook Jewish Medical Center Clinical Instructor of Pharmacy Practice.>")





