Download presentation
Presentation is loading. Please wait.

1
Omental Infarction and Epiploic Appendagitis
Scott Nguyen MD Oct 10, 2006

2
Epiploic Appendagitis
Small adipose protrusions from serosal surface of colon located along taenia throughout colon Most located at sigmoid or rectum, cecum Supplied by small artery and vein through the narrow pedicle Mobility of the fat-laden heavy appendix makes it prone to torsion, kinking, or stretching resulting in venous thrombosis

3
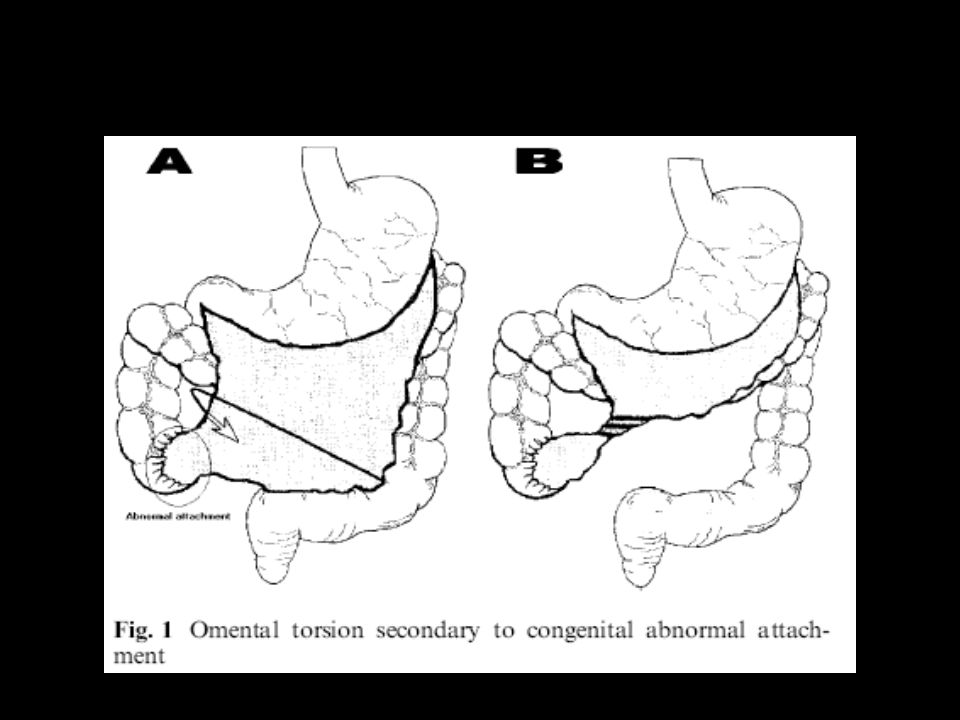
Omental Infarction Segment of Omentum succeptible to infarction as a result of torsion or venous thrombosis Primary and Secondary Predilection for Right Abdomen Primary and Secondary Secondary – associated w/ another intraabdominal process (omental cyst, hernia, tumor, adhesion, post surgery) Predilection for Right Abdomen d/t abnormality in embryonic formation of the Right side of the omentum and Right epliploic vessels Right omentum longer and more mobile
 Predilection for Right Abdomen. d/t abnormality in embryonic formation of the Right side of the omentum and Right epliploic vessels. Right omentum longer and more mobile.")
5
Risk Factors for Torsion or Infarction
OBESITY Fat accumulation in appendices – pedunculated nature and mobility increase chances of torsion Fat deposition may outgrow the bloody supply predisposing to ischemia Heavy exercise and excessive stretching – excess movement of omentum

6
EA – prevalence in LLQ often misdiag as diverticulits
OT – R abdomen…cholecystitis or appy European Radiology

7
Epiploic Appendigits J Clinical Ultrasound 2002 30:481-95
Only few series in literature…..few cases over many years Concentrated in LLQ Since diverticulitis was often working diagnosis, CT was method of choice in diagnosing these Often initially thought to be diverticulitis CT confirmed that was EA J Clinical Ultrasound :481-95

8
Epiploic Appendagitis often misdiagnosed as Diverticulitis
Retrospective Korean study comparing 8 EA to 18 Diverticulitis Often confused for Diverticulitis EA – no assoc GI sx, few w/ fever and leukocytosis IF do BE then will see no diverticulitis and see mass effect from appendix inflammation

9
Omental Infarction More often found at exploration for possible appendicitis Higher likelihood of resection Several reports in children, especially obese

10
Normal Epiploic Appendices

11
US normal epiploic appendices

12
CT Epiploic Appendagitis
Typical CT findings -- central hypodensity is fat of appendix, w/ surrounding inflamm rim Adjacent colon is normal Inflamm can adhere to anterior abd wall

14
Tendency to Abut abdominal wall

15
Sometimes can see central hyperdensity w/in append -- area of necrosis or hemorrhage, or thrombosis
2nd image w/ normal contrast filled diverticula

16
Sonogram Sonographic findings – hyperechoic ovoid lesion, Hypoechoic rim. Hypoechoic center – necrosis. US easy cause these usu right underneath abd wall

17
Treatment Epiploic Appendagits
Conservative No surgery necessary Symptoms treated with analgesics No antibiotics necessary Most literature support Imaging saves patient from exploratory laparotomy Repeat imaging often shows complete resolution of inflammation Occasionally fibrous band or calcified appendage may remain

18
CT at 6 weeks to see almost resolution of inflammation

19
Epiploic Appendagitis
Rarely complications of nonoperative management 4 cases of abscess formation 1 case intestinal obstruction from adhesions

20
Omental Infarct Usually ill defined heterogenous fat density if in early stage ( < 15 days) Cake like density
 Cake like density.")
22
Sometimes can see whorling of omentum……consistent w/ omental torsion

23
Evolves to a smaller, well defined lesion w/ a continous hyperdense rim > 30 days

24
Evolutionary changes in omental infarcts
Evolutionary changes in omental infarcts. Unlike epiploic appendagitis, which resolves completely upon repeat imaging. F/u imaging usually results in smaller fat lesion w/ hyperdense rim

25
Evolutionary changes

26
Micrographs reveal a intense inflammatory infiltrate into the fat

27
Treatment of Omental Infarction
Observation NSAIDS No need for antibiotics Rarely abscess

28
Largest Series in Literature 40 patients, 1988-1997
20 epiploic appendagitis 11 Omental infarction 9 Unspecified abdominal focal fat infarction All had CT or US No patients had to undergo exploration No antibiotics Most had symptoms resolve w/in 7 days

29
Appendices Epiploicae
“They rarely excite much notice, except to be cursed as an impediment to precise anastomosis of the colon or gratefully acknowledged as an added measure of protection when used to reinforce a precarious suture line.”

Similar presentations