Download presentation
Presentation is loading. Please wait.

1
Puberty By Dr. Khattab Omar
Prof. & Head of Obstetrics and Gynaecology Faculty of Medicine, Al-Azhar University, Damietta

2
Definition: It is the period of time during which 2ry sexual character-istics develop, menstruation begins and the psychological outlook changes. It is the process by which sex-ually immature persons be-come capable of reproduction. Pubertal changes include changes in body, mind and emotions.

3
- breast growth, - pubic hair growth, - axillary hair growth,
The body changes occur in 5 stages: - breast growth, - pubic hair growth, - axillary hair growth, - growth spurt and - menarche.

4
Sequences of pubertal events:
The 1st steroid to increase is DHEA (at 6-8y). Adrenarche(in DHEA, DHEAS & androstenedione) axillary (& pubic) hair growth with an increase in size & differentiation of the zona reticularis.
. Adrenarche(in DHEA, DHEAS & androstenedione) axillary (& pubic) hair growth with an increase in size & differentiation of the zona reticularis.")
5
In hypergonadotrophic & hypo-gonadotrophic hypogonadism (e. g
In hypergonadotrophic & hypo-gonadotrophic hypogonadism (e.g. gonadal dysgenesis & Kallmann’s syndrome) adrenarche occurs despite the absence of gonadarche. Adrenarche is not under control of Gn, ACTH or PRL. The stimulator appears to be a pituitary adrenal androgrn stimulat-ing factor (CASH, from the precursor pro-opio-melancortin [POMC]) which acts on ACTH-prepared & maintained adrenals.
 adrenarche occurs despite the absence of gonadarche. Adrenarche is not under control of Gn, ACTH or PRL. The stimulator appears to be a pituitary adrenal androgrn stimulat-ing factor (CASH, from the precursor pro-opio-melancortin [POMC]) which acts on ACTH-prepared & maintained adrenals.")
6
Decreasing repression of the 'gonadostat’.
The proposed mechanism of ‘gonadostat’ is hypersensitivity to the -ve feedback of est-rogen -- the important role in early childhood. Gonadostat reaches a max at the age of 7.

7
Gradual amplification of the GnRH–Gn & Gn–steroid (the hypothalamo-pituitary-gonadal axis) interactions leading to 'gonadarche‘. FSH, then LH levels rise moderately before the age of 10. FSH rises initially, then plateaus in mid-puberty, while LH rises more slowly and reaches adult levels in late puberty). GnRH&LH pulses first increase during sleep Augmentation of pulsatile Gn secretion is the essential hormonal event of puberty. It is affected by endocrine, nutritional & psychological factors.
. GnRH&LH pulses first increase during sleep Augmentation of pulsatile Gn secretion is the essential hormonal event of puberty. It is affected by endocrine, nutritional & psychological factors.")
8
Gonadarche rise in estradiol level breast development, female fat distribution, as well as vulvar, vaginal and uterine growth.

10
Also, growth hormone (GH) secretion becomes critically dependent on the gonadal estrogen secretion
GH levels increase before the appearance of any sign of sexual development. It stimulates the produc-tion of IGF-I.

11
- Menarche occurs when body weight is 42-52 kg and 17% of this is fat.
- Ovulation: Regular ovulation occurs about 20 months after menarche.

12
Hypothalamus Ant. Pituit. Gn secretion FSH CASH & ACTH GH ovary Adrenarche IGF-I in No. of growing follicles Skeletal growth in estrogen Growth of 2ry sexual organs in E2 first is irregular Irregular anovulatory menses then E2 rises steadily to a critical level LH secretion & ovulation + regular cycles

13
Timing and duration: Reversal of central inhibition (by GnRH – the important role in late child-hood) is due to a reduction in melatonin secretion. Puberty occurs at the age of 11.5 y over a period of 2-5 y. There is a correlation between the age of onset & duration of puberty; the earlier the onset, the longer the duration.

14
The major determinant of the timing of puberty is genetic.
Other factors appearing to influence the timing and the rate of progress-ion of puberty are: geographic loca-tion, exposure to light, general health & nutrition, and psychologic factors. The principal factor responsible for normal pubertal growth is insulin-like factor I (IGF -I), the mediator of sex steroid induction of growth.
, the mediator of sex steroid induction of growth.")
15
Male : female skeletal mass or muscle mass = 1.5
Female : male body fat = 2. Breast development, pubic hair and axillary hair development constitute the base of the Tanner system of classification.

16
Initial growth acceleration occurs first
Initial growth acceleration occurs first. Growth spurt occurs over a period of about 2 y in an average rate of 8 cm/y. Pubic hair develops over a period of about 3 y. Breast development completes over a period of about 4 y (between 9 & 12). Menarche occurs around the age of 12.6. As a rule, pubic hair & breast develop-ment precede menarche by about 2 y. Puberty (& growth spurt) starts in girls 2 y earlier than in boys.
. Menarche occurs around the age of As a rule, pubic hair & breast develop-ment precede menarche by about 2 y. Puberty (& growth spurt) starts in girls 2 y earlier than in boys.")
17
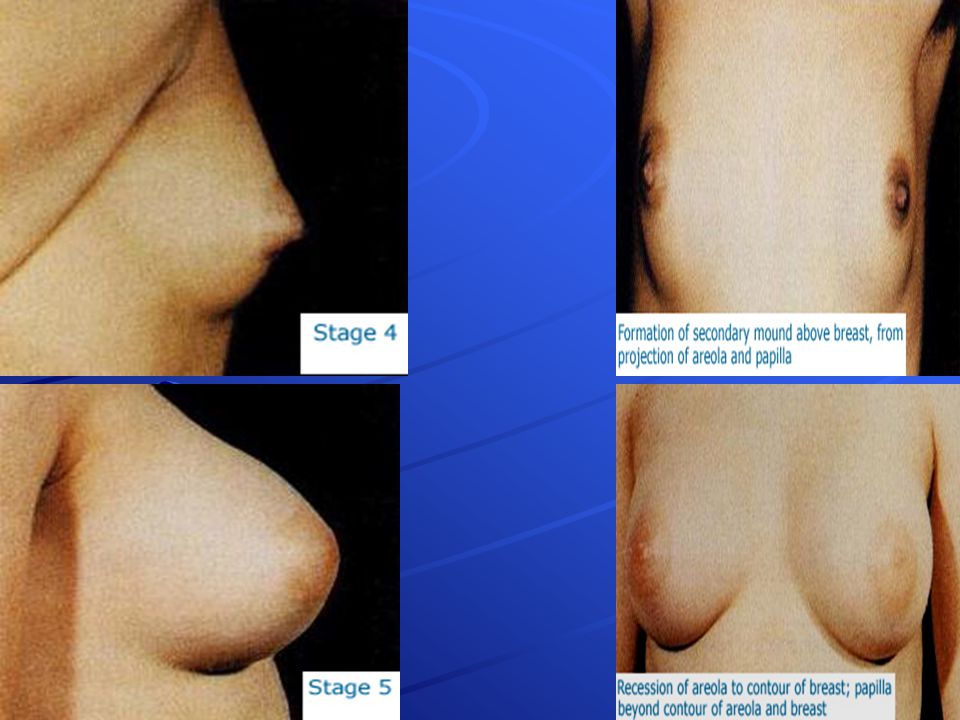
Tanner classification of female adolescent development.
Pubic hair Breast Stage None Papillae elevated (pre-adolescent), no breast buds. I Sparse, long slightly pigmen. Breast buds & papillae slightly elevated. II Dark, course, curly. Breasts and areolae confluent, elevated. III Adult-type, pubis only Areolae and papillae project above breast. IV Lateral distribution. Papillae projected, mature. V
, no breast buds. I. Sparse, long slightly pigmen. Breast buds & papillae slightly elevated. II. Dark, course, curly. Breasts and areolae confluent, elevated. III. Adult-type, pubis only. Areolae and papillae project above breast. IV. Lateral distribution. Papillae projected, mature. V.")
20
Problems of puberty These include: 1- Acne, 2- Wrong shape, 3- PMS, 4- Dysmenorrhoea, 5- Precocious puberty and 6- Delayed puberty.

21
PRECOCIOUS PUBERTY Definition: It is development of breast (or any 2ry sexual characteristic) before the age of 8 y, or menarche before the age of 10. Incidence: Precocity occurs in girls 5-x more frequently than boys.
 before the age of 8 y, or menarche before the age of 10. Incidence: Precocity occurs in girls 5-x more frequently than boys.")
22
Aetiology: 1- Most cases (90%) are constitutional (idiopathic; with Gn levels). In girls over the age of 4 years a specific aetiology is rarely found! A familial form does exist, but it is more common in boys.

23
2- CNS problems (7%) e.g. encephal-itis, meningitis & intracranial lesions. Hypothalamic hamartoma is the most common lesion in very young girls. An injury to the skull can stimulate precocity after a latent period of 1-2 months. The proposed mechanism is damage to the neural arm of the gonadostat. CNS neoplasms include optic gliomas and neurofibromas. Pineal tumours can be a cause only in male precocious puberty.

24
3- McCuneAlbright’s syndrome: 5%.
Polyostotic fibrous dysplasia and café au lait patches. Patients are usually younger than those of idiopathic precocity. In most of the cases vaginal bleeding is the first sign.

25
4- Feminizing ovarian tumour ( Gn levels; 10%)
4- Feminizing ovarian tumour ( Gn levels; 10%). It may be a functioning tumour or a benign one that induces the surrounding ovarian tissue to produce steroids Differential diagnosis: Ovarian tumour precocious puberty Vs. follicular cyst precocious puber Hepatoma and adrenal adenoma are extremely rare causes.
. It may be a functioning tumour or a benign one that induces the surrounding ovarian tissue to produce steroids. Differential diagnosis: Ovarian tumour precocious puberty Vs. follicular cyst precocious puber. Hepatoma and adrenal adenoma are extremely rare causes.")
26
5- Adrenal hyperplasia or tumour virilizing prec. pub
5- Adrenal hyperplasia or tumour virilizing prec. pub. (1%) or feminizing prec. pub. (1%). 6- Drugs like oestrogens.
 or feminizing prec. pub. (1%). 6- Drugs like oestrogens.")
27
The first 3 causes result in true prec pub (constitutional cases and CNS problems are GnRH-dependent, while Mc Cune Albright’s syndrome is GnRH-independent), … while the last 3 causes result in false precocious puberty (i.e. manifestations are reversible with removal of the cause. It may be partial or incomplete)
.")
28
Presentation: Increased growth is often the first change, followed usually by thelarche and pubarche. McCune Albright syndrome can be associated with ovarian cysts, GH- and PRL-secreting adenomas, hyperthyroidism, hyperparathyroidism and Cushing’s disease. FSH & LH levels are low. Hepatitis, intestinal polyposis and cardiac arrhythmias could occur. Premature thelarche: It most commonly occurs between 1 and 3 years of age. It may affect one or both breasts. Somatic growth is not accelerated and bone age isn’t advanced. Premature pubarche: It affects pubic &/or axillary hair. It may be idiopathic. Children tend to be slightly taller with marginally advanced bone age and slightly elevated DHEA. Early cases may occur 2ry to androgen excess (CAH or Leydig cell tumor). Premature menarche: Surprisingly, E2 levels are in the prepubertal range. Other causes of vaginal bleeding should be excluded.
. Premature menarche: Surprisingly, E2 levels are in the prepubertal range. Other causes of vaginal bleeding should be excluded.")
30
Diagnostic priority: Exclude life-threatening neoplasms of the CNS, ovaries and adrenals. Although most cases are idiopathic, this should be a diagnosis by exclusion.

31
State age at onset, duration and progression.
Work-up: State age at onset, duration and progression. Deduce family history & review body systems Examine skin for acne, adult-type body odor &café au lait patches Assess maturation of breasts and genitalia. Essential and basic is a left hand-wrist x-ray film. Head CT/MRI, abdominal & pelvic USS FSH, LH & hCG assay TFTs (TSH & free T4) DHAS, 17-OH-P, E2, testosterone & progesterone GnRH testing
 DHAS, 17-OH-P, E2, testosterone & progesterone. GnRH testing.")
32
Approach to diagnosis:
* Full signs of prec pub + pubertal levels of Gn (basal & Gn RH stimulated) = ? pituitary source of Gn. * If Gn levels are suppressed by GnRH while E2 levels are markedly increased, = ? ectopic source of Gn. * Signs of sexual puberty + skeletal maturation = ? ovarian tumour or cyst (high E2 level & low Gn). NB: If progesterone level is high = ? Luteoma. * Signs of sexual puberty+ virilization=adrenal hyper-plasia (17 OH-P or DOC) or virilizing adrenal or ovarian tumour ( DHEA-S or androstenedione). * Signs of sexual puberty + vaginal bleeding + short stature with DELAYED bone age = hypothyroidism.
 = pituitary source of Gn. * If Gn levels are suppressed by GnRH while E2 levels are markedly increased, = ectopic source of Gn. * Signs of sexual puberty + skeletal maturation = ovarian tumour or cyst (high E2 level & low Gn). NB: If progesterone level is high = Luteoma. * Signs of sexual puberty+ virilization=adrenal hyper-plasia (17 OH-P or DOC) or virilizing adrenal or ovarian tumour ( DHEA-S or androstenedione). * Signs of sexual puberty + vaginal bleeding + short stature with DELAYED bone age = hypothyroidism.")
33
Treatment Prompt investigation and treatment are essential to avoid short stature. Causal treatment for tumours and hyperplasia. Cyproterone acetate, medroxyprogesterone acetate or testolactone (an aromatase inhibitor). GnRHa for true precocious puberty (idiopathic & neurologic) is the treatment of choice because it delays both somatic and skeletal maturation. Treatment is continued until the age of GnRHa therapy fails with McCune Albright synd and has little effect beyond Tanner stage 3. NB: Precocious puberty is not associated with premature menopause.
. GnRHa for true precocious puberty (idiopathic & neurologic) is the treatment of choice because it delays both somatic and skeletal maturation. Treatment is continued until the age of GnRHa therapy fails with McCune Albright synd and has little effect beyond Tanner stage 3. NB: Precocious puberty is not associated with premature menopause.")
34
DELAYED PUBERTY = No signs of puberty by the age of 14; no thelarche by the age of 13; no menarche by the age of 15. Management should not be postponed waiting for delayed menarche.

35
Aetiology: Hypergonadotrophic hypogonadism is the most frequent cause of delayed puberty (43%): Gn, steroids. Ovarian failure: - with abnormal karyotype = 26%. - with normal karyotype constitutes 17% (46,XX = 15%; 46,XY = 2%). Examples: Mumps, resistant ovary syndrome (absent follicular receptors for Gn) & autosomal recessive familial form.
. Examples: Mumps, resistant ovary syndrome (absent follicular receptors for Gn) & autosomal recessive familial form.")
36
Hypogonadotrophic hypogonadism
= 31%. This may be: Reversible (18%): Physiologic delay = 10%. GnRH challenge test differ-entiates constitutional delay from similar conditions. Weight loss/anorexia = 3%. Prolactinomas = 1.5%. Primary hypothyroidism = 1%. CAH = 1%. Cushing’s disease = 0.5%. Irreversible (13%): GnRH deficiency = 7%. Hypopituitarism = 2%. Craniopharyngeoma, in late childhood, is the most common neoplasm associated with delayed puberty = 1%. Congenital CNS defects = 0.5%. Other pituitary adenomas = 0.5%. Malignant pituitary tumours = 0.5%.
: Physiologic delay = 10%. GnRH challenge test differ-entiates constitutional delay from similar conditions. Weight loss/anorexia = 3%. Prolactinomas = 1.5%. Primary hypothyroidism = 1%. CAH = 1%. Cushing’s disease = 0.5%. Irreversible (13%): GnRH deficiency = 7%. Hypopituitarism = 2%. Craniopharyngeoma, in late childhood, is the most common neoplasm associated with delayed puberty = 1%. Congenital CNS defects = 0.5%. Other pituitary adenomas = 0.5%. Malignant pituitary tumours = 0.5%.")
37
Eugonadotrophic hypogonadism
= 26%. Delayed menarche with adequate 2ry sexual characters. Mullerian agenesis = 14%. Inappropriate feedback leading to anovulation & androgen excess (→ oestrogen excess) = 7%. Vaginal septum = 3%. Androgen insensitivity syndrome = 1%. Imperforate hymen = 0.5%. Hand-Schuller-Christian disease (histiocytosis-X) in children is associated with delayed growth & puberty. Loss of 10-15% of weight for height delayed puberty and/or menarche.
 = 7%. Vaginal septum = 3%. Androgen insensitivity syndrome = 1%. Imperforate hymen = 0.5%. Hand-Schuller-Christian disease (histiocytosis-X) in children is associated with delayed growth & puberty. Loss of 10-15% of weight for height delayed puberty and/or menarche.")
38
The commonest cause of delayed puberty is ovarian failure.
More than 1/4 of the girls with delayed puberty have chromosomal abnormalities.

39
Management Serum Gn assay is important in distinguishing hypo- & hyper-gonadtrophic causes of delayed puberty. With low FSH levels, skull films & prolactin assay are mandatory. Absent 2ry sexual characters: Conjugated estro-gen 1.5 mg twice daily until breast develop-ment is progressing or spotting occurs. Dose is then reduced to OD, with progestin (10 mg provera) is added for 10 days/month. Therapy is discontinued when the bone age matches the chronologic age. Patients with inappropriate feedback should receive progestins every other month to prevent endometrial hyperplasia.
 is added for 10 days/month. Therapy is discontinued when the bone age matches the chronologic age. Patients with inappropriate feedback should receive progestins every other month to prevent endometrial hyperplasia.")
40
Thank you

Similar presentations