Download presentation
Presentation is loading. Please wait.

1
Resuscitation and Post Resuscitation Care
Jose G. Cabanas, MD MPH FACEP Paul R. Hinchey, MD MBA FACEP Office of the Medical Director Austin-Travis County EMS System

2
Austin/Travis County EMS
Approximately 1.2 million citizens, 1,100 square miles, 120k EMS calls per year 1,000 cardiac arrests responses per year 14 Fire Departments (1,500 FF’s,) EMS Transport Agency (400 Paramedics) EMS Systems are judged by their cardiac arrest resuscitation rates Most large cities are 5-7% King Cnty Wa 35-45% Wake Cnty NC 38-42% Austin 38%
 EMS Transport Agency (400 Paramedics) EMS Systems are judged by their cardiac arrest resuscitation rates. Most large cities are 5-7% King Cnty Wa 35-45% Wake Cnty NC 38-42% Austin 38%")
3
Why are we talking about Cardiac Arrest Resuscitation?

4
Philosophy of Five Time Dependent Intervention Dependent
Acute MI (STEMI) Acute Stroke Trauma / Surgical Emergency Intervention Dependent Cardiac Arrest Respiratory Distress Sophisticated providers/systems understand the difference
 Acute Stroke. Trauma / Surgical Emergency. Intervention Dependent. Cardiac Arrest. Respiratory Distress. Sophisticated providers/systems understand the difference.")
5
Time Dependent These conditions can not be definitively treated in the pre-hospital environment Requires specialized intervention only available in the hospital Outcomes are improved by early access to definitive intervention Goal is recognition and short scene interval

6
Intervention Dependent
Initial treatment can be delivered in prehospital environment Outcomes linked to prehospital interventions Goal is identification and initiation of treatment Scene intervals are NOT critical

7
Updates in Out-of-Hospital Resuscitation and Post Resuscitation Care

8
Objectives Describe the importance of continuous compressions and controlled ventilations Discuss what to do with the airway/drugs Acknowledge the difficulty of performing continuous compressions and the need for a scripted process Discuss importance of on-scene post ROSC stabilization Describe role of resuscitation centers Identify questions for the future

9
Why do we worry about CA Represents < 1% of our calls but…
> 70% of CA arrests occur outside the hospital Definitive management of cardiac arrest is in the prehospital environment

10
“Stated succinctly, if ACLS care in the field cannot resuscitate the victim, ED care will not resuscitate the victim.”- 2005 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care (Part 7.2: Management of Cardiac Arrest)
")
11
Priorities in OOHCA Changed
Emphasis on compression Limit interruptions from ANYTHING Goal is to maximize % of time in compressions Single D-fib every two minutes Precharge monitor before break Follow d-fib immediately by compressions Decreased importance of ventilations Fewer number of breaths Each delivered more slowly

12
So if you had to push a car, would you push a few feet and stop…
So if you had to push a car, would you push a few feet and stop….. only to start again a few minutes later?

14
So how important are compressions?

15
Compression fraction article
Circulation 2009

16
If compressions are the most important therapy when do you move the patient…..

17
Prehospital Emergency Care 2011;15(1):106
:106")
18
Results (Pre-Feedback)
N = 108 % (25th, 75th) Scene Correct Rate% Median: (9.54, 59.6) Mean: CI (33.2, 43.78) Transport Correct Rate% Median: (5.83, ) Mean: CI (18.35, 27.97) Scene Correct Depth% Median: (15.96, 73.29) Mean: CI (38.76, 51.37) Transport Correct Depth% Median: (2.62, 49.01) Mean: CI (20.12, 32.63) Note: Box Plot with clear “skew” = nonparametric
 Scene Correct Rate% Median: 44.8 (9.54, 59.6) Mean: CI (33.2, 43.78) Transport Correct Rate% Median: (5.83, 39.32) Mean: CI (18.35, 27.97) Scene Correct Depth% Median: (15.96, 73.29) Mean: CI (38.76, 51.37) Transport Correct Depth% Median: 8.88 (2.62, 49.01) Mean: CI (20.12, 32.63) Note: Box Plot with clear skew = nonparametric.")
19
Results (Post-Feedback)
N = 35 % (25th, 75th) Scene Correct Rate% Median: (14.68, 62.36) Mean: CI (34.61, 52.59) Transport Correct Rate% Median: (9.52, 60.22) Mean: CI (23.21, 42.33) Scene Correct Depth% Median: (36.23, 95.07) Mean: CI (56.57, 77.16) Transport Correct Depth% Median: (4.78, 90.78) Mean: CI (27.98, 56.11)
 Scene Correct Rate% Median: (14.68, 62.36) Mean: 43.6 CI (34.61, 52.59) Transport Correct Rate% Median: 19.0 (9.52, 60.22) Mean: CI (23.21, 42.33) Scene Correct Depth% Median: (36.23, 95.07) Mean: CI (56.57, 77.16) Transport Correct Depth% Median: 14.0 (4.78, 90.78) Mean: CI (27.98, 56.11)")
20
How about ventilations?

21
Importance of controlled Ventilation
Normal inspiration is negative pressure Encourages blood return to the chest Artificial ventilation is positive pressure Reduces blood return to the chest The faster the ventilation rate the higher the mean intrathoracic pressure Higher MIP reduces cerebral emptying and reduces blood return to the heart

22
Survival in hyperventilation

23
STOP Hyperventilating
Telling providers not to hyperventilate is ineffective High adrenaline situation Tendency to ventilate faster and faster Requires conscious effort to slow rates Need constant reminder Timing device Goal directed ventilation

24
How to Deliver Ventilations
Goal is to oxygenate primarily and ventilate as a secondary consideration Must provide continuous uninterrupted compressions Traditional method is endotracheal intubation but increases interruption in compresions So is this a paradigm that needs to be challenged?

25
* Indicates median values reported
Interrupt CPR…not ME 100 Cardiac Arrests CPR interruptions 2* (1-9) 1st ETI interruption 46.5 s* (7-221 s) Total all ETI interruption s* ( s) 1/3 > 1 min; ¼ > 3 min ETI Interruptions 23% of all * Indicates median values reported Wang et al Ann Emerg Med
 1st ETI interruption 46.5 s* (7-221 s) Total all ETI interruption s* ( s) 1/3 > 1 min; ¼ > 3 min. ETI Interruptions 23% of all. * Indicates median values reported. Wang et al Ann Emerg Med")
26
But an advanced airway is a better airway…..

27
Advanced Airway Management
Advantages No mask seal required Easier to do Less manpower Allows continuous compressions Disadvantage Requires interruption of compressions Easier to hyperventilate (rate and volume) Doesn’t provide better ventilation/oxygenation
 Doesn’t provide better ventilation/oxygenation.")
28
173 LMA vs 200 BVM by paramedics No difference in median:
Pa CO v 55.3 (p=0.06) Pa O v 71.9 (p=0.056) There is no MAGIC to these devices
 Pa O v 71.9 (p=0.056) There is no MAGIC to these devices.")
29
Retrospective analysis of OOHCA 1,294 Cardiac Arrests
79% received intubation 10% BVM 4% Combitube/EOA After adjusting for age, bystander CPR, witnessed arrest and initial rhythm OR for BVM vs Advanced airway was 4.5

30
What is best vascular access?
Goal is vascular access by any means that does not interrupt compressions Preferably rapid reliable access that does not detract from other tasks Based on assumption that the drugs do anything….more on this later IO access can be achieved in < 10 sec but which site should be used?

31
56 (65.9%) used tibial site first
88 Cardiac arrest 56 (65.9%) used tibial site first Initial success rate 89.7% 3 (5.8%) dislodged 18 (34%) used humerus first Initial success rate 60% 6(33%) dislodged Overall success rates Tibia 84.5% Humerus 40%
 used tibial site first. Initial success rate 89.7% 3 (5.8%) dislodged. 18 (34%) used humerus first. Initial success rate 60% 6(33%) dislodged. Overall success rates. Tibia 84.5% Humerus 40%")
32
So what about the drugs? Most recent quandary
Standard of care is currently being challenged Will be a major change in management in your career Who will make the first step…

33
851 patients with OOHCA randomized to:
418 given IV drugs 433 given no drugs Primary outcome hospital discharge Also looked at: Hosp admission with ROSC Neuro outcome at discharge Survival at 1 year

35
Recent epi study

36
Running the Arrest CA is not the most diagnostically challenging condition so thought to be “EASY” EXECUTION is anything but… Conflicting interests of multiple tasks and the need for continuous uninterrupted compressions and infrequent occurence

37
This is harder to do than you think

38
Task Interruptions Airway interventions and IVs Ventilations
Pulse checks Rhythm analysis Defibrillation Changing compressors Patient movement

39
We have limited awareness of task time in complex processes…
We have limited awareness of task time in complex processes….so these interruptions should be engineered and choreographed to minimize their impact…..

40
>20 second pause for defibrillation
>20 second pause for defibrillation. Appears that a ventilation was given before the compressions resumed. Compressions resume 10 seconds after shock delivery.

41
Long pause for ventilations
Long pause for ventilations. Then short sequence of compressions during defib charging. Compressions resumed approximately 5 seconds after shock 1 delivered.

42
Why engineer the process?
Creates uniformity: Accurate assessment of outcomes Linking specific interventions to outcomes Baseline for future modification In the process it: Improves outcomes Improves efficiency Reduces errors

43
Regional Variation in Incidence / Outcome
2008 11,898 cardiac arrests 2729 had initial rhythm of V-Fib / V-Tach. 954 (4.6% of total) were discharged alive. Incidence of EMS-treated CA was 52.1 per survival ranged from 3.0% to 16.3% (median of 8.4%) Median ventricular fibrillation 12.6 per survival ranged from 7.7% to 39.9%,
 were discharged alive. Incidence of EMS-treated CA was 52.1 per survival ranged from 3.0% to 16.3% (median of 8.4%) Median ventricular fibrillation 12.6 per survival ranged from 7.7% to 39.9%,")
44
So how do you control variability

46
Professional CA resuscitation is to CPR …. …
Professional CA resuscitation is to CPR …. ….what a pit crew is to changing tires

47
Pit Crew Model Same name…many versions CPR Controlled ventilations
Maximize compression fraction Effective compression(rate/depth) Provider fatigue Controlled ventilations Defib Emphasis on Shock/Don’t’ shock
 Provider fatigue. Controlled ventilations. Defib. Emphasis on Shock/Don’t’ shock.")
48
Current Goal: Less than 10 second break in every 2 minute cycle of CPR

49
Staying Alive or Another One Bites the Dust?
Staying alive 103 bpm 30:2 100 compressions/min =18s for compressions 5 s break for ventilations every 30 compressions? 18 of every 23s in active compression is 78% NOT counting other breaks in CPR Pit Crew Continuous compressions w/asynchronous ventilation 10s break every 2 min is 92% 5s break every 2 min is 96%

50
Typical example (actually 40:2)
©2010 Paul R. Hinchey

51
Good example of ventilations at a rate of about 8-10 per minute.
©2010 Paul R. Hinchey

52
©2010 Paul R. Hinchey

53
So we went to the simulation lab and now it’s ALL choreographed….

55
BLS & ALS

58
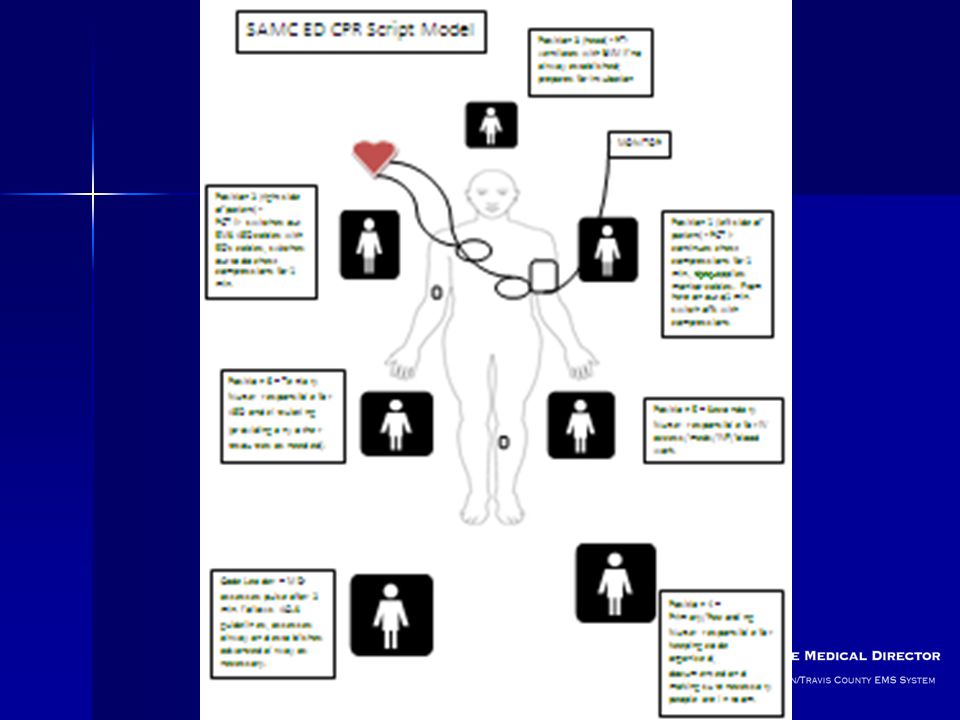
Need cpr checklist ©2010 Paul R. Hinchey

59
Some Scenarios

60
Scenario 1 78 y/o Wal-Mart greeter suffers cardiac arrest in the front of a store: Where do you work the cardiac arrest? Would this be different if it were in his house? When do you begin transport to the hospital? If unsuccessful when do you terminate the resuscitation?

61
Scenario 2 78 y/o Wal-Mart greeter has been resuscitated from CA and is being transported when he re-arrests: What would you instruct your crews to do if they were 20 min out from the hospital? What if they were 5 min out?

62
Scenario 3 78 y/o suffers CA at home. Wife does 2 min dispatcher directed CPR. Pt has ROSC and wakes up. Walks to couch. Crews find in CHF and treat appropriately w/meds and CPAP. FF ride w/crew to hosp. While pulling into ED bay pt goes into CA: What do you want your crews to do?

63
Take Home Message CA is not as easy as once thought
Pre-hospital providers must be the experts Its all about compressions Airway, drugs, etc are a big ? If you want to do this well you must have universally understood goals and plan

64
Post Resuscitation Care

65
Post-Cardiac Arrest Syndrome
Post-cardiac arrest brain injury Responsible for 68% of deaths of patients who survived to ICU admission (Lever, 2004) Post-cardiac arrest myocardial dysfunction LV dysfunction, myocardial stunning, cardiogenic shock Systemic ischemia/reperfusion injury Inflammatory response, impaired vasoregulation, oxygen delivery and utilization, resulting in hypotension / MSOF Persistent precipitating pathology STEMI, Toxic Ingestion, Hypoxia, Hemorrhage, etc. What are the components of mortality in PCAS – Improving hemodynamic status (BP, fluids) and hypothermia impacts all of them. Identifying the STEMI for immediate cath
 Post-cardiac arrest myocardial dysfunction. LV dysfunction, myocardial stunning, cardiogenic shock. Systemic ischemia/reperfusion injury. Inflammatory response, impaired vasoregulation, oxygen delivery and utilization, resulting in hypotension / MSOF. Persistent precipitating pathology. STEMI, Toxic Ingestion, Hypoxia, Hemorrhage, etc. What are the components of mortality in PCAS – Improving hemodynamic status (BP, fluids) and hypothermia impacts all of them. Identifying the STEMI for immediate cath.")
66
Phases of Post-Cardiac Arrest Syndrome

67
Post-Resuscitation Care
Goals of Post-Arrest Care Maintain Hemodynamic Stability Preserve the Brain Avoid hyperventilation Prevent re-arrest Elements of Post-Care include Vasopressor titration Therapeutic Hypothermia Early Cardiac Catheterization Sedation Glucose and Electrolyte Management I still believe there should be some attention paid to ensuring appropriate ventilation. hyperventilation in the patient with myocardial stunning is a double whammy. It is not the primary focus but it can create or worsen a perfusion problem. Please emphasize that the electrolyte management is primarily done in the ICU. To a large extent the issue with glucose is simply avoiding hypoglycemia (for EMS and the ICU) and avoiding hyperglycemia (ICU). I remain amazed at how paramedics take these things and use them as justification to do additional procedures (or at least request them). As you know, several of these post arrest care elements are over a time span that is much longer than the prehospital phase.
 and avoiding hyperglycemia (ICU). I remain amazed at how paramedics take these things and use them as justification to do additional procedures (or at least request them). As you know, several of these post arrest care elements are over a time span that is much longer than the prehospital phase.")
68
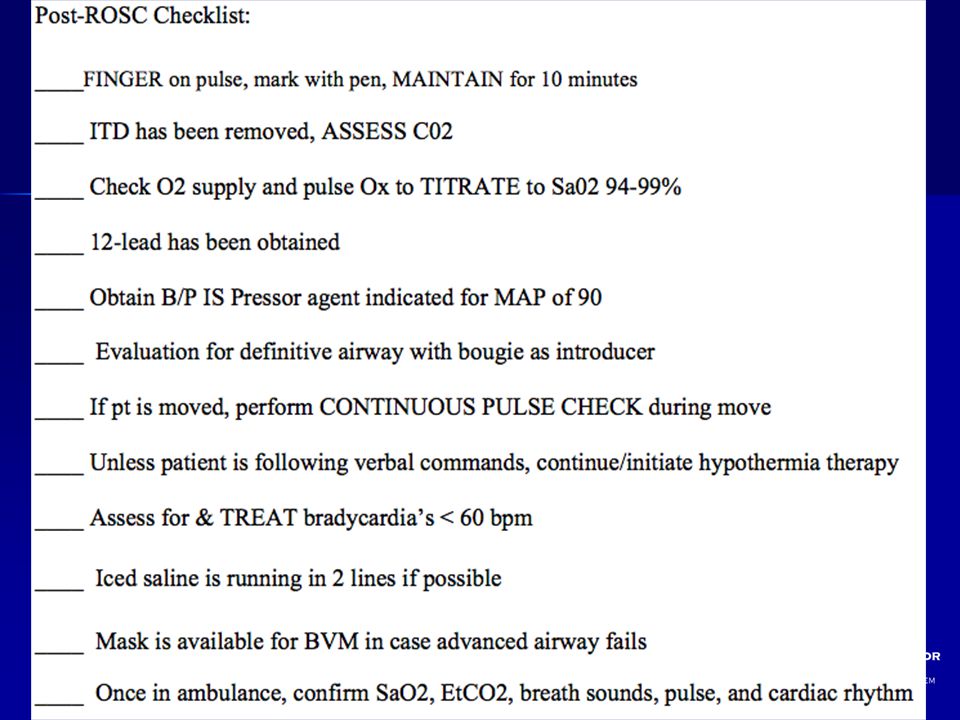
Post Cardiac Arrest Care
The first 20 minutes after ROSC is the Immediate Phase of Post Cardiac Arrest Syndrome Patients in these phases may be critically ill and benefit by immediate treatment AT SCENE: This is a better strategy for patient survival than rapid movement to the vehicle and rapid transport delaying or deferring key interventions Failure to initiate immediate aggressive treatment may result in re arrest of patient or increased morbidity Be sure you place the correct degree of emphasis of time on scene. The time should only be spent to deal with the things you have listed on next slide and should still be kep to a minimum. We are not good keepers of time while we are caring for patients.

69
1,199 Cardiac Arrests ROSC in 27.4% Rearrest in 36% Time to rearrest
Median 3.1 min ( )
")
70
Post-Resuscitation Care
Focus should be on restoring perfusion Perfuse the myocardium Perfuse the brain Fluids and pressors for MAP >90 Remove the ITD Initiate hypothermia Obtain 12 lead EKG THEN move the patient

72
Barriers in Post-Cardiac Arrest Care
Post– cardiac arrest patients are treated by multiple teams of providers Variation in post-cardiac arrest treatment and patient outcome between institutions. Limited reliability of early prognostication (<72 hours after arrest)
")
73
The science behind the cooling
Han Solo frozen in Carbonite – Star Wars Episode V (1980)
")
74
Journal Iowa Medical Society, November 1964

75
Therapeutic Hypothermia
HACA 2002 Bernard 2002 Idrissi 2001

76
ILCOR Advisory Statement
On the strength of these studies, the International Liaison Committee on Resuscitation published recommendations supporting the use of induced hypothermia after resuscitation from cardiac arrest. Given the large numbers of patients suffering cardiac arrest each year, even a small impact in survival and favorable neurologic outcome would lead to important gains for thousands of patients. Unconscious adult patients with ROSC after out-of-hospital VF cardiac arrest should be cooled to 32°C - 34°C for hours Possible benefit for other rhythms or in-hospital cardiac arrest

77
Editorial Comments “The reason hypothermia has not become the standard of care for post-resuscitation is simple. Emergency and EMS physicians have failed to make it so.” Mennegazzi and Callaway, PEC 2005

78
“The Future” 720j Defibrillation? Hands on Defibrillation?
Intra-arrest cooling? Mechanical CPR and AC/DC CPR? Regional Receiving Facilities?

79
Knowledge Gaps Impact of Prehospital Cooling in Outcomes?
Continuous temperature in the Field? Rate of Cooling? Target? How Long? Urban vs. Rural EMS? ALS Vs BLS? How do we train Providers?

80
Take Home Message Resuscitation is not over with ROSC
Post-Cardiac Arrest Patients need to be treated with a high sense of urgency. Patients should receive hypothermia specially if initial rhythm was VF/VT. Hypothermia is not a substitute for other key components in the Chain of Survival

81
Take Home Message Post-resuscitation/cardiac specialty hospitals should receive patients directly from the field or in prompt transfer Coordination between EMS, EM, ICU, and Cardiology is a must!! Engage all stakeholders in your system Management of Cardiac Arrest is evolving rapidly!! EMS Medical Directors must keep up

83
Questions?

84
Jose G. Cabanas MD, MPH / Brent Myers MD, MPH Wake County EMS System
Out-of-Hospital Initiation of Therapeutic Hypothermia with Cold Saline Improves Survival in Patients with Return of Spontaneous Circulation in the Field. Jose G. Cabanas MD, MPH / Brent Myers MD, MPH Wake County EMS System

85
Authors Brent Myers MD, MPH, Wake EMS/WakeMed
Jose G. Cabanas, MD, Wake EMS/WakeMed Ryan Lewis, MS, EMT-P, Wake EMS Valerie De Maio, MD MSc, WakeMed Graham Synder, MD, WakeMed Gay Beneveides, MD, WakeMed Robert Denton, MD, Rex Healthcare Daniel Licastese, RN, Rex Healthcare Robert Lee, MS MA, WakeMed

86
Disclosure This Project was supported by the SAEMS EMS Physio-Control Award (2008)
")
87
Objective To determine the impact on survival of a standard post-resuscitation care protocol that includes prehospital initiation of therapeutic hypothermia in patients with return of spontaneous circulation (ROSC) in the field.
 in the field.")
88
Methods Observational cohort
“Before and after” – Introduction of Therapeutic Hypothermia for patients with prehospital ROSC Post-resuscitation patients are selectively transported to one of 2 high volume PCI centers Wake County NC - pop. 897,000 April 2005 through December 2008

89
Cardiac Arrest Response
All calls receive EMD from a single, high-volume center Fire first response with AED and compressions Paramedic response with transport ambulances (2) Supervisory response at paramedic level
 Supervisory response at paramedic level.")
90
Protocol Revision [Apr 2005-Oct 2006]: Continuous compressions, controlled ventilations [Oct 2006-Dec 2008]: Induced Hypothermia after ROSC
![Protocol Revision [Apr 2005-Oct 2006]: Continuous compressions, controlled ventilations.](http://slideplayer.com/slide/3854662/13/images/90/Protocol+Revision+%5BApr+2005-Oct+2006%5D%3A+Continuous+compressions%2C+controlled+ventilations..jpg "[Oct 2006-Dec 2008]: Induced Hypothermia after ROSC.")
91
Criteria for Induced Hypothermia
ROSC after cardiac arrest not related to trauma or hemorrhage Age 16 years or greater Female without obviously gravid uterus Initial temperature >34 C Patient with advanced airway (no RSI) Patient remains comatose without purposeful response to pain
 Patient remains comatose without purposeful response to pain.")
92
Data Collection All EMS records are maintained in an electronic database Records with any of the following characteristics are reviewed to determine if cardiac arrest occurred: EMS Patient Disposition = cardiac arrest CPR procedure is recorded Defibrillation is recorded Induced Hypothermia Procedure

93
Inclusion Criteria All adult patients resuscitated from out of hospital cardiac arrest (OHCA) prior to hospital arrival, regardless of initial rhythm, were included if they had ROSC in the field.
 prior to hospital arrival, regardless of initial rhythm, were included if they had ROSC in the field.")
94
Exclusion Criteria Age less than 16 Obvious traumatic origin of arrest
EMS witnessed arrest Arrest not in EMS control Prison facilities Out-of-system intercept Arrests under direction of non-EMS physician

95
Outcome Measures Discharge from hospital (primary)
Neurologically intact survival was defined as CPC 1 or 2 at time of hospital discharge. 2 blinded physician reviewers from each hospital independently assigned CPC scores based on patient discharge records

96
Included Patients / Phase
All Phases N=640 Before (17 Months) 227 After (26 Months) 413
 227. After (26 Months) 413.")
97
Patient and EMS Characteristics
Before After (n=227) (n=413) Mean age (yrs) 66 64 Male sex 62% 60% Bystander witnessed arrest 45% 32% Bystander CPR 38% 39% Mean Response (mins) 5.6 Initial rhythm VF/VT 35% NOTE: no statistically significant difference between study periods
 (n=413) Mean age (yrs) Male sex. 62% 60% Bystander witnessed arrest. 45% 32% Bystander CPR. 38% 39% Mean Response (mins) 5.6. Initial rhythm VF/VT. 35% NOTE: no statistically significant difference between study periods.")
98
Multivariate Odds of Neuro Intact Survival
Factor Odds 95% CI Age 0.97 Bystander CPR 1.44 Vfib 8.58 Hypothermia (After) 1.95
")
99
Survival to Hospital Discharge for All Rhythms
NOTE: statistically significant difference p value <0.0163

100
Survival to Hospital Discharge for All Rhythms
*Difference in overall survival was significant with a p-value of

101
Percent of Survivors Neurologically Intact
NOTE: no statistically significant difference between study periods

102
Limitations Protocol-driven pre- and post-resuscitation cardiac arrest care Hawthorne effect Intention-to-treat analysis

103
Conclusion Out-of-hospital standard post-resuscitation care protocol that includes induced hypothermia for all patients with ROSC significantly improved survival to hospital discharge in this EMS system

105
Wake County EMS Annually 70,000+ 911 calls (700 OHCA)
Providers: 1,500 BLS, 225 ALS, 17 APPs Tiered response incl. dispatch assisted CPR, first responder apparatus and paramedic supervisor to high acuity calls Serve 7 hospitals of 3 health care systems, incl. 2 PCI capable facilities Annual protocol updates in April Utstein style data collection template

106
Survival to Discharge – VF/VT
NOTE: no statistically significant difference between study periods

107
Optimizing Neurologic Resuscitation
Mild Induced Hypothermia (IH) Decrease metabolic demand4,5,6,7 Inhibits inflammatory cascade12,14,15 IH is time sensitive8,11,14,15 Hemodilution12,13 Normal saline dilution as part of hypertensive reperfusion strategy Hypertensive reperfusion Use of vasopressors to target MAP of 90 Key characteristic of the post resuscitation syndrome is loss of cerebral autoregulaion. Healthy brain maintains global CBF of 50 mL per 100g of brain tissue per minute within a cerebral perfusion pressure range of mmHg. When cerebral perfusion pressure drops below 50 mmHg there is reduced flow. Brain may be able to tolerate CBF of as low as 10% of normal but trickle flow <10% may be worse than no flow.(see persse for description.) Induced hypothermia appears to be time sensitive. In rat studies delays > 45 min resulted in loss of benefit. (Markarian GZ, et al. Mild hypothermia:therapeutic window after experimental cerebral ischemia. Neurosurgery 1996, 38: ) In dogs delaying hypothermia by 15 minutes obscured the benefit in functional outcome as compared with that with immediate hypothermia. (Kuboyama)
 Decrease metabolic demand4,5,6,7. Inhibits inflammatory cascade12,14,15. IH is time sensitive8,11,14,15. Hemodilution12,13. Normal saline dilution as part of hypertensive reperfusion strategy. Hypertensive reperfusion. Use of vasopressors to target MAP of 90. Key characteristic of the post resuscitation syndrome is loss of cerebral autoregulaion. Healthy brain maintains global CBF of 50 mL per 100g of brain tissue per minute within a cerebral perfusion pressure range of mmHg. When cerebral perfusion pressure drops below 50 mmHg there is reduced flow. Brain may be able to tolerate CBF of as low as 10% of normal but trickle flow <10% may be worse than no flow.(see persse for description.) Induced hypothermia appears to be time sensitive. In rat studies delays > 45 min resulted in loss of benefit. (Markarian GZ, et al. Mild hypothermia:therapeutic window after experimental cerebral ischemia. Neurosurgery 1996, 38: ) In dogs delaying hypothermia by 15 minutes obscured the benefit in functional outcome as compared with that with immediate hypothermia. (Kuboyama)")
108
Circulation 2007

109
Standardized post resuscitation bundle:
Cardiac catheterization Therapeutic hypothermia Hemodynamic maintenance Ventilator management Electrolyte/glucose control Prognostication n

110
Outcome –CPC 1 or 2 Control period 15/58 (26%) Treatment period 34/61(56%) OR (CI , p=0.001)
 Treatment period 34/61(56%) OR 3.61 (CI , p=0.001)")
111
Induced Hypothermia Do NOT delay starting IH
If patient meets inclusion criteria start cooling Do not worry about rewarming

113
?

114
So if compressions are the MOST important intervention for a successful resuscitation what is our airway management device of choice in a cardiac arrest? ….more on this later

115
Ventilation vs Oxygenation
Oxygenation is delivery of oxygen to RBC and tissues Oxygenation determined by two things: FiO2 (% inspired O2) Pressure of gas (CPAP or PEEP) Ventilation is the elimination of CO2 Ventilation is determined by two things: Tidal volume Ventilatory rate
 Pressure of gas (CPAP or PEEP) Ventilation is the elimination of CO2. Ventilation is determined by two things: Tidal volume. Ventilatory rate.")
116
Why is this important? Cells require oxygen to make energy
Inability to oxygenate the tissue is quickly fatal Exchanging carbon dioxide is NOT! If forced to make the choice between oxygenation and CO2 exchange CHOOSE OXYGENATION!

117
So why does that matter? If oxygenation has nothing to do with ventilation why do we ventilate patients at rates > 30 breaths per minute? Who cares…..if breathing 12 times a minute is good 30 times a minute MUST be better right?

118
….what is our airway management device of choice in a cardiac arrest?

119
The device that allows us to oxygenate the patients brain and myocardium and causes the… LEAST interruption in compressions

120
Objective Describe the importance of:
Prehospital resuscitation Continuous compression Controlled ventilatory rates Describe the value and limitations of advanced airway management adjuncts List the critical components of cardiac arrest management

121
Pit Crew CPR Went to simulation to design highly scripted process that allows intervention without interruption Tasks assigned to positions rather than individuals because individuals change

122
OOHCA What matters! For first 2 cycles concentrate on compressions
Get on the chest as quick as possible Compress hard and fast (do NOT exceed 120) Minimize interruptions If on monitor compress up to delivery of shock Resume compressions immediately regardless of pulse or rhythm BVM ONLY Control ventilation (use your blinky light)
 Minimize interruptions. If on monitor compress up to delivery of shock. Resume compressions immediately regardless of pulse or rhythm. BVM ONLY. Control ventilation (use your blinky light)")
123
OOHCA What matters! After 2 cycles (4 min) place King Airway
Don’t stop compressions! ETI only if unsuccessful with BIAD Place gastric tube via KING or OG/NG Control your ventilations Recheck tube with each patient movement

124
OOHCA What matters! Continue resuscitation
Rhythm/Pulse check only at 2 min Change compressor q 1 min regardless of fatigue Run checklist to assure overlooked errors Careful consideration of causes Do NOT move the patient unless: You are in potential danger You are in a public place Other situation not suitable to leave the body

125
Pre-hospital providers must be the experts in cardiac arrest resuscitation!

126
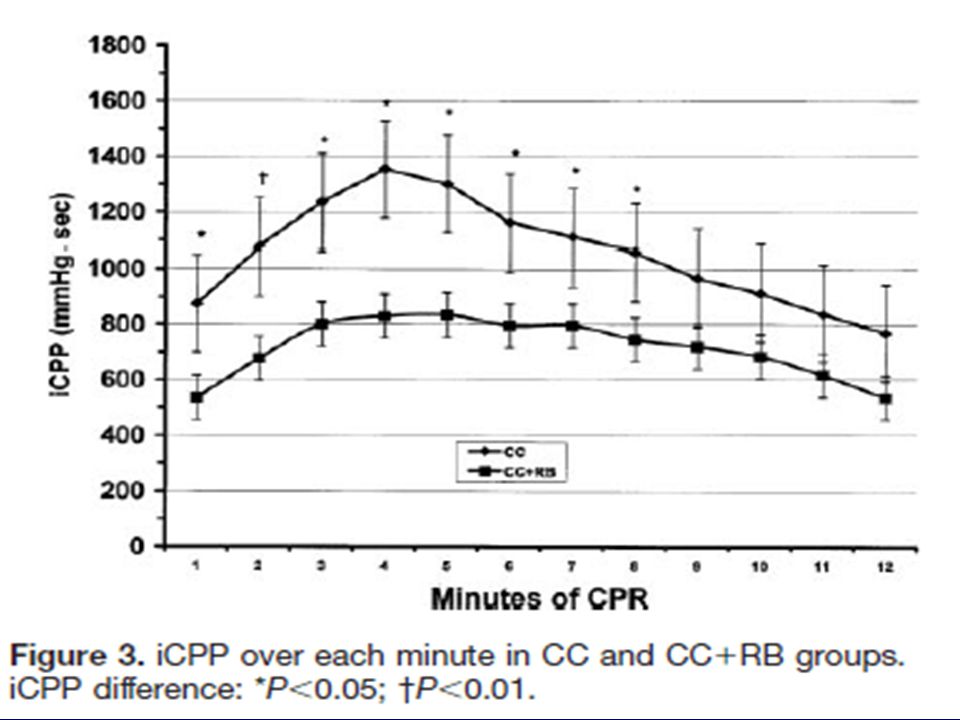
What we know? Metabolic Phase 2 4 6 8 10 12 14 16 18 20 Electric
2 4 6 8 10 12 14 16 18 20 Arrest Time (min) SHOCK CCC HYPO? Electric Circulatory Phase Etapa metabólica Metabolic Phase
 SHOCK. CCC. HYPO Electric. Circulatory Phase. Etapa metabólica. Metabolic Phase.")
127
Background

128
Inertia….. it’s not just for cars anymore!
Blood Inertia? Berg et al. Resuscitation 2001

129
What is Post-Cardiac Arrest Syndrome?
Unique / complex combination of pathophysiological processes, which include: Post–cardiac arrest brain injury, Post–cardiac arrest myocardial dysfunction Systemic ischemia/reperfusion response. DON’T FORGET!! the unresolved pathological process that caused the cardiac arrest.

130
Post-Cardiac Arrest Syndrome
High mortality of cardiac arrest patients after ROSC is due to multiple organ system dysfunction Cardiac Arrest etiology Duration of cardiac arrest and no flow Reperfusion injury after ROSC High mortality in post-cardiac arrest is related to MOSF – Especially cardiovascular and neurological collapse (brain injury)
")
131
Post-Cardiac Arrest Brain Injury
Pathophysiology Impaired Cerebral Autoregulation Cerebral Edema Clinical Manifestations Coma, Seizures, Myoclonus Vegetative State, Brain Death, Strokes Potential Treatments Therapeutic Hypothermia Early Hemodynamic Optimization Ventilation/ Oxygenation I don’t think airway is the best term. Shouldn’t this be ventilation / oxygenation?

132
Did Rate Change with Feedback?
Independent Variables (Not Paired) Scene Kruskal-Wallis Test P = 0.25 Transport P = 0.39* Independent groups and not paired – so use Kruskal Wallis Test (non-parametric)
 Scene. Kruskal-Wallis Test. P = Transport. P = 0.39* Independent groups and not paired – so use Kruskal Wallis Test (non-parametric)")
133
Post-Cardiac Arrest Myocardial Dysfunction
Pathophysiology Global Hypokinesis ACS Clinical Manifestations Reduced Cardiac Output (Low BP) Dysrhythmias Cardivascular Collapse Potential Treatments Early Revascularization (AMI) Hemodynamic Optimization
 Dysrhythmias. Cardivascular Collapse. Potential Treatments. Early Revascularization (AMI) Hemodynamic Optimization.")
134
Systemic Ischemia/ Reperfusion Response
Pathophysiology Systemic Inflammatory Response Increased Coagulation Adrenal Suppression Key Potential Treatments Temperature Control Hemodynamic Optimization Glucose Control Treat Cause of Arrest

135
Aha statement Post-Resuscitation Recommendations Induced hypothermia
Prevention of hyperthermia Tight glucose control Prevent hypocapnia Maintain elevated MAP

136
Therapeutic Hypothermia
The protective effects of hypothermia induction have been suggested since the time of Hippocrates, who advocated packing bleeding patients in snow. Baron Larrey, Napoleon’s Battle surgeon during the invasion of Russia had noted that soldiers that were left in the snow had improved survival than those treated with blankets and warm drinks.

137
History of Hypothermia and Cardiac Arrest
Williams et al -Annals of Surgery, Volume 4 #3 September 1958

138
Why Induced Hypothermia?
Pre-hospital ROSC1 45%(38%) of v-fib arrests 37% (22%)of all cardiac arrests Discharge1 12%(10%) Post Resuscitation Deaths3 10% die due to recurrent dysrhythmias 30% die to due to cardiovascular collapse 40% die due to PRE
 of v-fib arrests. 37% (22%)of all cardiac arrests. Discharge1. 12%(10%) Post Resuscitation Deaths3. 10% die due to recurrent dysrhythmias. 30% die to due to cardiovascular collapse. 40% die due to PRE.")
139
Mechanisms of Hypothermia
In the normal brain, hypothermia reduces the cerebral metabolic rate for oxygen (CMRO2) by 6% for every 1°C reduction in brain temperature It is thought to suppress many of the chemical reactions associated with reperfusion injury. (free radical, excitatory amino acid release, and calcium shifts, which can in turn lead to mitochondrial damage and apoptosis Steen PA, Newberg L, Milde JH, et al. Hypothermia and barbiturates: individual and combined effects on canine cerebral oxygen consumption. Anesthesiology. 1983;58:527–532.
 by 6% for every 1°C reduction in brain temperature. It is thought to suppress many of the chemical reactions associated with reperfusion injury. (free radical, excitatory amino acid release, and calcium shifts, which can in turn lead to mitochondrial damage and apoptosis. Steen PA, Newberg L, Milde JH, et al. Hypothermia and barbiturates: individual and combined effects on canine cerebral oxygen consumption. Anesthesiology. 1983;58:527–532.")
140
Post Resuscitation Encephalopathy
Initial insult from cardiac arrest Period of luxuriant hyperperfusion3 Cell injury8,11 Oxygen free radical formation Inflammatory cascade Glutamate mediated cell death Loss of autoregulation Sludging and hypoperfusion3,8,11 Perfusion/demand mismatch8,11 PRE 38%; recalcitrant ventricular dysrhythmias 10%; continued low cardiac output states 31%) see myerburg for best review of path Inflammatory cascade: ischemia causes outpouring of excitotoxic glutimate which in turn activates nmda and ampa receptors. This causes calcium and sodium channels open initiating enzymatic induced neuronal death. Particularly vulnerable are the hippocampus, cerebellum, frontoparietal cortex and basal ganglia. Cerebral perfusion problems occur in 4 phases.(see persse,D Manging the post reuscitation patient in the field for the review) 1. Multifocal no reflow occurs immediately and seems to be readily overcome by normotensive or hypertensive reperfusion. 2. Transient global reactive hyperemia lasting minutes. 3. Delayed, prolonged global and multifocal hypoperfusion begins about two hrs after circulation is restored leading to a decrease in blood flow of up to 50% because of loss of autoregulation. Meanwhile cerebral oxygen consumption returns to baseline or above baseline values leading to mismatch of oxygen delivery and uptake. 4. late resolution is the return to normal ccbf and consumption or in the case of brain death the abnormal flow and consumption persist. Note sludging of the blood contributes to the no-reflow phenomenon. Hemodilution has been shown to be effective in increasing cerebral blood flow. After initial period of hyperemia the dysregulation results in CBF as low as 50% of normal while cerebral metabolic ocygen consumption returns to or above baseline creating a mismatch of ocygen delivery and uptake(persse)
 see myerburg for best review of path. Inflammatory cascade: ischemia causes outpouring of excitotoxic glutimate which in turn activates nmda and ampa receptors. This causes calcium and sodium channels open initiating enzymatic induced neuronal death. Particularly vulnerable are the hippocampus, cerebellum, frontoparietal cortex and basal ganglia. Cerebral perfusion problems occur in 4 phases.(see persse,D Manging the post reuscitation patient in the field for the review) 1. Multifocal no reflow occurs immediately and seems to be readily overcome by normotensive or hypertensive reperfusion. 2. Transient global reactive hyperemia lasting minutes. 3. Delayed, prolonged global and multifocal hypoperfusion begins about two hrs after circulation is restored leading to a decrease in blood flow of up to 50% because of loss of autoregulation. Meanwhile cerebral oxygen consumption returns to baseline or above baseline values leading to mismatch of oxygen delivery and uptake. 4. late resolution is the return to normal ccbf and consumption or in the case of brain death the abnormal flow and consumption persist. Note sludging of the blood contributes to the no-reflow phenomenon. Hemodilution has been shown to be effective in increasing cerebral blood flow. After initial period of hyperemia the dysregulation results in CBF as low as 50% of normal while cerebral metabolic ocygen consumption returns to or above baseline creating a mismatch of ocygen delivery and uptake(persse)")
141
Wake EMS Experience…

142
Objective To determine the impact on survival of a standard post-resuscitation care protocol that includes prehospital initiation of therapeutic hypothermia in patients with return of spontaneous circulation (ROSC) in the field.
 in the field.")
143
Methods Observational cohort
“Before and after” – Introduction of Therapeutic Hypothermia for patients with prehospital ROSC Post-resuscitation patients are selectively transported to one of 2 high volume PCI centers Wake County NC - pop. 897,000 April 2005 through December 2008

144
Cardiac Arrest Response
All calls receive EMD from a single, high-volume center Fire first response with AED and compressions Paramedic response with transport ambulances (2) Supervisory response at paramedic level
 Supervisory response at paramedic level.")
145
Protocol Revision [Apr 2005-Oct 2006]: Continuous compressions, controlled ventilations [Oct 2006-Dec 2008]: Induced Hypothermia after ROSC
![Protocol Revision [Apr 2005-Oct 2006]: Continuous compressions, controlled ventilations.](http://slideplayer.com/slide/3854662/13/images/145/Protocol+Revision+%5BApr+2005-Oct+2006%5D%3A+Continuous+compressions%2C+controlled+ventilations..jpg "[Oct 2006-Dec 2008]: Induced Hypothermia after ROSC.")
146
Criteria for Induced Hypothermia
ROSC after cardiac arrest not related to trauma or hemorrhage Age 16 years or greater Female without obviously gravid uterus Initial temperature >34 C Patient with advanced airway (no RSI) Patient remains comatose without purposeful response to pain
 Patient remains comatose without purposeful response to pain.")
147
Data Collection All EMS records are maintained in an electronic database Records with any of the following characteristics are reviewed to determine if cardiac arrest occurred: EMS Patient Disposition = cardiac arrest CPR procedure is recorded Defibrillation is recorded Induced Hypothermia Procedure

148
Inclusion Criteria All adult patients resuscitated from out of hospital cardiac arrest (OHCA) prior to hospital arrival, regardless of initial rhythm, were included if they had ROSC in the field.
 prior to hospital arrival, regardless of initial rhythm, were included if they had ROSC in the field.")
149
Exclusion Criteria Age less than 16 Obvious traumatic origin of arrest
EMS witnessed arrest Arrest not in EMS control Prison facilities Out-of-system intercept Arrests under direction of non-EMS physician

150
Outcome Measures Discharge from hospital (primary)
Neurologically intact survival was defined as CPC 1 or 2 at time of hospital discharge. 2 blinded physician reviewers from each hospital independently assigned CPC scores based on patient discharge records

151
Included Patients / Phase
All Phases N=640 Before (17 Months) 227 After (26 Months) 413
 227. After (26 Months) 413.")
152
Patient and EMS Characteristics
Before After (n=227) (n=413) Mean age (yrs) 66 64 Male sex 62% 60% Bystander witnessed arrest 45% 32% Bystander CPR 38% 39% Mean Response (mins) 5.6 Initial rhythm VF/VT 35% NOTE: no statistically significant difference between study periods
 (n=413) Mean age (yrs) Male sex. 62% 60% Bystander witnessed arrest. 45% 32% Bystander CPR. 38% 39% Mean Response (mins) 5.6. Initial rhythm VF/VT. 35% NOTE: no statistically significant difference between study periods.")
153
Survival to Hospital Discharge for All Rhythms
NOTE: statistically significant difference p value <0.0163

154
Survival to Hospital Discharge for All Rhythms
*Difference in overall survival was significant with a p-value of

155
Percent of Survivors Neurologically Intact
NOTE: no statistically significant difference between study periods

156
Limitations Protocol-driven pre- and post-resuscitation cardiac arrest care Hawthorne effect Intention-to-treat analysis

157
Conclusion Out-of-hospital standard post-resuscitation care protocol that includes induced hypothermia for all patients with ROSC significantly improved survival to hospital discharge in this EMS system

158
Optimizing Neurologic Resuscitation
Mild Induced Hypothermia (IH) Decrease metabolic demand4,5,6,7 Inhibits inflammatory cascade12,14,15 IH is time sensitive8,11,14,15 Hemodilution12,13 Normal saline dilution as part of hypertensive reperfusion strategy Hypertensive reperfusion Use of vasopressors to target MAP of 90 Key characteristic of the post resuscitation syndrome is loss of cerebral autoregulaion. Healthy brain maintains global CBF of 50 mL per 100g of brain tissue per minute within a cerebral perfusion pressure range of mmHg. When cerebral perfusion pressure drops below 50 mmHg there is reduced flow. Brain may be able to tolerate CBF of as low as 10% of normal but trickle flow <10% may be worse than no flow.(see persse for description.) Induced hypothermia appears to be time sensitive. In rat studies delays > 45 min resulted in loss of benefit. (Markarian GZ, et al. Mild hypothermia:therapeutic window after experimental cerebral ischemia. Neurosurgery 1996, 38: ) In dogs delaying hypothermia by 15 minutes obscured the benefit in functional outcome as compared with that with immediate hypothermia. (Kuboyama)
 Decrease metabolic demand4,5,6,7. Inhibits inflammatory cascade12,14,15. IH is time sensitive8,11,14,15. Hemodilution12,13. Normal saline dilution as part of hypertensive reperfusion strategy. Hypertensive reperfusion. Use of vasopressors to target MAP of 90. Key characteristic of the post resuscitation syndrome is loss of cerebral autoregulaion. Healthy brain maintains global CBF of 50 mL per 100g of brain tissue per minute within a cerebral perfusion pressure range of mmHg. When cerebral perfusion pressure drops below 50 mmHg there is reduced flow. Brain may be able to tolerate CBF of as low as 10% of normal but trickle flow <10% may be worse than no flow.(see persse for description.) Induced hypothermia appears to be time sensitive. In rat studies delays > 45 min resulted in loss of benefit. (Markarian GZ, et al. Mild hypothermia:therapeutic window after experimental cerebral ischemia. Neurosurgery 1996, 38: ) In dogs delaying hypothermia by 15 minutes obscured the benefit in functional outcome as compared with that with immediate hypothermia. (Kuboyama)")
159
Is Earlier Better?? Nordmark 2005
20 Pigs Subjected to 8 minutes of V-fib followed by CPR Randomized into 2 groups (hypothermia/control) Hypothermic group received cold saline after 1 min in CPR Conclusion: “Inducing Therapeutic Hypothermia with a cold infusion seems to be an effective method that can be started during ongoing CPR”
 Hypothermic group received cold saline after 1 min in CPR. Conclusion: Inducing Therapeutic Hypothermia with a cold infusion seems to be an effective method that can be started during ongoing CPR")
160
Is Earlier Better?? Bernard 2008 Resuscitation
60 year-old female in cardiac arrest (37 minutes) due to pericardial tamponade D/H Alert and Oriented Conclusion: “Treatment with a rapid Intravenous Infusion of large volume (40ml/kg), Ice-cold (4˚C) fluid during CPR induces mild hypothermia and may provide neurological protection”
 due to pericardial tamponade. D/H Alert and Oriented. Conclusion: Treatment with a rapid Intravenous Infusion of large volume (40ml/kg), Ice-cold (4˚C) fluid during CPR induces mild hypothermia and may provide neurological protection")
161
Is Pre-Hospital Cooling Safe??
Bruel 2008 The study was aimed to determine the safety and effectiveness of cooling patients while in ALS Support The Median time to reach mil hypothermia (<34˚C) after ROSC was 16 minutes Conclusion: “The infusion of 2 liters of Normal Saline at 4˚C in the field during ALS to induce mild hypothermia in resuscitated OHCA patients is safe, feasible and effective”
 after ROSC was 16 minutes. Conclusion: The infusion of 2 liters of Normal Saline at 4˚C in the field during ALS to induce mild hypothermia in resuscitated OHCA patients is safe, feasible and effective")
Similar presentations





















 Medical Incident Report Form Education Module for 2009.>")


>")

