Download presentation
Presentation is loading. Please wait.

1
Jim McManus Director of Public Health Working with the new Public Health Arrangements Chartered Society of Physiotherapy 18 th September

2
What’s in a name? “the science and art of preventing disease, prolonging life and promoting, protecting and improving health through the organised efforts of society” Sir Donald Acheson, 1988 “Decency, Freedom from infection, Labour, Dignity” Sir Alfred Hill, President of the Society of Medical Officers of Health, 1866-1903

3
1 st – Poverty, Living Conditions (Up to 1900) ◦ Improvement in incomes, reduction in deaths 2 nd –Communicable Diseases (Up to 1950s) ◦ Now on average 6-11% of deaths in UK. Was 85% of deaths before 1900 3 rd – Non-Communicable Diseases (Today) ◦ Over 60% of deaths due to lifestyle and behaviour ◦ Poorest fare worst (smoking, diabetes, heart disease)
 ◦ Over 60% of deaths due to lifestyle and behaviour ◦ Poorest fare worst (smoking, diabetes, heart disease).")
4
Contributors to overall health outcomes Have changed over time Smoking 10% Diet/Exercise 10% Alcohol use 5% Poor sexual health 5% Health Behaviours 30% Education 10% Employment 10% Income 10% Family/Social Support 5% Community Safety 5% Socioeconomic Factors 40% Access to care 10% Quality of care 10% Clinical Care 20% Environmental Quality 5% Built Environment 5% Built Environment 10% Source: Robert Wood Johnson Foundation and University of Wisconsin Population Health Institute. Used in US to rank counties by health status While this is from a US context it does have significant resonance with UK Evidence, though I would want to increase the contribution of housing to health outcomes from a UK perspective.

5
Policy History...Zzzzz Chadwick Aneurin Bevan Black Report 1982 (UK) Ottawa Charter 1986 (World) Health of the Nation 1984 (England & Wales) Our Healthier Nation 1998 (England & Wales) Healthier Wales 2000 (Wales) Choosing Health 2005 (England) WHO Commission on Social Determinants 2009 Marmot Review of Health Inequalities 2010
 Ottawa Charter 1986 (World) Health of the Nation 1984 (England & Wales) Our Healthier Nation 1998 (England & Wales) Healthier Wales 2000 (Wales) Choosing Health 2005 (England) WHO Commission on Social Determinants 2009 Marmot Review of Health Inequalities 2010")
6
The Technology that is Public Health Outcomes Art Science

7
The Domains of Public Health Health Improvement Health Protection Service Quality Then & Now Sanitation Housing Now Environment Then & Now Smoking Heart Disease Now Care which keeps People healthy and independent

8
Key Point As the factors and services behind health in the UK improved, key public health contributions became mainstream parts of the local government day job (sanitation, housing, school meals) How do we work with the new day job?
 How do we work with the new day job")
9
The Health and Social Care Act 2012 Specialist public health is multidisciplinary Most public health coming to LAs in 2013 / 2015 Some going to NHS Commissioning Board National Agency Public Health England Health and Wellbeing Boards

10
Statute and guidance Boards of commissioners Provider and district engagement left open Roadmap of JSNA to Commissioning Plans Unlikely CSP or Physios will be given membership per se but each Board is different Constitutional anomaly – officers as members

11
Influence DPH and lead elected Members Work with CCGs directly Where can you add value? ◦ Prevention ◦ Long term conditions ◦ Working age adults ◦ Frail elderly Expect JSNA and Strategy and Commissioning Plans to reflect your contribution rather than a seat on the Board Provider Fora?

12
Specialist / Wider Public Health Specialist High level of training in a technical public health function, largely defined by legislation or policy in West Application of technical and specialist skills to the three domains of public health Health Improvement Health Protection Service Quality

13
Mechanisms Policy Mechanisms ◦ Marmot, JSNA, Health and Wellbeing Board Commissioning Mechanisms ◦ Applying specialist skills to commissioning ◦ Invest in the right things Delivery Mechanisms ◦ Mainstream public health – everyone provider or citizens understands their contribution

14
Timeframes of impact/yield Years 0151015 Planning Education Vitamin Supplements Air Pollution Decent Homes Jobs Primary Care 20 CVD Events Self Care Vitamin D and TB Rickets CVD Events Acute Bronchitis Admissions Respiratory Mental Health overcrowding educational attainment Life Expectancy Healthier space useChanging culture of activity Life ExpectancyMental Health

15
Public Health Input into the Commissioning Cycle Monitor/ Evaluate Plan Review Need for Service and Effectiveness of existing services Contract/Deliv er Public Health Input into the Commissioning Cycle. Can be throughout or can be on specific areas playing to the PH strengths Community Engagement Support in establishing meaningful indicators of delivery and outcome Model whether need will Be met by proposed volume Check whether plans equate To evidence and need and Test for equity / inequity Support and advise on Evaluation and conduct Bits of it if enough resource Needs Assessments Equity Auditing Evidence of Effectiveness Health Impact Assessment Triangle of critical influence – where public health should be most visible

16
Investing in the Right Things Our Burden of Disease is not the right way round Primary Prevention Secondary Prevention Tertiary Prevention System Failure

17
Health and Care: Our Burden of Disease is not the right way round Primary Prevention Secondary Prevention Tertiary Prevention The shift to prevention

18
Understanding key drivers of health and wellbeing, and interventions to improve population health Structured ways of doing needs analysis Decision analysis and helping with economic analyses of policy to help setting outcomes Supporting the understanding of complex variables and their interaction in policy and decision making

19
Resource allocation for policy and interventions Understanding targeting action and interventions to bring most benefit Understanding and manage the conflicts between population and individual concerns (equity) Finding, assessing and applying evidence Supporting effective commissioning using 1,2 and 3 above Evaluation of commissioning against desired outcomes
 Finding, assessing and applying evidence Supporting effective commissioning using 1,2 and 3 above Evaluation of commissioning against desired outcomes")
20
1. Commission for the whole person’s lived experience (housing, volunteering, leisure, transport,) 2. See Potentials not Problems, assets as well as needs 3. Transformation of current system through staged redesign to preventive and early intervention 4. Subsidiarity and Access 5. Co-production 6. Behavioural Sciences 7. Pathwayed
 2. See Potentials not Problems, assets as well as needs 3. Transformation of current system through staged redesign to preventive and early intervention 4. Subsidiarity and Access 5. Co-production 6. Behavioural Sciences 7. Pathwayed.")
21
Making this lot work Burden of avoidable ill-health Demographic and growing demands Benefits to citizens Preventing service use Moves people into self-care We cannot afford the coming time bomb Justice and fairness are public health values The DPH’s concerns…

22
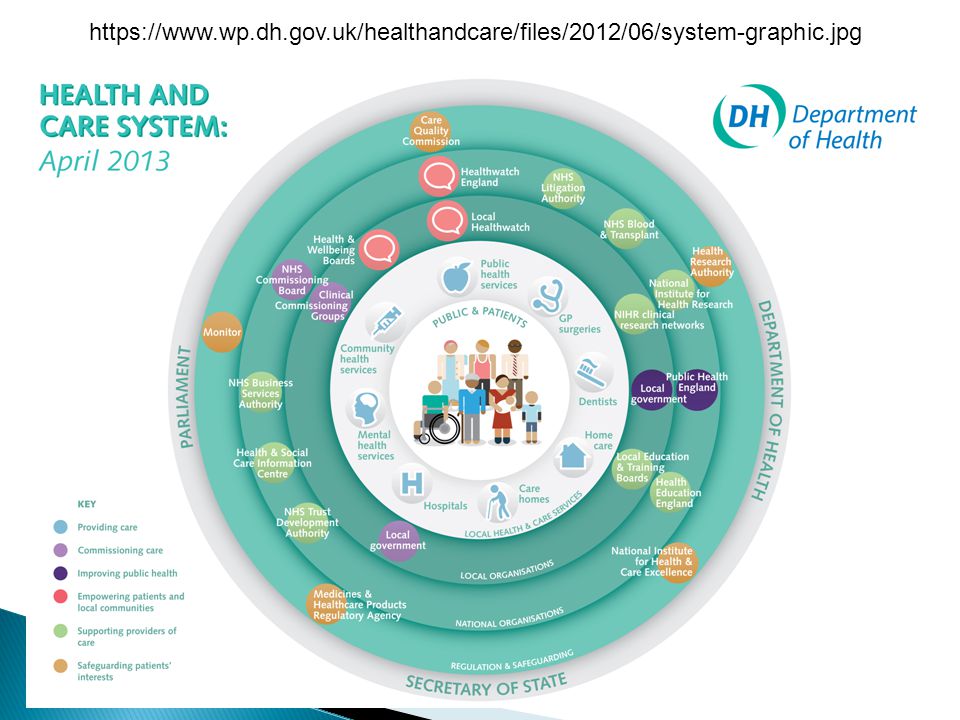
https://www.wp.dh.gov.uk/healthandcare/files/2012/06/system-graphic.jpg
Similar presentations



















