Download presentation
Presentation is loading. Please wait.

2
BIKHA Prof. Bikha Ram Devrajani FCPS,FACP, FRCP Professor Medicine& Director MRC Liaquat University of Medical & Health Sciences Jamshoro

3
PAROXYSMAL EXCESSIVE NEURONAL DISCHARGE CORTICAL/SUBCORTICAL STRUCTURES CLINICAL DEFINITION: Abrupt onset and end of one or more of the following; 1. Disconnection/Loss of consciousness. 2. Loss of postural control. 3. Motor, sensory or psychic symptoms. 4. Autonomic dysfunction. DEFINITION OF EPILEPSY

4
BIKHA

9
CLASSIFICATION OF SEIZURE TYPES Partial seizures. - Simple Partial - Complex partial Generalized seizures - Tonic clonic - Absence - Myoclonic, tonic, atonic Secondarily generalized seizures

10
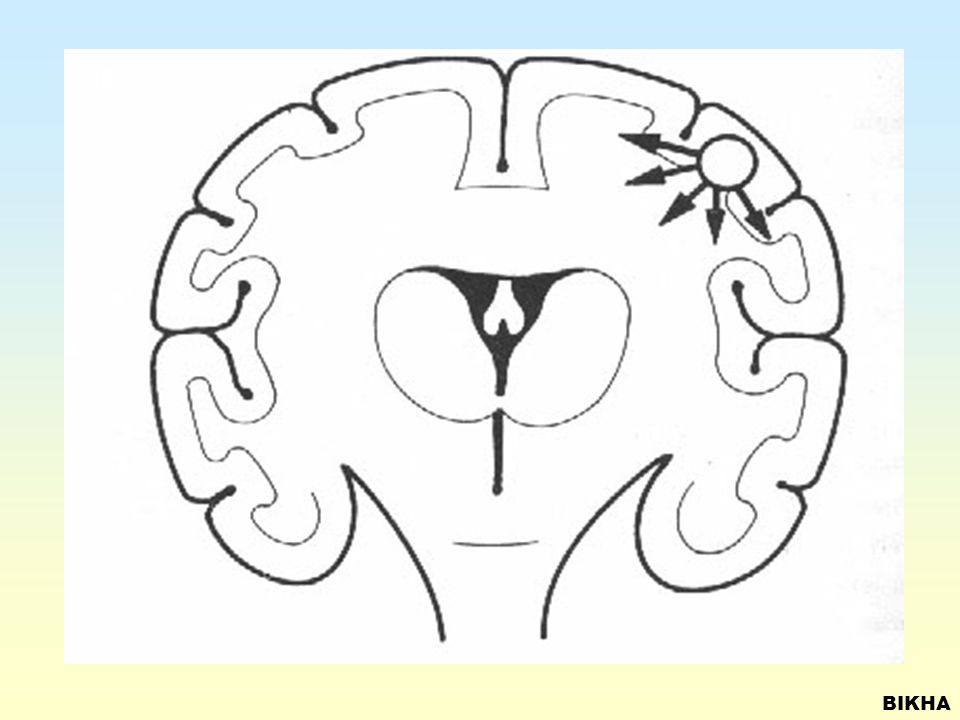
BIKHA SIMPLE PARTIAL SEIZURES Focus - Central

11
BIKHA

12
SIMPLE PARTIAL SEIZURES Focus – Left Central

13
BIKHA

14
SIMPLE PARTIAL SEIZURES Focus – Occipital

15
BIKHA

16
COMPLEX PARTIAL SEIZURES Temporal lobe

17
BIKHA

18
COMPLEX PARTIAL SEIZURES Focus - Temporal

19
BIKHA

20
COMPLEX PARTIAL SEIZURES Parietal lobe

21
BIKHA

22
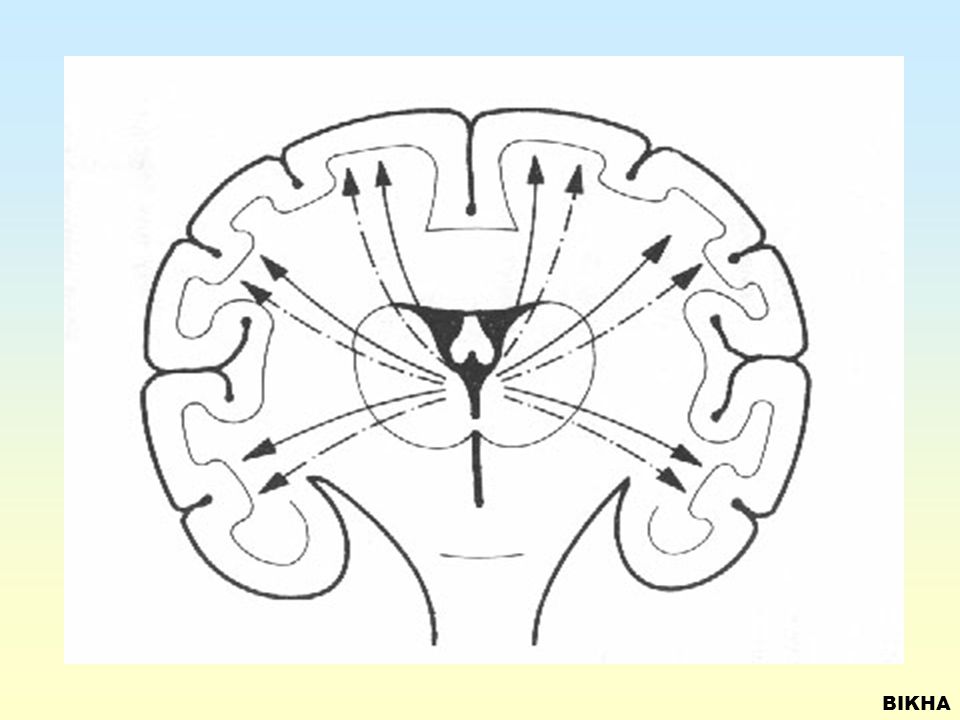
PRIMARY GENERALIZED SEIZURES Childhood non-convulsion

23
BIKHA

24
PRIMARY GENERALIZED SEIZURES Simple Absence Childhood non convulsive

25
BIKHA

26
PRIMARY GENERALIZED SEIZURES Childhood non convulsive (with facial clonus)
")
27
BIKHA

28
PRIMARY GENERALIZED SEIZURES Adolescent Myoclonic (upper limb)
")
29
BIKHA

30
PRIMARY GENERALIZED SEIZURES Adolescent myoclonic

31
BIKHA

32
PRIMARY GENERALIZED SIEZURES Adolescent clonic-tonic-clonic

33
BIKHA

34
PRIMARY GENERALIZED SEIZURES Childhood atonic

35
BIKHA

36
SECONDARY GENERALIZED SEIZURES Focus left occipital

37
BIKHA

38
SECONDARY GENERALIZED SEIZURES Frontal Lobe

39
BIKHA

40
SECONDARY GENERALIZED SEIZURES Focus central

41
BIKHA

42
NON-EPILEPTIC ATTACKS Breath holding Spells

43
BIKHA

44
NON-EPILEPTIC ATTACKS Psychogenic Seizures

45
BIKHA

46
NON-EPILEPTIC ATTACKS Psychogenic Seizures

47
BIKHA

48
Management of Epilepsy

49
BIKHA DIAGNOSIS OF EPILEPSY SEIZURE HISTORY Circumstances/Precipitant Timing/Duration Symptoms: preceding, during, after Frequency MEDICAL HISTORY PATIENT WITNESS

50
BIKHA

51
DD OF EPILEPSY SYNCOPE: Vasovagal, Cardiac, Cough, Micturation, etc. HYSTERIA, Swoon, Malingering, Simulation, Expressions of Immature Emotions OTHER PSYCHIATRIC ILLNESSES ACUTE VERTIGO MIGRAINE

52
BIKHA PSYCHIATRIC DIFFERENTIAL DIAGNOSES Conversion disorder Panic disorder Dissociative disorders Psychotic disorders Post-traumatic stress disorder Impulse control disorders Malingering etc.

53
BIKHA MEDICAL MANAGEMENT ? OBSERVATION ONLY…. No “Trial” treatment INFREQUENT FITS…. No treatment FREQUENT FITS…. Drug treatment. REGULAR REVIEW, Compliance, Drug S/E ADDITIONAL PROBLEMS Medical, Psychiatric, etc.

54
BIKHA PRINCIPLES OF DRUG TREATMENT Monotherapy better than polytherapy Slow introduction (1/4th dose) Increase weekly, titrate to optimal dose. Compliance Choice of drug depends on seizure type, side effects availability, cost

55
BIKHA CHOICE OF DRUGS (AEDs) GENERALISED TONIC-CLONIC, PARTIAL, OTHERS (95%) Carbamazepine (Tegral, Seizunil, Teril) Phenytoin ( Dihyden, Epilantin) Phenobarbitone Valproate (Epilim, Epival, Depakan) GENERALISED ABSENCE (5%) Ethosuximide (NA) Valproate (Epilim, Epival, Depakan)
 GENERALISED TONIC-CLONIC, PARTIAL, OTHERS (95%) Carbamazepine (Tegral, Seizunil, Teril) Phenytoin ( Dihyden, Epilantin) Phenobarbitone Valproate (Epilim, Epival, Depakan) GENERALISED ABSENCE (5%) Ethosuximide (NA) Valproate (Epilim, Epival, Depakan)")
56
BIKHA CHOICE OF DRUGS (AEDs) NEWER DRUGS Topiramate (Topamax) Lamotrigine (Lamictal) Gabapentin (Neurontin) Vigabatrin, Tiagabin, Levetiracetam SECOND LINE DRUGS Benzodiazepines (Clonazepam, Nitrazepam, Clobazam) Acetazolamide (Diamox, AZM)
 NEWER DRUGS Topiramate (Topamax) Lamotrigine (Lamictal) Gabapentin (Neurontin) Vigabatrin, Tiagabin, Levetiracetam SECOND LINE DRUGS Benzodiazepines (Clonazepam, Nitrazepam, Clobazam) Acetazolamide (Diamox, AZM)")
57
BIKHA NON-PHAMACOLOGICAL AND NON- VALIDATED TREATMENTS VAGAL STIMULATION- Helpful in upto 30% reduction in seizures KETOGENIC DIET (Medium Chain Glyderides) HERBAL HOMEOPATHIC YOGA MUSIC MEDITATION
 HERBAL HOMEOPATHIC YOGA MUSIC MEDITATION")
58
BIKHA STATUS EPILEPTICUS Def: Convulsions lasting > 5-10 min (single or serial). Potentially fatal…. Must hospitalize. Commonest cause…. low compliance. All steps of “Coma Management”. Asses cause…. investigate while controlling fits. IV 50 ml 25% glucose, B1 (1 ampule neurobion). Diazepam 10 mg IV…. Repeat every 30 min if recur. Or 200 mg in 500 ml drip at rate 20 drops/min. Phenytoin 18mg/kg; rate not more than 50mg/min Valproate IV …. 500-750mg 6-8 hourly.
. Diazepam 10 mg IV…. Repeat every 30 min if recur. Or 200 mg in 500 ml drip at rate 20 drops/min. Phenytoin 18mg/kg; rate not more than 50mg/min Valproate IV … mg 6-8 hourly..")
59
BIKHA SIMPLE FEBRILE CONVULSION (SFC) 5% of all normal Children Age-Specific…. 6m-5y. Generalized convulsion Duration of fit…. <5 min. No neurological deficit No F/H/O of epilepsy Total number of fits <6 in the age 6m-5y. If all above + …. good prognosis.

60
BIKHA COMPLEX FEBRILE CONVULSION (CFC) Patient who do not fulfill SFC criteria Multiple fits in the same febrile episode Focal seizures High risk children…. focal n. sign or handicap Single generalized seizure > 5 min. Suspected with CNS infection…Meningitis, Encephalitis

61
BIKHA COUNSELLING IS CRUCIAL Explain nature of disorder; “electric model” Reinforce compliance Discuss expectations, limitations and S/E of AEDs Driving, employment, Leisure activities Education Marriage, children, hereditary

62
BIKHA

Similar presentations