Download presentation
Presentation is loading. Please wait.

1
A Rehospitalization Reduction Program on a Geriatric Skilled Nursing Unit Randi Berkowitz, MD Hebrew SeniorLife

2
Why decrease readmissions? I.Excellence in care –Decrease errors – patient satisfaction – staff satisfaction II.Financial –Increased referrals – subacute beds long-term care – census – reimbursement/patient

3
How? 1.Admission 2.Stay on unit 3.Discharge

4
Reducing AVOIDABLE hospital transfers

5
Bucket #1: Problems on Admission Ineffective communication of prognosis / options PCP out of loop Inadequate care plans for recurrent symptoms

6
Reduce AVOIDABLE hospital transfers Approach to the Problem: Admission MD standardized discussions Communication family and PCP High risk patients –Automatic Palliative Care consult –Flag for entire team

7
Bucket #2: Stay on Unit: Problems With Team Operation Disciplines operating in silos Failure to identify problems early Failure to learn from mistakes

8
Reduce AVOIDABLE hospital transfers Approach to the Problem: Stay on the Unit Team Improvement for the Patient and Safety (TIPS) conference Call to hospital Root cause analysis
 conference Call to hospital Root cause analysis")
9
Bucket #3: Problems With Home Discharge Poor hand off to next team No teach back with patient/HCP No standardized discharge summary/ nursing process

10
Reduce AVOIDABLE hospital transfers Approach to the Problem: Home Discharge Project RED –Written home care plan from electronic medical record –Making specific for geriatric use E.g. advance directives, diet, VNA, assistive devices Standardized discharge summaries

11
Target Population All admissions to the RSU subacute unit 1000 admissions a year 3NP/3MD- geriatric and palliative care certified

12
Process and Outcome Measures Admission –90% patients have discussion with MD prognosis rehospitalizations past 6 months Communication family and PCP –Patient/ family satisfaction survey

13
Process and Outcome Measures Middle- Stay on the unit –Unplanned discharge rates –benchmarked staff safety survey for staff

14
Process and Outcome Measures Discharge Home 30 day readmission rates after discharge from SNF Satisfaction survey of discharge preparedness

15
Perceived Facilitators/Barriers Pt acceptance of less aggressive approaches Increased liability Increase cost keeping sicker patients Difficulty obtaining information from hospital Time needed to engage primary care Lack of practitioner access to computer systems in key referral sites Limited IT resources for Project RED

17
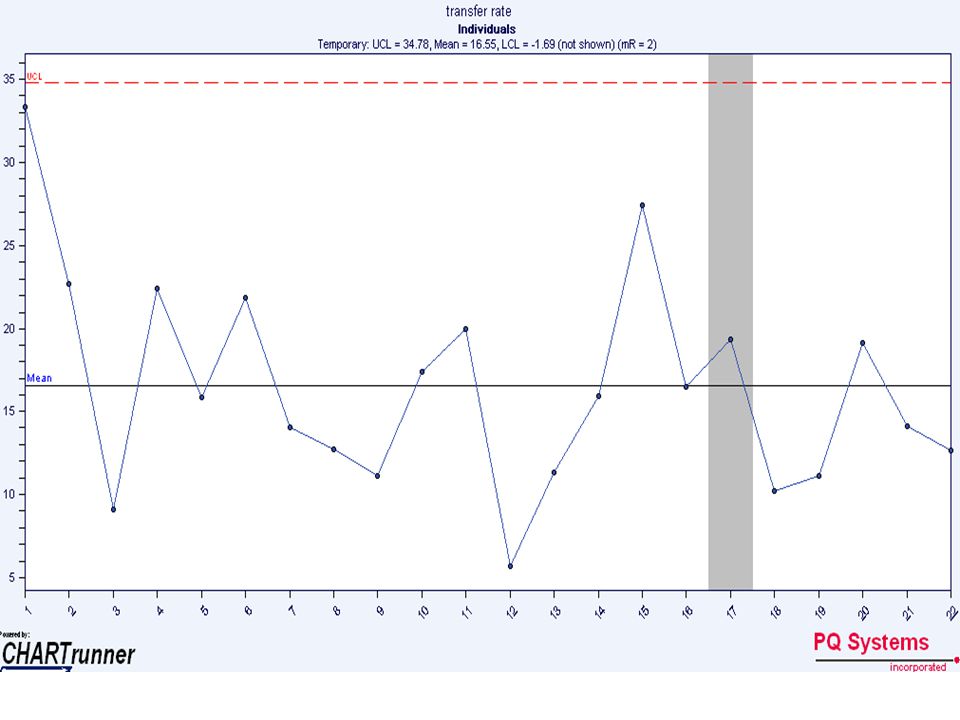
Preliminary Data Unplanned Transfers January 2008- June 2009 compared with post TIPS July 2009-November 2009 Massachusetts 30 day 22-28% Pre-intervention16.9% Post-intervention12.7% Rate Reduction-24.7%

18
Staff feel safe reporting their mistakes

19
Questions Flag risk to entire team Avoidable-unavoidable discharges RED call everyone 30 days- use OASIS Call those LTC Aides to TIPS conferences Survey admission process high risk vs everyone tool

Similar presentations







 A Community Collaboration.>")











