Download presentation
Presentation is loading. Please wait.

1
SLIDESHOW PRACTICE

2
What is this? What condition it associated with?
What are the most common causes of this condition? What oesophageal condition is it associated with? Name 3 important investigations

3
ANSWERS Iron deficiency anaemia
Caused by blood loss (gi bleed, menorrhagia; hookworm in tropics, malabsorption (coeliac disease) Plummer Vinson syndrom (post cricoid web) FBC, ↓serum iron, ↓ferritin, ↑TIBC, FOB, sigmoidoscopy, colonoscopy, barium enema Tx – oral iron
 Plummer Vinson syndrom (post cricoid web) FBC, ↓serum iron, ↓ferritin, ↑TIBC, FOB, sigmoidoscopy, colonoscopy, barium enema. Tx – oral iron.")
4
Describe immediate management
A 52 year old diabetic man presented to A and E feeling sick. 1 week previously his GP had treated him for reflux Describe immediate management

5
ANSWER Morphine Oxygen Nitrates (buccal suscard) Aspirin 300mg
B-blocker and ACE-I (within 24 hours) Thrombolysis if no contraindications! As presented within 24 hours of ischaemic chest pain with ST elevation of at least 2mm in 2 adjacent chest leads PRIMARY PCI IF IN COOL TEACHING HOSPITAL
 Thrombolysis if no contraindications! As presented within 24 hours of ischaemic chest pain with ST elevation of at least 2mm in 2 adjacent chest leads. PRIMARY PCI IF IN COOL TEACHING HOSPITAL.")
6
CONTRAINDICATIONS TO THROMBOLYSIS
Internal bleeding Prolonged/traumatic CPR Any prev haemorrhagic stroke Ischaemic stroke within 1 year Recent trauma surgery (2 weeks) Intracerebral neoplasm/recent head trauma Suspected aortic dissection Prev allergic reaction to fibrinolytic
 Intracerebral neoplasm/recent head trauma. Suspected aortic dissection. Prev allergic reaction to fibrinolytic.")
7
Report this Xray Describe 5 changes you should look for on the XRay in this condition What investigations would you do if this was an acute problem? How would you manage?

8
5 changes in L ventricular failure
A alveolar oedema (bat wings) B Kerley B lines (interstitial oedema) C Cardiomegaly D Dilated upper lobe vesseld E Pleural Effusion SIGNS: tachycardia, basal creps, pink frothy sputum, PND, orthopnoea FBC, U+E, cardiac enzymes, ECG (ischaemia, MI, LVH), ABG, BNP (raised in failure) Echo
 B Kerley B lines (interstitial oedema) C Cardiomegaly. D Dilated upper lobe vesseld. E Pleural Effusion. SIGNS: tachycardia, basal creps, pink frothy sputum, PND, orthopnoea. FBC, U+E, cardiac enzymes, ECG (ischaemia, MI, LVH), ABG, BNP (raised in failure) Echo.")
9
Commonest causes of acute LVF?
Post MI myocardial ischaemia Malignant hypertension aortic stenosis or aortic incompetence mitral incompetence arrythmia

10
Management of acute LV failure
Sit up Give 100% 02 IV access monitor ECG for arrythmias, MI etc Diamorphine mg IV slowly Metoclopramide 10mg iv Frusemide 40-80mg IV slowly Give sublingual GTN if systolic BP>100 Monitor urine output (catherterise) Repeat ABG and K+ if condition deteriorates
 Repeat ABG and K+ if condition deteriorates.")
11
A 58-year-old afebrile woman presented with a 2-day history of pain and red streaks of her right leg following minor trauma. There were palpable cords beneath the erythematous streaks. How would you manage?

12
ANSWER SUPERFICIAL THROMBOPHLEBITIS
Treatment includes gentle support by means of a bandage or stocking and elevation of the affected leg. Anti-inflammatory drugs such as ibuprofen 400mg tds. duplex ultrasound scan (DVT risk)
")
13
This 55year old man has returned from a holiday 2 weeks ago with arthralgia, malaise, lymphadenopathy and peripheral neuropathy He has the following lesion which started as a red macule. What is the diagnosis? How would you treat?

14
Erythema chronicum migrans
classical immune-mediated skin lesion which occurs at the site of the bite in Lyme disease some weeks after the bite by the tick. (boriella burgdorferi infection) The tick bite leaves a red macule or papule which approximately later expands to produce a hot, painless annular/target lesion. Tx doxycycline
 The tick bite leaves a red macule or papule which approximately later expands to produce a hot, painless annular/target lesion. Tx doxycycline.")
15
Lyme disease often the first manifestation of Lyme disease = Lyme borreliosis spirochete Borrelia burgdorferi is transmitted by the bite of the deer tick Ixodes scapularis in the northeastern U.S. systemic borreliosis is a potentially serious disease, causing both acute and chronic symptoms such as fever, malaise, arthralgia, carditis, arthritis, meningitis, neuropathy, ataxia

16
TROUSSEAU’s SIGN This is a recurring thrombophlebitis characterised by successive crops of tender nodules in affected blood vessels. Different veins may be affected simultaneously or randomly. It denotes a thrombotic state and is associated with visceral malignancy, especially of the pancreas and lung. Thrombophlebitis migrans was first recognised by Trousseau in the diagnosis of his own pancreatic cancer.

17
What is this? What causes it? What other signs would you look for?

18
ANSWER Plummer vinson syndrome (Post cricoid web) Iron deficiency anaemia Koilonychia, pallor, atrophic mucous membranes, tachycardia if marked Tx balloon dilatation and iron supplements Pre-malignant!!!

19
This patient presented with weight loss and this crazy skin condition…
What is it? Clue: say what you see

20
Erythema Gyratum Repens
wood-grain" pattern (repens is a plant) wavy, erythematous, urticarial bands with scale slowly migrate breast, stomach, bladder, prostate, cervix; (occasionally no CA )
 wavy, erythematous, urticarial bands with scale. slowly migrate. breast, stomach, bladder, prostate, cervix; (occasionally no CA )")
21
This patient presented with weight loss, a palpable liver.
What is this skin condition and with what condition is it associated?

22
Necrolytic migratory erythema
Glucagonoma - alpha cell tumor of the pancreas is associated with this condition (in more than 70% of patients) abdomen, thighs and buttocks present with attacks of hyperglycaemia (diabetes mellitus occurs in more than 50% of cases), anaemia, rash and diarrhoea. Also glossitis, angular cheilitis, normocytic anemia 90% have liver metastasis at presentation
 abdomen, thighs and buttocks. present with attacks of hyperglycaemia (diabetes mellitus occurs in more than 50% of cases), anaemia, rash and diarrhoea. Also glossitis, angular cheilitis, normocytic anemia. 90% have liver metastasis at presentation.")
23
This 22yr old woman presents with weight loss and bloody diarrhoea
She develops this lesion on her ankle What is it? What else is her condition associated with?

24
Pyoderma gangrenosum characteristic rapidly expanding ulcer with bluish undermined border; often lower extremities; begin as sterile pustules 1% to 10% of patients with active ulcerative colitis; often (but not always) parallels disease Other disease associations: Crohn’s, chronic active hepatitis, rheumatoid arthritis, HIV infection; acute and chronic granulocytic leukemia (bullous PG) UC associated with uveitis, arthropathy, erythema nodosum, sclerosing cholangitis
 parallels disease. Other disease associations: Crohn’s, chronic active hepatitis, rheumatoid arthritis, HIV infection; acute and chronic granulocytic leukemia (bullous PG) UC associated with uveitis, arthropathy, erythema nodosum, sclerosing cholangitis.")
25
What is this sign? Name 4 causes of this condition

26
Grey turners Acute pancreatitis Gallstones Ethanol Trauma Steroids
Mumps Autoimmune (PAN) Scorpion Hyperlipidaemia ERCP Drugs (azathiporine, mercaptourine, diuretics?
 Scorpion. Hyperlipidaemia. ERCP. Drugs (azathiporine, mercaptourine, diuretics")
27
What is this?

28
Cullen’s sign yellow blue discolouration of the skin around the umbilicus. It was first reported in ruptured ectopic pregnancy but is more commonly associated with severe, acute pancreatitis. It is caused by pancreatic enzymes that have tracked along the falciform ligament and digested subcutaneous tissues around the umbilicus.

29
What is this. What else would you look for
What is this? What else would you look for? What investigations would you do? What treatment would you start?

30
Tendon xanthoma extensor tendons of fingers, patella, elbows, Achilles tendon (one of the most common sites); diffuse infiltration of tendon by lipid Xanthelasma in eyes, corneal arcus hypercholesterolemia; Types II and III Lipid profile Statins

31
What is this? What is it associated with?

32
Acanthosis nigricans velvety thickening and darkening (hyperpigmentation) of the skin, especially on the nape of the neck, axillae and other body folds underlying causes obesity; drugs; "malignant" acanthosis nigricans; hereditary, benign AN GLUCOSE INTOLERANCE, INSULIN RESISTANCE
 of the skin, especially on the nape of the neck, axillae and other body folds. underlying causes. obesity; drugs; malignant acanthosis nigricans; hereditary, benign AN. GLUCOSE INTOLERANCE, INSULIN RESISTANCE.")
33
Another example

34
What is this? With what conditions is it associated?

35
Erythema nodosum deep erythematous painful nodules, symmetrically on the lower legs; female predominance; a hypersensitivity panniculitis fever, chills, malaise, leukocytosis disease associations: streptococcal infections, drugs (OCPs, sulfonamides, iodides), pregnancy, TB, deep mycoses, acute sarcoidosis, inflammatory bowel disease
, pregnancy, TB, deep mycoses, acute sarcoidosis, inflammatory bowel disease.")
36
What is this and with what condition is it associated?

37
Keratoderma blenorrhagica
Keratoderma blenorrhagia is a skin condition associated with Reiter's syndrome. urethritis conjunctivitis a seronegative arthritis In this disorder there are vesicles which fill in with caseous material. Pustular psoriasis may produce an identical clinical and histological picture. The lesions are found: soles of the hands and feet penis, causing a circinate balanitis in the mouth It is treated with 1% hydrocortisone.

38
What are these lesions? With what are they associated?

39
Erythema multiforme form of cutaneous reaction to an underlying condition. In 50% of cases, a cause can’t be identified common causes: HERPES VIRUS drugs (sulfonamides, phenytoin, barbiturates, penicillin, etc.); infections (esp. herpes simplex and Mycoplasma) inflammatory bowel disease eruption usually lasts for a week or two, then spontaneously remits the "target" lesion is approximately 1cm dull-red macule or papule with a central area of blistering or hemorrhage
; infections (esp. herpes simplex and Mycoplasma) inflammatory bowel disease. eruption usually lasts for a week or two, then spontaneously remits. the target lesion is approximately 1cm dull-red macule or papule with a central area of blistering or hemorrhage.")
40
What is this? What are the common causes?

41
urticaria IDIOPATHIC IS MOST COMMON
Drugs (e.g., penicillins, aspirin, NSAIDs, opiates, phenytoin, atropine, metronidazole phenytoin Food stuffs, insect bites, candida infections systemic lupus erythematous - in early stages, urticaria may be the only clinical abnormality, with wheals persisting for an unusually long time days viral hepatitis - may begin with urticaria Still's disease rheumatic fever hyperthyroidism Primary lesion is a wheal, a flesh-colored to pink, well circumscribed plaque caused by dermal edema; itchy! Individual lesions last only a few hours, never more than 24 hours MAJORITY NO CAUSE IS FOUND THEREFORE DO NOT INVESTIGATE!!!

42
A 32 year old man presents with unilateral leg swelling
A 32 year old man presents with unilateral leg swelling. What is your differential diagnosis? How would you investigate and manage this problem?

43
Diff diagnosis of unilateral leg swelling
Deep vein thrombosis Cellulitis Ruptured Baker’s cyst Lymphoedema Fracture

44
DVT Figure 2: Well’s Clinical model for predicting pretest probability. Clinical feature Score Active cancer Paralysis, paresis or recent plaster immobilisation of lower extremities 1 Recently bedridden > 3days or previous surgery within 12 weeks requiring regional or general anaesthesia Localised tenderness along the distribution of deep venous system 1 Swelling of the entire leg Calf swelling by more than 3cm compared with asymptomatic leg 1 Pitting oedema confined to the symptomatic leg 1 Collateral superficial veins Previously documented DVT Alternate diagnosis as likely or greater than that of DVT -2

45
Well’s criteria SCORE >3 HIGH RISK SCORE 1-2 MODERATE RISK
SCORE <1 LOW RISK D-dimer for LOW RISK- good negative predictive value USS of deep veins (duplex ideally) Tx clexane (until INR between 2 and 3) Warfarin, support hosiery
 Tx clexane (until INR between 2 and 3) Warfarin, support hosiery.")
47
Steven johnsons syndrome
severe and sometimes fatal form of erythema multiforme. Bullous ulcerating lesions higher incidence in children and young adults, and it is twice as common in males than females. seen more often as a response to drugs such as sulphonamide, some sedatives and penicillin or infection or neoplasia

48
Differential diagnosis of SJ
Behcet's syndrome Reiter's syndrome syphilis - primary or secondary hand, foot and mouth disease pemphigus toxic epidermal necrolysis Kawsasaki disease Tx refer to specialist care (dermatologist) supportive tx
 supportive tx.")
49
USS of legs. Describe what this shows
Which is normal? A or B? Management?

50
Compression US of legs B is normal – normal compressibility
A shows non compressibility – i.e thrombosis in vein Tx clexane until warfarin in therapeutic range. Continue warfarin 3-6 months IVC filter if worried about PE TED stockings

51
Jimmy has just enjoyed a snickers bar… he now looks like this…
What is happening to poor jimmy? Describe your immediate management

52
ANAPHYLAXIS AIRWAY 100% 02 IV adrenaline 1:1000 solution
0.5mL (500mcg) IM Repeat in 5 minutes if no clinical improvement IV access and fluids (colloid if hypotensive) Antihistamine H1-antagonist (chlorphenamine) mg IM/slow IV Hydrocortisone mg IM/slow IV (if severe/recurrent/in asthmatics) If bronchospasm does not subside treat as asthma – salbutamol nebs (adjunctive measure)
 IM. Repeat in 5 minutes if no clinical improvement. IV access and fluids (colloid if hypotensive) Antihistamine H1-antagonist (chlorphenamine) mg IM/slow IV. Hydrocortisone mg IM/slow IV (if severe/recurrent/in asthmatics) If bronchospasm does not subside treat as asthma – salbutamol nebs (adjunctive measure)")
53
Young female presents with weight loss, polyuria and these leg lesions…what is this and what condition is it associated with?

54
Necrobiosis lipoidica
This is a dermatological condition that is associated with diabetes mellitus in 50% of cases. It occurs in women three times more frequently than in men, usually in young adults or in early adult life. Necrobiosis lipoidica usually affects the skin on the lateral and anterior surfaces of the lower legs The epidermis is smooth or slightly scaly and atrophic. Delicate vessels may be observed through the surface. Long standing lesions may show ulceration, fibrosis and scarring. if non-ulcerated necrobiosis lipoidica - topical corticosteroids if ulcerated NL then there may be response to immunomodulating drugs such as cyclosporin and mycophenolate mofetil

55
What is this? With what is it associated?

56
Granuloma annulare Granuloma annulare is a condition which presents with skin lesions that consist of asymptomatic dermal nodules. In children, they are usually on the fingers or toes. This condition is harmless but resolution may take many months. In the adult, this condition is sometimes associated with diabetes.

57
What is being tested here
What is being tested here? What else would you look for in your examination? How would you investigate and treat?

58
Dehydration reduced tissue turgor thirst dry mucous membranes
sunken eyes Prolonged capillary refil tachycardia dark urine hypotension (late sign in young- preterminal) low urine output (<600 ml/day or 30 ml/hr)
 low urine output (<600 ml/day or 30 ml/hr)")
59
Investigating and treating dehydration
fluid loss without water replacement - for example, an unconscious patient with fluid lost from diarrhoea, burns, vomiting, sweat, respiration diabetes insipidus osmotic diuresis - for DKA Conn's syndrome - hypokalaemic alkalosis Cushing's syndrome incorrect intravenous fluid replacement some patients with hyperosmolar non-ketoacidotic diabetic coma; this condition may also cause hyponatraemia hypothalamic dysfunction

60
Management of severe hypovolaemia
Lie patient flat and raise feet to restore BP IV access - Two large cannulae - brown venflons Give colloid/crytalloid (no evidence either is better) Insert CVP line/arterial line (more accurate assessment of BP) Catheterise and monitor urine output. Monitor Bp, lying and standing, JVP, chest… Pulmonary OEDEMA Take blood for group and save, crossmatch. fluid should be run in as fast as possible; patient's response monitored. If the patient remains shocked, group specific or O Negative blood should be given as cross-matching may take up to 45 minutes. If the patient still fails to improve, internal bleeding should be sought. Following stabilisation, fluid infusion may be moderated according to urine production. Give blood to maintain Hb>8g/dl
 Insert CVP line/arterial line (more accurate assessment of BP) Catheterise and monitor urine output. Monitor Bp, lying and standing, JVP, chest… Pulmonary OEDEMA. Take blood for group and save, crossmatch. fluid should be run in as fast as possible; patient s response monitored. If the patient remains shocked, group specific or O Negative blood should be given as cross-matching may take up to 45 minutes. If the patient still fails to improve, internal bleeding should be sought. Following stabilisation, fluid infusion may be moderated according to urine production. Give blood to maintain Hb>8g/dl.")
61
Hypovolaemia Haemorrhage – aortic dissection, leaking AAA, splenic rupture Fluid loss - Diarrhoea, vomiting, polyuria,burns 3rd space losses- acute pancreatitis, ascites Adrenal failure

62
What is this x ray showing?
what condition is this person likely to have? What are the complications of this condition?

63
arachnodactyly MARFAN’S SYNDROME (AD) – diff diagnosis homocystinuria -disorder of methionine metabolism OCULAR upward lens dislocation retinal detachment SKELETAL and MUSCLES arachnodactyly tall with disproportionately long legs and arms - the span of the arms is greater than the height pectus excavatum spinal abnormalities - spondylolisthesis, scoliosis SUFE generalised joint laxity with predisposition to flat feet or dislocation of patella or shoulder CARDIOVASCULAR dilatation of the aorta may aortic regurg, mitral regurg dissecting aneurysm of the aorta Mental development is normal. The average lifespan of an affected individual is 40 to 50 years.

64
What is this and with what conditions is it associated?

65
Dupuytrens contracture
Liver disease Epilepsy/ treatment with phenobarbitone or phenytoin Peyronie's disease - penile fibrosis Family history trauma myxoedema diabetes mellitus hypercholesterolaemia AIDS

66
What is this called? What conditions is it associated with??

67
Alopecia areata localised, round bald patches developing suddenly over one or two weeks, without any preceding symptoms. At the edge of the patch, there may be small, broken hairs with a tapering shaft - 'exclamation mark' hairs. autoimmune phenomenon Asssociations: thyroid disorders, vitiligo, diabetes.

68
A diabetic patient developed this eruption…what is it?
These are small rounded plaques with raised borders lying in a linear fashion over the shins. In late diabetic dermopathy these may present as pigmented scars.

69
Diabetic dermopathy These are small rounded plaques with raised borders lying in a linear fashion over the shins. In late diabetic dermopathy these may present as pigmented scars.

70
What is wrong with these chaps?

71
Peyronie’s disease the penis becomes curved due to asymmetrical fibrosis in the fascia surrounding the corpora cavernosa. Curvature towards the affected side is increased during an erection making intercourse difficult and painful Assoc with dupuytrens contracture and premature atherosclerosis

72
What is wrong with this chap?

73
Winged scapula Long thoracic nerve injury
The long thoracic nerve supplies the serratus anterior muscle. It may be injured as a result of pressure on the shoulder, either from a sudden blow or by prolonged carrying of heavy objects. It is often one of the nerves affected in brachial neuritis and may also be damaged in diabetes mellitus. Winging of the scapula results.

75
Henoch schonlein Henoch-Schonlein purpura is a condition characterized by a widespread necrotizing vasculitis of arterioles and small capillaries. children aged 3 to 8 years are affected, boys more than girls, Abdo pain, arthritis (large joints) and glomerulonephritis 70% have haematuria and proteinuria, but the glomerulonephritis is often asymptomatic, conferring a good prognosis. The disease is usually self limiting. Bed rest and simple analgesics may be prescribed for arthropathy
 and glomerulonephritis. 70% have haematuria and proteinuria, but the glomerulonephritis is often asymptomatic, conferring a good prognosis. The disease is usually self limiting. Bed rest and simple analgesics may be prescribed for arthropathy.")
76
What is this? What aggravates this condition? How do you treat?

77
psoriasis Made worse by stress, alcohol, b-blockers, infection
Better in sunlight Tx emolients, dithranol, Vitamin D analogues, coal tar, keratolytics PUVA Methotrexate, cyclosporin Infliximab, Etanercept

79
erythrodermic psoriasis
Life threatening complication of psoriasis Plaques cover over 90% of the body surface. Problems with thermoregulation, septicaemia, dehydration and high output cardiac failure may occur.

80
This middle aged man is very unwell and has lost weight
He developed these slowly evolving itchy lesions What is the diagnosis?

81
Mycosis fungoides Mycosis fungoides is a non-Hodgkin's lymphoma that arises from CD4+ T lymphocytes. It is a cutaneous lymphoma that characteristically affects middle aged males. It usually begins as an eczematous reaction and proceeds to form plaques, tumours and fungating ulcers. Erythroderma may occur which often is highly pruritic. Treatment - topical steroids, topical cytotoxic agents, PUVA or radiotherapy. Prognosis relates to extent and type of skin involvement - average survival in the early stage of this disease is at least years (2)
")
82
What has this young chap developed?

83
Eczema herpeticum widespread HSV infection superimposed on pre-existing (often mild) atopic eczema. Widespread vesicles and erosions, fever, and malaise occur. treat with intravenous and topical acyclyovir broad spectrum antibiotics are added in to treat or prevent superinfection. It is necessary to scrupulously care for the skin and carefully monitor fluid and electrolyte balance. Prophylactic oral aciclovir is indicated for recurrent disease.

84
Eczema herpeticum again

85
What has this 72 year old man developed? What would you advise?

86
Chronic venous insufficiency
Wear thick socks Avoid bruising Raise legs up as often as possible Compression bandaging for ulcer Tx dermatitis, infection

87
What is this? What are the main complications?

88
Neurofibromatosis (2 types)
von Recklinhausen's disease, peripheral or type I neurofibromatosis (AD) bilateral acoustic neurofibromatosis, central or type II neurofibromatosis Café au lait spots commonly seen COMPLICATIONS: Nerve entrapment Peripheral nerve tumours neuropathy
 bilateral acoustic neurofibromatosis, central or type II neurofibromatosis. Café au lait spots commonly seen. COMPLICATIONS: Nerve entrapment. Peripheral nerve tumours. neuropathy.")
89
What is this?

90
pemphigoid autoimmune blistering disorder
characterized by large, tense, intradermal (subepidermal) blisters on an erythematous base. BLISTERS REMAIN INTACT. If in eyes- blindness Elderly affected, Women > men. it is more common than pemphigus treatments that aim to suppress the inflammatory process, e.g. corticosteroids, antibiotics (e.g. tetracyclines, sulphones) other immunosuppressive treatments aim to suppress the production of the pathogenic antibodies, e.g. high-dose corticosteroids e.g. prednisolone mg per day, azathioprine, methotrexate, cyclophosphamide and cyclosporin
 blisters on an erythematous base. BLISTERS REMAIN INTACT. If in eyes- blindness. Elderly affected, Women > men. it is more common than pemphigus. treatments that aim to suppress the inflammatory process, e.g. corticosteroids, antibiotics (e.g. tetracyclines, sulphones) other immunosuppressive treatments aim to suppress the production of the pathogenic antibodies, e.g. high-dose corticosteroids e.g. prednisolone mg per day, azathioprine, methotrexate, cyclophosphamide and cyclosporin.")
91
What is this?

92
PEMPHIGUS blisters within the epidermis of both skin and mucous membranes. autoimmune basis? Peak onset is between 60 and 70 years of age. W>M In comparison, bullous pemphigoid is characterised by blister formation at the level of the basement membrane and not within the epidermis.

93
Long standing asymptomatic lump. What is the likely diagnosis?

94
Lipoma Treatment is for cosmesis and consists of local excision.
Some individuals have multiple subcutaneous lipomata; a biopsy may be required to exclude neurofibromatosis in such patients. The patient with multiple, tender lipomata may have Dercum's disease. A rare complication of lipomata is a liposarcoma.

95
What is shown at the arrow?

96
Ascending lymphangitis
spreading of infection from its focus along regional lymphatic vessels. Commonly, an abscess forms at the regional nodes. commonly due to Streptococcus pyogenes; less often, to Staphylococci. It presents as red blushes and streaks in the skin corresponding to the inflamed lymphatics. Treatment is bed rest with the affected limb elevated. Penicillin V and Flucloxacillin Permanent lymphatic obstruction may develop resulting in a persistent oedema. Repeated attacks cause chronic lymphangitis.

97
What is this? It started life as a red macule.

98
Erythema chronicum migrans
Caused by Borrelia burgdorferi, Lyme disease is common in the northeast United States and in Wisconsin and Minnesota. It is carried by Ixodes spp. of ticks. The rash occurs in 2/3 of those infected, with a solitary lesion characteristic of Stage 1 disease, and multiple lesions characteristic of disseminated Stage 2 disease

99
What is this associated with?

100
Vitiligo is associated with
Hypothyroidism Addison’s disease diabetes mellitus pernicious anaemia Tx camouflage cream

101
What does this 72 year old chap have?

102
Basal cell carcinoma This is a locally invasive carcinoma of the basal layer of the epidermis. It almost never metastasizes but it may kill by local invasion. sunlight exposure the initial lesion is a small pearly-white nodule with visible (telangiectatic) blood vessels; early lesions may bleed and ulcerate and then heal again a red nodule forms which expands to leave a characteristic rolled edge with central ulceration ('rodent ulcer') Tx: surgery, local radiotherapy, cryotherapy, or curretage
 blood vessels; early lesions may bleed and ulcerate and then heal again. a red nodule forms which expands to leave a characteristic rolled edge with central ulceration ( rodent ulcer ) Tx: surgery, local radiotherapy, cryotherapy, or curretage.")
103
Think maybe he should have come to the doc sooner about this one

104
What is this?

105
Squamous cell carcinoma
Squamous cell carcinoma (SCC) is a malignant tumour of the epidermis in which the cells, if differentiated, show keratin formation. basal cell carcinoma keratocanthoma malignant melanoma solar keratosis pyogenic granuloma infected seborrheic wart rapidly expanding painless, ulcerated nodule rolled indurated margin. Often the lesion may have a cauliflower-like appearance with areas of bleeding, ulceration or serous exudation. Metastatic potential – surgery (+radio/chemo if advanced)
 is a malignant tumour of the epidermis in which the cells, if differentiated, show keratin formation. basal cell carcinoma. keratocanthoma. malignant melanoma. solar keratosis. pyogenic granuloma. infected seborrheic wart. rapidly expanding painless, ulcerated nodule rolled indurated margin. Often the lesion may have a cauliflower-like appearance with areas of bleeding, ulceration or serous exudation. Metastatic potential – surgery (+radio/chemo if advanced)")
106
What is this? What types exist and what features are characteristic in this lesion?

107
Malignant melanoma superficial spreading (48%) nodular (23%)
lentigo maligna (15%) acral lentiginous including periungual (6%) amelanotic melanoma Change in SHAPE, SIZE, COLOUR >5mm diameter, inflammation, bleeding, irritation Excision biopsy (1cm margin for every mm thickness)
 acral lentiginous including periungual (6%) amelanotic melanoma. Change in SHAPE, SIZE, COLOUR. >5mm diameter, inflammation, bleeding, irritation. Excision biopsy (1cm margin for every mm thickness)")
108
What is happening in this patients arm
What is happening in this patients arm? They previosly had a simple ulcer there

109
Marjolin’s ulcer (arm)
cancer

110
What is this condition?

111
Peutz Jeghers Peutz-Jegher's syndrome (AD)
multiple hamartogenous polyps of the gastrointestinal tract - most often in the small bowel but may occur affect any portion of the GI tract mucocutaneous pigmentation - mainly, of the lips, buccal mucosa, genitalia, hands and feet Patients often present with small bowel intussusception before the age of 10 years. The polyps themselves have a very low malignant potential. About 10-20% of patients develop gastrointestinal carcinoma but this is thought to arise from coexistent adenomas. Patients have an increased risk of developing carcinomas of the pancreas, lung, ovary and breast.

112
What are these lesions?

113
Lichen planus flat-topped shiny violaceous (pink/mauve/purple)
typically they are seen on the inner aspects of the elbows, on the wrists, shins and sacral area and genitals Wickhams striae mouth lesion This is a condition of unknown aetiology characterized by intensely pruritic flat topped papules that are usually seen on the inner aspect of the elbows and wrists. The mucous membranes are often affected.

114
What does this chap have? What complications is it associated with?

115
Ehlers danlos Ehlers-Danlos syndrome (EDS) is a condition where abnormalities of collagen production result in bruising, wide scars, laxity of joints and hyperelasticity of the skin. Hernia MR/AR Aortic dissection pneumothoraces GI bleeds
 is a condition where abnormalities of collagen production result in bruising, wide scars, laxity of joints and hyperelasticity of the skin. Hernia. MR/AR. Aortic dissection. pneumothoraces. GI bleeds.")
116
This 34 year old wool factory worker presented with this…what is it?

117
Cutaneous anthrax Anthrax sheep wool

118
What is this?

119
tylosis Tylosis is a congenital hyperkeratosis with pitting of the palms - tylosis palmaris - and of the soles - tylosis plantaris. It is inherited as an autosomal dominant trait. In some cases, it is associated with oesophageal carcinoma. Treatment measures include the use of a keratolytic. Systemic treatment with retinoids may be used

120
What is wrong with this chap? How would you diagnose it?

121
Kaposis sarcoma Kaposi's sarcoma is a multicentric, malignant neoplastic vascular proliferation, characterised by the development of bluish-red nodules on the skin. Sometimes there may be widespread visceral involvement. It may metastasize to lymph nodes. occurs in immunocompromised patients (e.g. HIV positive patients, transplant patients) Diagnosis: skin biopsy
 Diagnosis: skin biopsy.")
122
What is this?

123
keratoacanthoma Difficult to distinguish from SCC
rapidly growing epidermal tumour that resembles squamous cell carcinoma both clinically and histologically. It is believed to arise from hair follicles. There is little evidence that keratocanthoma has malignant potential Trauma, viral infection, sun exposure, and chronic exposure to tar, pitch and petroleum have all been implicated as aetiologic agents. Surgical excision is thought to produce less scarring than leaving the lesion to resolve spontaneously.

124
What are these? What are they associated with?

125
Gottrons papules Gottron's papules are scaly, erythematous lesions affecting the dorsum of the hands, knuckles, and extensor surfaces of other small joints. They are characteristic of dermatomyositis.

126
What does this patient have? With what is it associated?

127
Heliotrope rash Polymyositis and dermatomyositis are systemic connective tissue diseases which are characterised by acute and chronic inflammation of striated muscle. In dermatomyositis there is an accompanying dermatitis. The limb girdle or proximal muscles are most severely affected but their bulk is preserved beyond that expected from their weakness: this is an important sign distinguishing this condition from a limb girdle dystrophy. The aetiology is unknown but there is an association with HLA-B8 and HLA-DR3. Dermatomyositis in males over the age of 60 years may be suggestive of an underlying systemic malignancy.

128
This 33 year old woman presented with fever, tachycardia, chills, malaise and this hot tender lesion on her face. What is it? What is tx?

129
erysipelas Erysipelas is a rapidly spreading Streptococcal infection of the skin and subcutaneous tissue characterized by cellulitis and lymphangitis. Streptococcus pyogenes fever, tachycardia, chills, malaise the infected area is red, hot, and tender e.g. red shiny plaque on face local oedema which produces a raised border that is clinically diagnostic the cellulitis spreads rapidly to involve uninfected skin careful examination may reveal an abrasion through which the streptococcus organism gained entry an incision within the infected area exudes a thin pus Tx: amoxicillin

130
What is wrong with this chap? What could have caused it?

131
Left CN III palsy TUMOUR, INFECTION, VASCULITIS, DEMYELINATION SAFE ANSWER FOR ALL NERVE LESIONS central lesions: tumours: due to direct invasion of the third nerve nucleus due to raised intracranial pressure vascular: caused by a brainstem lesion demyelination peripheral causes include: compressive lesions: tumour aneurysm, often the posterior communicating artery basal meningitis nasopharyngeal carcinoma orbital lesions e.g. Tolosa-Hunt syndrome infarction: often spares the pupillary reflex, when the condition is termed a "medical third nerve palsy" often caused by diabetes mellitus

132
This xray and CT are showing the same sign… what is it?

133
Porcelain gallbladder
Porcelain gallbladder is a calcification of the gallbladder believed to be brought on by excessive gallstones but more studies are necessary to determine the exact cause. Porcelain gallbladder often results in a diagnosis of gallbladder cancer. The association with the two is uncertain; gallbladder cancer is rare, but is almost always found with porcelain gallbladder. The prognosis is poor, in that the gallbladder is usually asymptomatic until the cancer has spread.

134
A 53-year-old man presented with low-grade fever and abdominal pain
A 53-year-old man presented with low-grade fever and abdominal pain. A tender, erythematous umbilical 3-cm mass is shown.

135
Strangulated umbilical hernia
In a strangulated hernia, the blood supply of the contents of the hernia, e.g. bowel or omentum, is cut off. It is commonest at the neck of the sac. The region becomes ischaemic and subsequently gangrenous. Gangrene can lead to perforation of the bowel with ensuing peritonitis. When a loop of gut is strangulated, there will also be intestinal obstruction.

136
This 23 year old woman is complaining of rectal pain
This 23 year old woman is complaining of rectal pain. She denies any other symptoms

137
What is this xray showing?
Patient presented with an acute abdomen with the sudden onset of severe upper abdominal pain, nausea and vomiting.

138
Gallstone pancreatitis

139
Describe how you would investigate and manage this patient
A 50-year-old man presented with a 2-day history of atraumatic right middle finger swelling, redness, and pain. There was tenderness and swelling of the proximal interphalangeal joint. ESR was elevated. The leukocyte count normal. Describe how you would investigate and manage this patient

140
Septic arthritis URGENT ADMISSION!!! ASPIRATE!!!! blood cultures
full blood count for leucocytosis erythrocyte sedimentation rate C-reactive protein aspiration of synovial fluid - usually purulent with a neutrophil count above 50,000 per mm3, and low glucose concentration anti-streptolysin O titre Tx flucloxacillin and amoxicillin empirically!

141
A 65-year-old woman presented to the emergency department because a friend was concerned that the patient was having a stroke. The patient was asymptomatic other than complaints of a pestering nonproductive cough. What is wrong?

142
Subconjuntival haemorrhage
This presents as a bright red patch under the conjunctiva following rupture of a small conjunctival vessel. It may arise spontaneously, following slight trauma, or as a result of local congestion due to coughing or sneezing. In head injury, blood from a fracture at the base of the skull may travel through the floor of the orbit and into the subconjunctival space. The condition is usually unilateral. Recurrent or bilateral subconjunctival haemorrhage suggests hypertension or blood dyscrasias.

143
A 28-year-old woman complained of a foreign-body sensation, pain and redness of the outer lower quadrant of her left eye of 2-day's duration.

144
episcleritis unilateral in two-thirds of cases.
It is benign and self-limited. 30% are associated with general medical conditions such as collagen disease, herpes zoster, gout and syphilis. There are two types - simple and nodular. Simple episcleritis is characterized by a very acute onset. It is mild, sectoral, recurrent and resolves rapidly. The nodular form presents as a localised, raised mobile area of inflammation near the limbus. The nodules may be single or multiple and usually recur. About 15% of patients develop a mild iritis. Episcleritis is distinguished from conjunctivitis by the localised response and the lack of palpebral conjunctival involvement. oral non-steroidal anti-inflammatory drug (NSAID).
.")
145
A 2- year-old girl presented with fever, erythema, and swelling of the left upper eyelid. There were no visual symptoms or proptosis.

146
periorbital cellulitis
The findings shown are suggestive of acute periorbital cellulitis, or more accurately, preseptal cellulitis, an infection confined to the soft tissues of the eyelid. Bacteriology of preseptal cellulitis includes those bacteria that cause sinusitis (Haemophilus influenzae, Streptococcus pneumoniae, Moraxella catarrhalis, S pyogenes); skin flora from trauma (Staphylococcus aureus and group A Streptococcus); and idiopathic (H influenzae type B, S pneumoniae). (L.S.)
; skin flora from trauma (Staphylococcus aureus and group A Streptococcus); and idiopathic (H influenzae type B, S pneumoniae). (L.S.)")
147
A 20-year-old man presented with a brief loss of consciousness following a fall from standing height. He had a brief lucid interval then became progressively less responsive. This is his CT scan

148
Extradural haematoma The characteristic appearance of a CT of an extradural haemorrhage is of a biconvex, lozenge shaped area of increased density. Spread is limited by the adhesion of the dura to the skull. A midline shift with compression of the ipsilateral ventricle may be apparent.

149
A 25-year-old man was brought to the emergency department after having been hit in the left lateral chest with a jet ski. He was short of breath and hypotensive.

150
Tension pneumothorax Should not have obtained an Xray… emergency situation

151
A 37-year-old homeless man presented to the emergency department with a 3-week history of neck pain that had started after a motor vehicle accident

152
Subluxation of c1 on c2 Cervical subluxation is a flexion injury. There is no bony damage but the soft tissues are extensively damaged and the posterior ligaments torn. The affected vertebra hinges forward on the one below, opening up the interspinous space posteriorly then falls back again. Radiologically there may be an increased gap between the spines of affected vertebra, but the film often appears normal - flexion radiology may be required to demonstrate the instability. Treatment is usually a collar for six weeks. However, if there is persistent instability a posterior spinal fusion may be required.

153
What is wrong with this girl…be specific!

154
Bell’s palsy It is a lower motor neurone palsy usually diagnosed by exclusion. Typically, presentation is with facial distortion, loss of taste, hyperacusis and a watery eye. Bell's palsy was previously considered as an idiopthic lower motor neurone nerve palsy but there has been increasing evidence to suggest that the main cause of Bell's palsy is latent herpes viruses (herpes simplex virus type 1 and herpes zoster virus), which are reactivated from cranial nerve ganglia
, which are reactivated from cranial nerve ganglia.")
155
Patient is asked to look left

156
Right VI nerve palsy Tumour Trauma Demyelination Ischaemia (stroke)
Raised intracranial pressure FALSE LOCALISING SIGN

158
Left CN 9 palsy Uvula deviates away from the affected side

160
Left CN 12 palsy Tongue deviates towards side of lesion

161
What is wrong with this lil lady?

162
Trochlear CN IV palsy Diplopia
abnormal head posture - head tilted towards the normal side, face rotated towards the normal side, and the chin is depressed. The affected eye is higher than its fellow. positive head tilt test - affected eye moves higher when the head is tilted towards the affected side CNIV is thinnest and has the longest intracranial course damaged easily by stroke and trauma

163
What is wrong with these miserable looking folk?

164
Myasthenia gravis Myasthenia gravis is an acquired autoimmune disorder characterised by weakness, typically of the periocular, facial, bulbar, and girdle muscles. Associated with serum IgG antibodies to acetylcholine receptors in the postsynaptic membrane of the neuromuscular junction. Classically, the muscles are easily fatigued. It affects 5 people in every Non-thymoma cases have a peak incidence at years and again, at years of age; those associated with thymoma have a peak incidence at years of age.

165
Diff diagnosis Lambert-Eaton syndrome - muscles are not fatiguable - contraction leads to increased strength - reflexes are diminished congenital myasthenia botulism motor neurone disease (MND) - note that eye is very rarely involved in MND
 - note that eye is very rarely involved in MND.")
166
Myasthenia gravis Exacerbated by: exercise, barbituates, steroids
improvement in strength after administering a short-acting anticholinesterase drug, for example, edrophonium chloride. acetylcholine receptor antibodies Management oral anticholinesterase medication, e.g. pyridostigmine or neostigmine (symptomatic improvement). if there is life-threatening or respiratory weakness developing in treated patients, then this usually requires immediate control of the airway, treatment of any underlying infection, and a course of plasma exchange thymectomy - required if there is a thymoma because of the risk of local infiltration. Also occasionally undertaken in other non-thymoma patients with myasthenia immunosuppression with corticosteroids +/- cytotoxic agents is also highly effective in inducing remission of disease and may be necessary preliminary to surgery in patients with severe disease. plasma exchange
. if there is life-threatening or respiratory weakness developing in treated patients, then this usually requires immediate control of the airway, treatment of any underlying infection, and a course of plasma exchange. thymectomy - required if there is a thymoma because of the risk of local infiltration. Also occasionally undertaken in other non-thymoma patients with myasthenia. immunosuppression with corticosteroids +/- cytotoxic agents is also highly effective in inducing remission of disease and may be necessary preliminary to surgery in patients with severe disease. plasma exchange.")
167
Lambert eaton Lambert-Eaton myasthenia is a presynaptic myasthenic syndrome characterised by impaired release of acetycholine from nerve terminals. 60% of patients have small cell lung carcinoma. Electromyography shows increased evoked potentials after repeated galvanic stimulation (the opposite occurs in myasthenia gravis). Symptoms improve with exercise
. Symptoms improve with exercise.")
169
Right sided horners syndrome
slight ptosis pupillary miosis: due to paralysis of the sympathetically innervated Muller's muscle which normally dilates the pupil anhydrosis over the forehead Pancoasts tumour, carotid body tumour infection, vasculitis, demyelinating disease MS

170
What is wrong with this chap
What is wrong with this chap? Ignore the white thing I don’t know what that is

171
hydrocephalus Communicating hydrocephalus
obstruction to CSF flow from outside the ventricular system, usually in the subarachnoid space. All the ventricles show a generalised dilatation on a CT scan. It is safe to perform a lumbar puncture Non-communicating hydrocephalus obstruction to CSF flow within the ventricular system. Fluid accumulates proximal to the site of the blockage causing dilation.

172
Management of hydrocephalus
The cause of hydrocephalus should be eliminated if possible - e.g. colloid cysts of the 3rd ventricle, intraventricular meningioma, other obstructive causes. Otherwise, relieve pressure by shunting, or if the patient is rapidly deteriorating, by draining the ventricle directly. Endoscopic third ventriculostomy has become a more recent, and important, treatment option for occlusive hydrocephalus associated with aqueductal stenosis or space-occupying lesions of or around the posterior third ventricle and upper brainstem (1,2): this procedure appears to be more successful in adults than in young children it is efficacious in both previously shunted and non shunted patient complication and mortality rates compare favorably with those for shunts has also been increasingly used as an alternative treatment option for shunt complications Lumbar puncture may be used to relieve pressure in an acute communicating hydrocephalus.
: this procedure appears to be more successful in adults than in young children. it is efficacious in both previously shunted and non shunted patient. complication and mortality rates compare favorably with those for shunts. has also been increasingly used as an alternative treatment option for shunt complications. Lumbar puncture may be used to relieve pressure in an acute communicating hydrocephalus.")
173
NPH Normal pressure hydrocephalus is a form of communicating hydrocephalus in which the intracranial pressure, as measured by lumbar puncture, is normal or intermittently raised. Failure to reabsorb CSF is compensated by reduced production. gait apraxia progressive dementia with memory loss sphincter disturbance resulting in incontinence

174
What has happened here? What are the risk factors for this?

175
L Middle cerebral artery ischaemic stroke
Hypodense (dark) area on CT No midline shift Non-modifiable risk factors increasing age male gender Afro-Caribbean descent positive family history of stroke Modifiable Risk factors for stroke smoking diabetes mellitus diet: high salt intake high fat intake low potassium intake low vitamin intake excess alcohol intake morbid obesity low physical exercise low body temperature cholesterol
 area on CT. No midline shift. Non-modifiable risk factors. increasing age. male gender. Afro-Caribbean descent. positive family history of stroke. Modifiable Risk factors for stroke. smoking. diabetes mellitus. diet: high salt intake. high fat intake. low potassium intake. low vitamin intake. excess alcohol intake. morbid obesity. low physical exercise. low body temperature. cholesterol.")
177
Haemorrhagic stroke Note the high-density haemorrhage within the low density of the oedematous, infarcted region in the right hemisphere. Haemorrhage is evident from its onset on CT scanning.

178
What is this?? What factors predispose to this condition? How would you manage?

179
Subdural haemorrhage The characteristic picture of a CT scan of a subdural haemorrhage is one of a biconcave, concentric shaped, area of increased density spreading around the surface of the cerebral hemisphere. The contralateral ventricle may dilate owing to obstruction at the foramen of Munro. After days, the subdural haematoma becomes isodense with brain. Later it becomes relatively hypodense.

180
Subdural haematoma Subdural haemorrhages result from rupture of cortical bridging veins. These connect the venous system of the brain to the large intradural venous sinuses and lie relatively unprotected in the subdural space. any factor that stretches the bridging veins: cerebral atrophy, e.g. elderly low CSF pressure after shunting, for example for long- standing hydrocephalus or a fistula alcoholism coagulation disorder or anticoagulation therapy patients in whom conscious level is depressed: evacuate haematoma through 2-3 burr holes, and irrigate cavity with saline nursing in the head down position is recommended to prevent recollection patients in whom conscious level is not depressed: consider conservative measures - steroid treatment over several weeks

181
How do you diagnose and treat this condition?

182
Multiple myeloma a malignant neoplasm of plasma cells that arises in the bone marrow. Presentation is with anaemia, bone pain, skeletal destruction, pathologic fractures, or Bence Jones proteinuria. M (monoclonal) band on serum electrophoresis Tx- cytotoxic chemo and supportive ,measures
 band on serum electrophoresis. Tx- cytotoxic chemo and supportive ,measures.")
183
What is wrong with these chaps? What features are common?

184
Parkinson’s disease tremor bradykinesia rigidity
impaired postural reflexes shuffling gait expressionless, unblinking face Pill-rolling tremor slurred monotonous speech small handwriting increased salivation and dribbling Ali actually has parkonsonsim due to dopamine depletion within the basal ganglia (boxing knocked it all out)
")
185
What is wrong with this chap?

186
Myotonic dystrophy characterised by myotonia and muscular atrophy.
Inheritance is AD. The incidence is 5 per with onset between 15 and 40 years, although it may present as early as birth. The causal gene is on chromosome 19. The disease is slowly progressive and is characterised by cataract formation, hypogonadism, frontal balding and cardiac disorders. There is weakness, wasting and myotonia of involved muscles. Wasting of the stenocleidomastoids produces the classical swan-necked appearance

187
Loss of lower limb refelxes and extensor plantar response noted in this 15 year old boy…

188
Friedreich's ataxia most common inherited ataxia. prevalence of 1 in inheritance is ar progressive gait and limb ataxia, loss of proprioception, pyramidal weakness and dysarthria. Extra-neurological involvement includes: hypertrophic cardiomyopathy in most patients diabetes mellitus in 10% pes cavus and kyphoscoliosis Onset is usually during adolescence.

189
What is wrong with this 14 yr old boy ?
He has foot drop and reduced reflexes

190
Charcot marie tooth AD condition characterised by slowly progressive sensorimotor neuropathy. It is the most commonly inherited peripheral neuropathy in the UK. type I: a demyelinating sensorimotor neuropathy early onset, typically in the first decade presentation with walking difficulties and pes cavus associated deformities include eqinovarus foot and kyphoscoliosis wasting occurs: distally before proximally in the legs before the arms distal wasting may produce the classical inverted champagne bottle deformity there is generalised areflexia there may be cerebellar ataxia of the arms respiratory muscles may be weak nerve conduction is slowed to less than 38 m/sec peripheral nerves may be palpably thickened

191
This girls leg is wasted, weak, with absent knee and ankle reflexes
What is your differential diagnosis?

192
polio Poliomyelitis is a notifiable infectious viral illness affecting the central nervous system. Poliomyelitis is an acute illness that follows invasion through the gastrointestinal tract by one of the three serotypes of polio virus (serotypes 1, 2 and 3) LMN lesion Sensation is unaffected by this condition. When a badly- paralysed limb is picked up it has a floppy feel which, in the presence of normal sensation, is characteristic of the residual paralysis from poliomyelitis.
 LMN lesion. Sensation is unaffected by this condition. When a badly- paralysed limb is picked up it has a floppy feel which, in the presence of normal sensation, is characteristic of the residual paralysis from poliomyelitis.")
193
differential Polio Trauma Botulism paraneoplastic

194
What is this? What conditions is it associated with?

195
Berry aneurysm adult polycystic kidney disease Ehlers-Danlos syndrome
coarctation of the aorta mostly remain asymptomatic throughout life vary in size, most symptomatic aneurysms are >1 cm often occur at vessel bifurcations cause 80% of subarachnoid haemorrhages If >1cm clip them prophylactically If <1cm leave them (risk of surgery>risk of bleed)
")
197
Optic atrophy Full moon Featureless disc retinal lesions: optic nerve:
central retinal artery or vein occlusion retinitis pigmentosa tobacco / nutritional - end result of tobacco amblyopia optic nerve: chronic glaucoma - most common of all causes ischaemic optic neuropathy secondary to papilloedema or papillitis secondary to optic neuritis or retrobulbar neuritis trauma - severing, avulsion, contusion, surgery familial - Leber's disease, Friedreich's ataxia pressure on optic nerve: tumour - glioma, meningioma Paget's disease aneurysm of the anterior circle of Willis chiasmal compression: pituitary tumour, craniopharyngioma, suprasellar meningioma, aneurysm, stroke

199
Acute glaucoma cupping
Tx of acute closed angle glaucoma reduction of intra-ocular pressure by reducing aqueous secretion – acetazolamide pupillary constriction - topical pilocarpine or thymoxamine, an alpha receptor antagonist surgical or laser iridectomy - once the attack has been controlled - rarely surgery may be undertaken as an emergency procedure if medical management fails

201
papilloedema intracranial space-occupying lesions – tumours, cerebral abscesses; subdural haematoma hydrocephalus e.g. subarachnoid haemorrhage, meningitis, head injury venous sinus thrombosis benign intracranial hypertension malignant hypertension central retinal venous occlusion, ischaemic optic neuropathy, optic neuritis chronic carbon dioxide retention

203
Pan retinal photocoagulation
Treatment of diabetic nephropathy

205
maculopathy Reduced vision

206
What would this patient complain of?

207
Retinitis pigmentosa Night blindness peripheral visual loss
pigmentary retinopathy Seen in Laurence-Moon-Biedl syndrome

209
Tuberous sclerosis congenital disease characterised by hamartomatous lesions in the skin, nervous system and internal organs, principally heart and kidney. Triad of adenoma sebaceum: actually an angiofibroma with passive involvement of sebaceous glands epilepsy mental retardation

210
What is this? With what is it associated?

211
Same again…

212
Osler weber rendu Hereditary haemorrhagic telangiectasia is a rare AD condition where multiple small telangiectases occur on the skin and mucous membranes, most commonly on the lips and the tongue. Lesions are also often scattered over the pulps of fingers. Epistaxis is the most common complaint. When telangiectases are present in the gastrointestinal tract they may cause chronic blood loss with iron deficiency anaemia. Occasionally there may be torrential bleeding. Arteriovenous malformations may occur in the: liver lungs, causing: clubbing murmurs paradoxical emboli

214
Scurvy Gingival haemorrhage Vitamin C deficiency
anaemia, spongy gums, a tendency to mucocutaneous haemorrhages, and brawny induration of calf and leg muscles, poor wound healing Tx Vitamin C mg/day orally.

215
What is this? What causes it?

216
Gingival hyperplasia acute leukaemia – typically AML Drugs: scurvy
phenytoin nifedipine cyclosporin scurvy pregnancy gingivitis

217
What is wrong with this patient and what is your immediate management
55yr old man was started on ACE-I for his hypertension 2 weeks ago. His blood pressure is now higher than 2 weeks ago and his creatinine is raised

218
Renal artery stenosis STOP ACE-I !
This condition may result in secondary hypertension and secondary hyperaldosteronism. Other possible features include: coexistant cerebrovascular, cardiovascular or peripheral vascular disease deterioration of renal function following treatment with ACE inhibitor abdominal bruit; signs of coexistant vascular disease e.g. carotid or femoral bruit; absent peripheral pulses Tx - balloon dilatation

219
This patient presented with tiredness and weight loss
This patient presented with tiredness and weight loss. ON examination his tongue has this appearance and he has proteinuria, oedema and hepatosplenomegaly

220
Macroglossia in amyloidosis
In amyloidosis, there is extracellular deposition of fibrillar protein. This may be in a localized deposition or widely distributed throughout the body. Amyloid fibrils stain with Congo red and show apple green birefringence in polarized light. Cytotoxic and immunosuppressive drugs have been used to treat amyloidosis, but often with poor results. Improvement may be attained by treatment of an underlying cause.

221
What is wrong with this patient?

222
HEPATOMEGALY MASSIVE MODERATE MILD Secondary metastasis HCC
alcoholic liver disease with fatty infiltration (more likely to have shriveled liver) myeloproliferative disease malaria MODERATE right heart failure haemochromatosis haematological disease: chronic myeloid leukaemia lymphoma fatty liver - secondary to diabetes, toxins MILD hepatitis biliary obstruction
 myeloproliferative disease. malaria. MODERATE. right heart failure. haemochromatosis. haematological disease: chronic myeloid leukaemia. lymphoma. fatty liver - secondary to diabetes, toxins. MILD. hepatitis. biliary obstruction.")
224
Hepatosplenomegaly infection: haematological disease:
acute viral hepatitis infectious mononucleosis cytomegalovirus haematological disease: leukaemia myeloproliferative disease lymphoma pernicious anaemia sickle cell anaemia thalassaemia chronic liver disease and portal hypertension: chronic active hepatitis amyloidosis acromegaly systemic lupus erythematosus

225
What is this condition and how would you treat?
Ca and PO4 are normal Alk Phos is raised

226
Paget’s It is characterised by excessive and disorganised bone resorption and formation. Analgesia Bisphosphonates Surgery for fractures/ joint replacement

227
What is the likely cause of this boy’s enlarged abdomen who presented with fever, chills and sweating?

228
Splenomegaly MASSIVE SPLENOMEGALY : MODERATE SPLENOMEGALY
chronic myeloid leukaemia myelofibrosis primary lymphoma of the spleen malaria kala-azar (visceral form of leishmaniasis ) MODERATE SPLENOMEGALY portal hypertension: splenic/portal vein thrombosis hepatic cirrhosis Budd-Chiari syndrome lymphocytic leukaemias thalassaemias
 MODERATE SPLENOMEGALY. portal hypertension: splenic/portal vein thrombosis. hepatic cirrhosis. Budd-Chiari syndrome. lymphocytic leukaemias. thalassaemias.")
229
What emergency surgery was performed here?

230
Liver transplant Possible indications in an adult include:
fulminant or subacute liver failure: paracetamol poisoning viral hepatitis end-stage liver cirrhosis: alcoholic liver disease chronic active hepatitis primary biliary cirrhosis

232
caput Medusae It is a sign of severe portal hypertension with portal-systemic shunting through the umbilical veins

233
What is this and how many are we allowed?

234
Spider naevi None are normal for a man Less than 5 in women
They are found in the distribution of the superior vena cava i.e. on the arms, neck, and chest wall. cirrhosis - most frequently, alcoholic oestrogen excess - usually in association with chronic liver disease; part of normal hepatic function is the inactivation of oestrogens hyperthyroidism rheumatoid arthritis - rarely

235
87 year old man presented with abdominal pain and a 4 wk history of constipation
What features would you expect on examination? How would you treat this man?

236
Sigmoid volvulus - 'bent inner-tube' - inverted U - sign
marked abdominal distension sudden onset of colicky pain absolute constipation and no passage flatus for at least 24 hours abdomen is distended and tympanic left ilac fossa tenderness rectal examination reveals a capacious, empty rectum Tx immediate management: sigmoidoscopy and air insufflation there is a gush of liquid faeces and flatus as the obstruction is relieved High fibre diet and review medication

238
Caecal volvulus A caecal volvulus occurs when there is twisting of the bowel at the caecum and resultant intestinal obstruction. Distention of the caecum ensues to the extent that the volvulus can be felt as a palpable mass. The patient may have vomiting, abdominal pain and constipation. The classical radiological appearance is the 'comma' sign - there is a gas-filled ileum and caecum. Treatment is by decompression and resection, or fixing of the caecum to the posterior abdominal wall.

239
What does this xray show?
With what conditions is it associated?

240
Ulcerative colitis primary sclerosing cholangitis Cholangiocarcinoma
sacro-iliitis and ankylosing spondylitis pyoderma gangrenosum, erythema nodosum anterior uveitis episcleritis Increased risk colon cancer Toxic megacolon

241
What does this colonoscopy show?

242
crohns

243
What is this close up of a barium enema showing?
What disease has caused this?

244
String Sign Crohns disease
Small-bowel follow-through study demonstrates the string sign in the terminal ileum. pseudodiverticula of the antimesenteric wall of the terminal ileum, secondary to greater distensibility of this less-involved segment of the wall

245
What is this? How would you treat?

246
Small bowel obstruction with fluid levels
Drip and suck

248
pneumoperitoneum

249
What does this xray show?
A 23yr old man presented to A and E with fever, abdominal distension and tenderness On examination he was tachycardic and had postural hypotension

250
Toxic megacolon life-threatening complication of inflammatory or infectious colitis. segmental, non-obstructive dilatation of the colon to greater than 6 cm diameter systemic toxicity Xray dilatation of the lumen from 6-15 cm the most common sites of dilatation are the right and transverse colons there is thickening of the colonic wall with disruption of the normal haustral pattern there may be multiple air-fluid levels

252
Diverticular disease Management – high fibre diet, antispasmodics, laxatives Complications: peritonitis, fistula formation, persistent haemorrhage, pericolic abscess formation, intestinal obstruction, and repeated episodes of diverticulitis that are resistant to medical therapy.

253
What sign is shown? What is the most likely cause?

254
Apple core sign Stricture most likely due to colon cancer

255
What is wrong with this patient?

256
Dextrocardia/Situs Inverus
Kartagener's syndrome bronchiectasis (also seen in Xray) sinusitis dextrocardia It is associated with a defect in cilia function and now is termed as synonymous with primary ciliary dyskinesia. The situs inversus is thought to be a developmental consequence of failure of ciliary action in the formation of the gastrointestinal tract and other stuctures.
 sinusitis. dextrocardia. It is associated with a defect in cilia function and now is termed as synonymous with primary ciliary dyskinesia. The situs inversus is thought to be a developmental consequence of failure of ciliary action in the formation of the gastrointestinal tract and other stuctures.")
257
What is the diagnosis? This patient presented with gradual onset, intermittent dysphagia. He also has had recurrent chest infections

258
Achalasia MANAGEMENT intrasphincteric injection of botulinum toxin
neuromuscular failure of relaxation at the lower end of the oesophagus with progressive dilatation, tortuosity, incoordination of peristalsis and often hypertrophy of the oesophagus above. MANAGEMENT intrasphincteric injection of botulinum toxin endoscopic hydrostatic or pneumatic dilatation Heller's operation - cardiomyotomy - success rate of about 90% in those who do not respond to dilatation

259
What is this upper GI endoscopy showing?
What appearance would it have on barium swallow?

260
Oesophageal candidiasis
Furry oesophagus on swallow

261
This patient presented with retrosternal chest pain
What is the diagnosis?

262
Corkscrew Oesophagus Altered motility of the oesophagus (sometimes loosely referred to as "spasm") can be a cause of chest pain. The rare condition of diffuse oesophageal spasm (seen radiologically as a "corkscrew oesophagus") is associated with pain,
 is associated with pain,")
263
What is wrong with this 55 yr old publican who has long standing recurrent abdominal pain and weight loss

264
Chronic pancreatitis Plain film with extensive calcification in duct system of a patient with chronic pancreatitis secondary to alcohol

266
Apparently this is a “leather bottle stomach”
This is it out of the Body Caused by gastric cancer

268
Oesophageal varices

270
Peutz jeghers multiple hamartogenous polyps of the gastrointestinal tract - most often in the small bowel but may occur affect any portion of the GI tract mucocutaneous pigmentation - mainly, of the lips, buccal mucosa, genitalia, hands and feet

272
Oral hairy leukoplakia
This is a lesion on the tongue that may be seen in immunocompromised patients.It appears to be the result of a proliferation of Epstein-Barr virus, possibly associated with Papilloma virus in the superficial layers of the squamous epithelium of the tongue.

273
What is this upper GI endoscopy of dueodenum showing
What is this upper GI endoscopy of dueodenum showing? How else would you investigate this?

274
Coeliac disease Endoscopic still of duodenum of patient with coeliac disease showing scalloping of folds ENDOMYSIAL ANTIBODIES ENDOSCOPY AND JEJUNAL BIOPSY Bloods – anaemia, iron, folate, PT prolonged DEXA- looking for damage due to low Ca Tx gluten free diet, vit + calcium + iron supplements, pneumococcus vaccine

276
Biopsy of small bowel showing coeliac disease manifested by blunting of villi, crypt hyperplasia, and lymphocyte infiltration of crypts,

277
This man has a 2 month history of weight loss
This man has a 2 month history of weight loss. He is itchy, has no pain and has a palpable gall bladder

278
Head of pancreas Ca Presents with painless obstructive jaundice, weight loss and anorexia Gallbladder is palpable (Courvoisiers Law) painless jaundice + palpable gallbladder is not gallstones!!!! US/CT for diagnosis (CT for staging) Tx Whipples (pancreatoduodenectomy) Chemo Most present with metastatic disease with crap prognosis (6months mean survival)
 Tx Whipples (pancreatoduodenectomy) Chemo. Most present with metastatic disease with crap prognosis (6months mean survival)")
280
Sclerosing cholangitis
Beads on a string Associated with UC

282
Acute otitis media common causes are URTI (viral or bacterial)
clinical features ear pain ear rubbing cloudy white/yellow eardrum (pus in middle ear) bulging eardrum distinctly immobile eardrum distinctly red eardrum 80% recover in around three days without antibiotics complications are rare Tx paracetamol and Inbuprofen (watchful waiting)
 bulging eardrum. distinctly immobile eardrum. distinctly red eardrum. 80% recover in around three days without antibiotics. complications are rare. Tx paracetamol and Inbuprofen (watchful waiting)")
284
Glue ear Secretory otitis media, or `glue ear', is the most frequent cause of hearing problems in children. accumulation of serous or viscous fluid within the middle ear pain conductive hearing loss dull / dark blue/ grey appearance of tympanic membrane Rinne's test negative; Weber's test - sound heard loudest in the deafer ear.

286
Grommets The function of a grommet is to ventilate the middle ear, rather than drain it. Grommets thus replace the function of the blocked eustachian tube in glue ear and improve hearing. use of grommets in glue ear (otitis media with effusion) offer only small benefits potentially adverse effects on the tympanic membrane are common after grommet insertion ears treated with grommets had an additional risk for tympanosclerosis one to five years later
 offer only small benefits. potentially adverse effects on the tympanic membrane are common after grommet insertion. ears treated with grommets had an additional risk for tympanosclerosis one to five years later.")
287
This 5 year old boy presented with fever, malaise, sore throat and otalgia
What is the differential diagnosis? How would you manage this condition?

288
Acute tonsilitis Differential – rest
soluble paracetamol held in the mouth and then swallowed eases the discomfort (1) the patient must be encouraged to drink to prevent dehydration antibiotics are unnecessary for most patients with sore throat as it is a self-limiting condition, which resolves by one week in 85% of people, whether it is due to streptococcal infection or not
 the patient must be encouraged to drink to prevent dehydration. antibiotics are unnecessary for most patients with sore throat as it is a self-limiting condition, which resolves by one week in 85% of people, whether it is due to streptococcal infection or not.")
289
The Centor criteria tonsillar exudate
tender anterior cervical lymph nodes absence of cough history of fever Then treat with antibiotics as it could be Group A beta-haemolytic streptococcus infection (erythromycin as amoxicillin will cause rash in infectious mononucleosis)
")
292
Torsion of testis

293
The patient is a five year old boy who presented with a febrile urinary tract infection (UTI).
His CT and US are shown. What is diagnosis?

294
Acute pyelonephritis On CT, an edematous left kidney is seen with multiple large areas of decreased enhancement in the periphery Ultrasound images reveal an enlarged left kidney with heterogeneous echo texture as well as several discrete areas of hyopechogenicity

296
Staghorn calculi

298
nephrocalcinosis

300
Right hydronephrosis

302
Chronic pancreatitis

304
gallstones Note that no contrast was necessary to acquire this image; sequence depicts fluid which is either stagnant or flowing slowly.

306
What sign is being shown?
What other features are likely to be present? would you treat this problem?

307
Trousseau’s sign Paraesthesia, tetany, psychosis, convulsions, long QT interval Chvostek’s sign (tapping on facial nerve causes twitch mild tetany - oral calcium supplements severe tetany - intravenous calcium gluconate, 10 ml (2.32 mmol) calcium gluconate 10% IV over 10 minutes. vitamin D - either if primary disease is due to vitamin D or, to ensure adequate absorption of calcium. calciferol for simple vitamin D deficiency alfacalcidol or calcitriol if in renal failure - offer no advantage over calciferol for simple deficiency
 calcium gluconate 10% IV over 10 minutes. vitamin D - either if primary disease is due to vitamin D or, to ensure adequate absorption of calcium. calciferol for simple vitamin D deficiency. alfacalcidol or calcitriol if in renal failure - offer no advantage over calciferol for simple deficiency.")
308
This 38 yr old woman with asthma has presented with a purpuric rash and haematuria, proteinuria and raised BP What is the diagnosis?

309
Churg Strauss The six classification criteria asthma
peripheral blood eosinophilia neuropathy pulmonary infiltrates paranasal sinus involvement biopsy showing vasculitis with extravascular eosinophils Laboratory diagnosis is based on tissue biopsy and the antineutrophil cytoplasmic antibody (ANCA) test. About 25% of patients have cANCA and about 50% have pANCA This syndrome is also characterised by elevated levels of IgE. Glomerulonephritis is a result of the vascultits Tx high dose corticoteroids
 test. About 25% of patients have cANCA and about 50% have pANCA. This syndrome is also characterised by elevated levels of IgE. Glomerulonephritis is a result of the vascultits. Tx high dose corticoteroids.")
310
This 50 year old man who enjoys a drink and smokes 10 cigs per day presents with epigastric pain and weight loss. What is being shown here and how would you investigate?

311
Virchow’s node Gastric cancer
endoscopy and biopsy: investigation of choice barium meal; suspicious findings: space occupying mass rigidity of adjacent gastric wall greater curve ulcer an ulcer with irregular borders and disruption of normal mucosal folds contracted, non-distensible stomach - linitis plastica fundic tumours are difficult to evaluate because of poor filling chest x-ray, liver enzymes, and liver ultrasound for evidence of metastases anaemia in as much as 50% of all cases faecal occult blood test positive in the vast majority of subjects

312
This 70 year old man presented with a few weeks history of difficulty swallowing and weight loss
What other investigations would you perform? What is his prognosis? What would you do for him in terms of swallowing difficulty?

313
Oesophageal carcinoma
Adenocarcinoma (lower 1/3) Apple core sign CT staging should be performed 5 year survival 10% (asymptomatic until late stage) Oesophageal stenting (palliative)
 Apple core sign. CT staging should be performed. 5 year survival 10% (asymptomatic until late stage) Oesophageal stenting (palliative)")
314
Risk factors for Oe cancer
AGE Diet (far eastern diet) Smoking Acid reflux Barret’s oesophagus (30-40X) Achalasia Tylosis Plummer-vinson (fe deficiency oesophageal web) also called paterson-kelly-brown
 Smoking. Acid reflux. Barret’s oesophagus (30-40X) Achalasia. Tylosis. Plummer-vinson (fe deficiency oesophageal web) also called paterson-kelly-brown.")
315
What is this upper GI endoscopy showing?
What symptoms will this 70 yr old man be experiencing?

316
Oesophageal Ca Dysphagia Vomiting/ food regurg Chest pain Odynophagia
Wt loss/ anorexia Haematemesis Hoarse voice/ coughing/ aspiration of saliva into lung

317
What is being shown here?

318
Hiatus hernia with pneumoperitoneum SLIDING
Sphincter at bottom of oesophagus and top of stomach slides through hiatus in diaphragm. May slide up and down ROLLING Part of stomach protrudes up through a hole in the diaphragm next to the oesohagus… can become strangulate. Less common

319
This 34 yr old male patient presented with malaise, weight loss, apthous ulcers and this intensely itchy skin rash

320
Dermatitis herpetiformis
Dermatitis herpetiformis is an intensely itching subepidermal vesicular blistering condition that usually develops in the 3rd or 4th decade. Men>women. intensely pruritic, vesicular rash chiefly affecting the extensor surfaces of shoulders, buttocks, knees, forehead and scalp, sparing the mucosae. Small blisters are rarely seen since they are rapidly excoriated, leaving raw papules. Vesicles are frequently grouped, as those of the true herpes virus, hence the name 'herpetiformis.‘ About 90% of patients with dermatitis herpetiformis will have coeliac disease Tx - dapsone, in doses of mg/day for itching Gluten free diet Topical steroids

321
How would you exanine this patient?

322
Determining if indirect or direct inguinal hernia
Only true way to know is at surgery Reduce hernia Place finger over internal ring with 2 fingers When standing if no protrusion hernia is likely indirect. If protrusion present is direct.

323
How would you examine this patient?

324
DO NOT EXAMINE ANAL FISSURES ARE EXTREMELY PAINFUL!!!
There is a prominent skin tag present also in this photo

325
What is the diangosis? How would you treat?

326
Prolapsed internal haemorrhoids
CONSERVATIVE TX ensuring the perineum is dried and washed after defaecation: digital replacement of prolapsed haemorrhoids: local anaesthetic creams and ointments treatment aimed at reducing spasm of the internal anal sphincter: nitroglycerine ointments: glyceryl trinitrate % (unlicensed) botulinum toxin injection SURGICAL TX sclerotherapy rubber band ligation photocoagulation cryotherapy HAEMORRHOIDECTOMY LORD’S STRETCH!!!! ANAL DILATATION UNDER GA
 botulinum toxin injection. SURGICAL TX. sclerotherapy. rubber band ligation. photocoagulation. cryotherapy. HAEMORRHOIDECTOMY. LORD’S STRETCH!!!! ANAL DILATATION UNDER GA.")
327
HOW WOULD YOU TREAT THIS?

328
HYDROCOELE Tx childhood hydrocoeles only if they persist after 1 yrs old. The procedure is as for an inguinal hernia - open the sac, inspect the testis for abnormalities, ligate and divide the patent processus vaginalis. In adults, primary hydrocoeles may be treated: conservatively - reassure the patient and provide a scrotal support. by aspiration - use a sterile needle and syringe. Clear, pale yellow fluid should be drained; fluid that is bloodstained suggests trauma or other underlying pathology. Following aspiration, the testis should be palpable. A sclerosant such as phenol may then be injected to stop fluid from reaccumulating, otherwise, periodic aspiration may be necessary. A hydrocoele should not be tapped if there is any suspicion of tumour - in the case of a tumour, aspiration may result in spread of malignant cells. by operation - if the diagnosis is in doubt, the hydrocoele is large, or fluid repeatedly reaccumulates after drainage. Once the fluid has been removed, the testis is examined for abnormalities.

330
Neuropathic ulcer (diabetes pt)
")
331
What is this? How would the patient who has had this removed have been investigated initially?

332
Ruptured appendix Acute appendicitis is usually a clinical diagnosis
full blood count - leukocytosis is generally present urea and electrolytes - assessment of dehydration pregnancy test serum amylase - if pancreatitis suspected abdominal radiology - helpful to distinguish: volvulus intussusception renal stones (90%) gallstones (10%) localised ileus Generally, urine analysis is unhelpful in differentiating appendicitis from a urinary tract infection. There is no place for barium enema in the diagnosis of appendicitis. Occasionally, ultrasound and CT scanning are used to investigate suspected appendicitis where the story is atypical. US exclude gynae pathology (ovarian cyst)
 gallstones (10%) localised ileus. Generally, urine analysis is unhelpful in differentiating appendicitis from a urinary tract infection. There is no place for barium enema in the diagnosis of appendicitis. Occasionally, ultrasound and CT scanning are used to investigate suspected appendicitis where the story is atypical. US exclude gynae pathology (ovarian cyst)")
333
Diff diagnosis of acute appendicitis
Ectopic pregnancy Salpingitis Period pains Cystitis Cholecystitis Diverticulitis Perforated ulcer Meckel’s diverticulum Crohn’s disease

334
What is this a sign of?

335
Duodenal atresia investigated by:
electrolyte and acid-base status measures, e.g. U&E's, blood gases, with subsequent correction of abnormalities plain abdominal X-ray: this may show a 'double bubble' sign of duodenal obstruction barium study may show stenosis Treatment involves surgical correction via a duodenojejunostomy with resection of the atretic section.

336
A 34 year old vagrant is treated following a second variceal bleed… what is shown here?

337
TIPS TRANSJUGULAR INTRAHEPATIC PORTO-SYSTEMIC SHUNT
the treatment of acute oesophageal variceal bleeds which fail to respond to drugs or sclerotherapy the prevention of variceal bleeds angioplasty balloons and metallic stents are used to enlarge and maintain the porto-systemic shunt

338
What is wrong with this chap. How would you investigate
What is wrong with this chap? How would you investigate? What are common causes?

339
ASCITES NOTE DRAIN SITES!!! Shifting dullness ultrasound
diagnostic paracentesis in which 30 to 50 ml of fluid is withdrawn. This will enable identification of: protein content: albumin and total protein malignant cells bacteria white blood cells Glucose TB culture amylase

340
CAUSES OF ASCITES TRANSUDATE EXUDATE Protein<3g/100ml
Cardiac failure Constrictive pericarditis Nephrotic syndrome Cirrhosis Ovarian tumours –meig’s syndrome EXUDATE Protein>3g/100ml Malignancy Pyogenic Infection Tb Pancreatitis Lymphoma Myxoedmea

341
MANAGEMENT OF ASCITES TENSE ASCITES NON-TENSE ASCITES
therapeutic paracentesis of 4-6 litres plasma volume expansion with albumin (6g/litre of ascitic fluid removed) NON-TENSE ASCITES bed-rest, reduced salt intake, and spironolactone ( mg per day). A fall in weight of approximately 0.5 kg per day should be aimed for. spironolactone is gradually increased to 300 mg per day and then, if necessary, frusemide is added, but only once the spironolactone has reached its maximum dose. loop diuretics may precipitate the hepatorenal syndrome If a patient has malignant ascites then large doses of frusemide may be required to control ascites. A Le Veen shunt (peritoneo-venous) may be useful in refractory cases.
 NON-TENSE ASCITES. bed-rest, reduced salt intake, and spironolactone ( mg per day). A fall in weight of approximately 0.5 kg per day should be aimed for. spironolactone is gradually increased to 300 mg per day and then, if necessary, frusemide is added, but only once the spironolactone has reached its maximum dose. loop diuretics may precipitate the hepatorenal syndrome. If a patient has malignant ascites then large doses of frusemide may be required to control ascites. A Le Veen shunt (peritoneo-venous) may be useful in refractory cases.")
342
What is wrong with this baby?
How would you treat?

343
kwashiokor Classically hair colour change, hepatomegaly, pitting oedema, bleating cry when picked up Tx electrolyte imbalance, hypoglycaemia, vitamin deficiency. May need warming if hypothermic. 80-100kcal/kg/day – care not to overload pt

344
What is wrong with this baby?

345
Marasmus Marasmus is failure to grow associated with emaciation and fair appetite. It may be defined in terms of weight, for example less than 60% of that expected for age. Marasmus generally occurs in infants up to one year. In the developed world it is found in infants who are born undernourished or are recovering from a severe chronic illness, especially those affecting the bowel. In developing countries this condition commonly is associated with failure of lactation due to poor nutrition of the mother. Note that marasmus is an adaptive response to poor nutrition.

346
A 77 year old man presents with his 4th episode of rectal bleeding
A 77 year old man presents with his 4th episode of rectal bleeding. The blood is a mixture of fresh blood and clots. The bleeding was severe enough to require a 4 unit blood transfusion. Barium enema was normal. Colonscopy showed this lesion

347
Angiodysplasia Colonic angiodysplasia is a common cause of acute or chronic rectal bleeding and iron deficiency anaemia. Angiodysplasias are tiny mm in diameter - hamartomatous capillary lesions in the colonic wall which produce bleeding out of proportion to their size. They are believed to be acquired, possibly as a result of tension on the veins where they pass through the muscularis. colonscopy: may visualise lesion Treatment: electrical coagulation via the colonoscope resection of segment of colon if the above is unsuccessful

348
This baby presented with severe diarrhoea, alopecia, FTT and a rash over the mucocutaneous junction. This started soon after he stopped breastfeeding.

349
acrodermatitis enteropathica
autosomal recessive disorder characterized by periorificial and acral dermatitis, alopecia, and diarrhoea Sharply demarcated, brightly erythematous periorificial plaque Caused by Zinc deficiency Tx zinc

350
This boy presented with this rash, diarrhoea and confusion
What is wrong?

351
Pellagra caused by deficiency of niacin
classically characterised by four D's: photosensitive dermatitis diarrhoea dementia Death monotonous maize diet (maize is low in tryptophan) a very low protein diet conditions producing considerable loss of protein e.g. nephrotic syndrome
 a very low protein diet. conditions producing considerable loss of protein e.g. nephrotic syndrome.")
352
What is wrong with this man with wrist drop and marked wasting of the lower extremities?

353
Beriberi severe prolonged deficiency of vitamin B1 (thiamine)
Beriberi was discovered in the seventeenth century in Java by the Dutch physician Jacobius Bonitus. The name means "sheep" in the local language; this describes the characteristic gait of patients. Today, beriberi is confined to the poorest parts of Asia where little else is eaten except polished rice. Prevention of beriberi requires: a more varied diet, including legumes and pulses thiamine supplementation of rice

355
Scoliosis Image in a 27-year-old tennis player with a history of cystic fibrosis and only minimal symptoms exhibits bronchial wall thickening, bilateral small nodular opacities, and scoliosis.

357
bronchiectasis

359
Barrel chest Emphysema Sorry I think that man might actually be dead

360
What is this? What is it showing?

361
Flow volume loop Showing severe airflow limitation
This is a normal one

363
Hyperinflated lung COPD

364
Report this xray of a 47-year-old smoker who presented after just a few hours of rigors and productive cough. What other investigations would you carry out and how would you manage?

365
consolidation in the right upper lobe
Consistant with a pneumonia Investigate: FBC (WCC raised, particularly neutrophils) U+Es Sputum and blood culture Pulse oximetry and ABG Serology for atypicals RBS – diabetes is risk factor for infection
 U+Es. Sputum and blood culture. Pulse oximetry and ABG. Serology for atypicals. RBS – diabetes is risk factor for infection.")
366
Assessing severity CURB-65 Score Confusion Urea>7mmol/l
Resp rate>30 BP systolic<90 or diastolic<60 Age>65 Score 0-1 home Tx 2 consider hospital supervised Tx (in or outpt) 3 or more in patinet Tx and assess for ICU
 3 or more in patinet Tx and assess for ICU.")
367
MANAGEMENT

368
What is this ECG of a 23 year old man with episodes of tachycardia showing? How would you manage?

369
Wolf Parkinson White The two complications of WPW are the development of an AV re-entrant tachycardia or atrial fibrillation. An AV re-entrant tachycardia is managed as for any other supraventricular tachycardia (see linked item) Atrial fibrillation secondary to WPW should not be treated with AV-blocking drugs such as verapamil and digoxin. The simplest method of terminating atrial fibrillation is cardioversion. If drugs are to be used then they must slow conduction in the accessory pathway e.g. intravenous sotalol, flecainide, amiodarone. These drugs will slow the ventricular response and will often result in restoration of sinus rhythm. For prevention of atrial fibrillation drugs such as oral sotalol and amiodarone are effective.
 Atrial fibrillation secondary to WPW should not be treated with AV-blocking drugs such as verapamil and digoxin. The simplest method of terminating atrial fibrillation is cardioversion. If drugs are to be used then they must slow conduction in the accessory pathway e.g. intravenous sotalol, flecainide, amiodarone. These drugs will slow the ventricular response and will often result in restoration of sinus rhythm. For prevention of atrial fibrillation drugs such as oral sotalol and amiodarone are effective.")
370
What has happened to him?
This 69 year old man was admitted to hospital 5 years earlier with palpitations and blackouts. He was discharged on a new medication. What has happened to him? What other problems are associated?

371
Amiodarone side effects
The side-effects are time and dose related. Minor side effects of amiodarone include corneal microdeposits. Moderate side effects include: photosensitivity skin discolouration abnormal thyroid function, and abnormal TFTs nausea nightmares sleep disturbance Serious side effects include: peripheral neuropathy disturbed hepatic function: acute hepatitis and jaundice are particularly associated with intravenous administration chronic toxicity may cause fibrosis or cirrhosis amiodarone lung amiodarone has some proarrhythmic potential

372
This is the ECG of a 70yr old man with exercise intolerance
This is the ECG of a 70yr old man with exercise intolerance. What is shown…how would you manage?

373
Complete heart block Acute inferior block:
give atropine to reduce vagal effect temporary pacing required for profound bradycardia Acute anterior block: start temporary pacing early may need a permanent pacemaker Chronic block: permanent pacing

374
An 57 year old lady with palpitations.

375
Atrial flutter with 2:1 AV conduction
The sawtooth waveform of atrial flutter can usually be seen in the inferior leads II, III and aVF if one looks closely. Sometimes the rapid atrial rate can be seen in V1. Suspect atrial flutter with 2:1 block when you see a rate of about 150 bpm.

376
68 year old lady on digoxin complaining of lethargy.

377
What is wrong? What is your immediate management?

378
Management of VF Give 1 shock at 360
IMMEDIATELY RESUME CPR 30:2 FOR 2 MINS ASSESS RHYTHM

381
Restrictive lung disease
Restrictive lung disease. Chest radiograph of a 67-year-old man diagnosed with idiopathic pulmonary fibrosis, based on open lung biopsy findings. Extensive bilateral reticulonodular opacities are seen in both lower lobes.

383
Restrictive lung disease
Restrictive lung disease. A CT scan image from a 59-year-old woman shows advanced pulmonary fibrosis. Extensive honeycombing and traction bronchiectasis are present.

385
Chest radiograph in a 60-year-old dairy farmer who had an 8-year history of intermittent dyspnea shows bilateral reticulonodular interstitial infiltration secondary to subacute hypersensitivity pneumonitis

387
Bilateral hilar lymphadenopathy
DIFF DIAGNOSIS Sarcoidosis (commonest cause in UK) tuberculosis lymphoma - almost never shows the striking symmetry of the BHL carcinoma fungi hypogammaglobulinaemia berrylliosis
 tuberculosis. lymphoma - almost never shows the striking symmetry of the BHL. carcinoma. fungi. hypogammaglobulinaemia. berrylliosis.")
389
This 55yr old pipe lagger developed left sided chest pain, finger clubbing and weight loss

391
Lid lag Graves disease

393
Pretibial myxoedema Graves disease

395
bronchiectasis

397
Pseudohypoparathyroidism
End organ resistance to PTH Small metacarpals Pseudopseudohypoparatyhroidism – is when have physical abnormality but no end organ resistance to PTH

398
What are the indications for this?
What are the complicatons? Where is the semi permeable membrane? Where is the dialysate?

399
Dialysis Acute renal failure End stage (established) renal failure
Persistent hyperkalaemia Severe metabolic acidosis Pulmonary oedema Encephalopathy or pericarditis (20 to uraemia) End stage (established) renal failure eGFR<15ml/min
 End stage (established) renal failure. eGFR<15ml/min.")
400
Complications or RRT Hypotension/ hypertension Anaphylaxis
hyperkalaemia - from poor dietary compliance amyloidosis – infection - Gram positive bacteria are common. There is an increased incidence of hepatitis C malnutrition - causes include: loss of amino acids and peptides in the dialysate sodium restriction and poor palatability of diet dialysis induced hypercatabolism social and psychological factors aluminium intoxication - from inadequate filtration of incoming water supply - this is now rare Vascular access- thrombosis, stenosis, bleeding, ischaemia Anaemia Renal osteodystrophy

401
What is this? What would it feel like? What could have caused this (rarely)
")
402
Varicocoele Feels like a bag of worms Dull dragging ache at end of day
Commoner on left side Rarely renal carcinoma can compress L testicular vein and cause a L sided varicocoele

404
SAH Subarachnoid haemorrhage accounts for about 6% of cerebrovascular disease with an annual incidence of about 1 per 10,000. It is bleeding from intracranial vessels in the subarachnoid space. Occasionally, the arachnoid layer gives way and a subdural haematoma develops. Seen here as white area in the centre

406
syringomyelia Cavitation of central segment of spinal cord
DISSOCIATED SENSORY LOSS (spinothalamic damage- lose pain and temp but retain light touch, proprioception and vibration) WEAKNESS, WASTING, LOSS OF REFLEXES (anterior horn cell damage) Consider surgery for tx
 WEAKNESS, WASTING, LOSS OF REFLEXES (anterior horn cell damage) Consider surgery for tx.")
408
Bulbar Palsy LMN lesion

409
Apparently showing same thing
In a homosexual man with weight loss and recurrent infections

410
CMV retinitis Cytomegalovirus (CMV) retinitis occurs in immunocompromised patients. 'pizza pie' fundus: retinal spots which are the result of superficial retinal infarction also flame shaped haemorrhages associated with a low CD4 count Asymptomatic or sudden (and untreatable) visual loss Other manifestations of cytomegalovirus infection in these patients includes encephalitis, pneumonitis, and diffuse gastro-intestinal involvement. Treat with ganciclovir (or foscarnet in cases of reduced sensitivity to ganciclovir).
 visual loss. Other manifestations of cytomegalovirus infection in these patients includes encephalitis, pneumonitis, and diffuse gastro-intestinal involvement. Treat with ganciclovir (or foscarnet in cases of reduced sensitivity to ganciclovir).")
412
Roth spots These are superficial retinal haemorrhages with red edges but pale or white centres. These may be seen in a variety of conditions including infective endocarditis. They are not pathognomonic of any particular disease. Also seen in leukaemia

414
Loosers zones Osteomalacia
This is a pseudofracture seen in osteomalacia. On x-ray, it appears as a thin, translucent band, about 2 mm in width, which runs perpendicular to the surface of the bone extending from the cortex inwards. incomplete stress fractures which heal with callus lacking in calcium pubic rami, the necks of the humeri and femora and at the axillary edge of the scapulae

416
Oral kaposi’s sarcoma

418
Wickham’s striae Lichen planus The oral lesions have a radiating velvet, white or gray appearance, most commonly in a reticulated pattern. This represents the "lace-like" network of linear subepithelial fibrosis found in these lesions. The buccal and glossal mucosas are most commonly affected, however, lesions can also be found in the palate and gingiva (erosive gingivitis).
.")
420
Central retinal artery occlusion
The retina has become milky because of infarction. Tissue necrosis makes the tissue lose its normal transparency. Cherry-red spot The red-orange color of the fovea appears in stark contrast to the surrounding milky retinal edema. Called a "cherry-red spot," it results from the fact that the fovea contains only the photoreceptor layer, which is spared because it is nourished by the choroidal circulation rather than the retinal circulation.

422
Central retinal vein occlusion
The patient presents with painless loss of vision, often mixed with sparkles, that may be sudden or evolve over hours to days. Systemic hypertension is the most common cause; hyperviscous and hypercoagulable states must also be considered. Numerous haemorrhages seen – splattered with blood

424
thalassaemia

425
What is shown on left? What else is needed for the diagnosis of this condition?

426
Serum electrophoresis
Monoclonal IgG kappa monoclonal band Multiple myeloma Control sample ran on left Increased plasma cells on bone marrow biopsy CRAB

Similar presentations


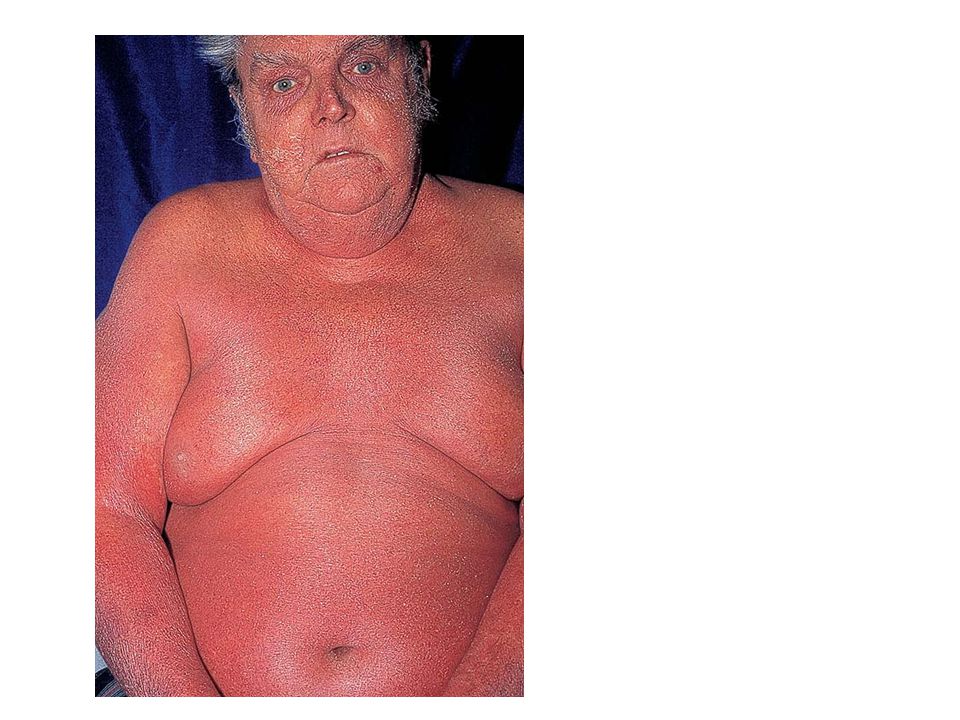

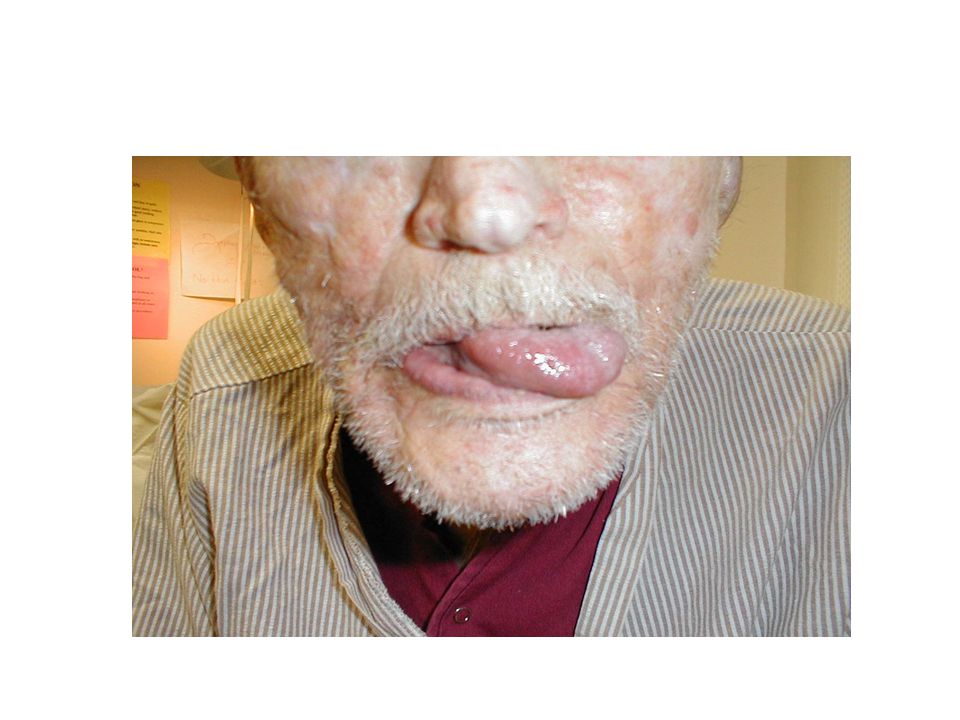

































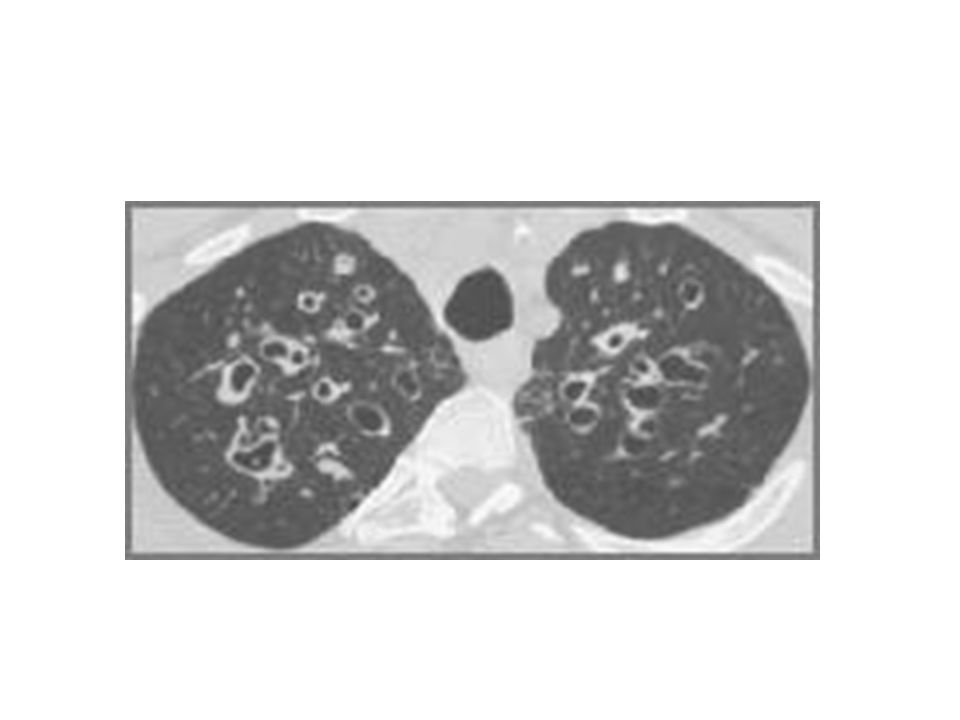






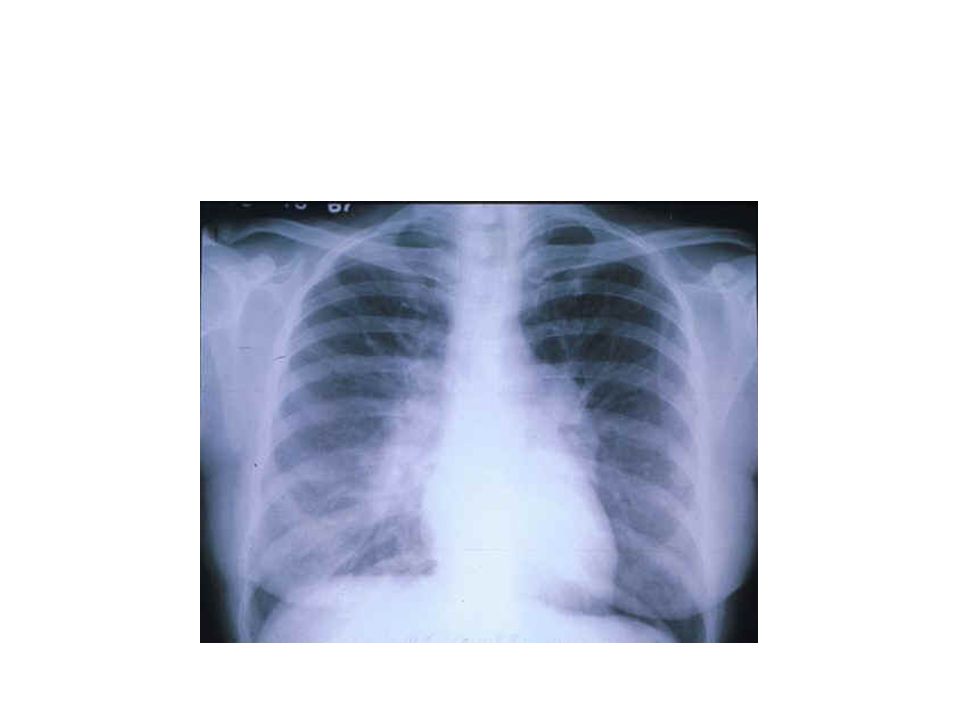
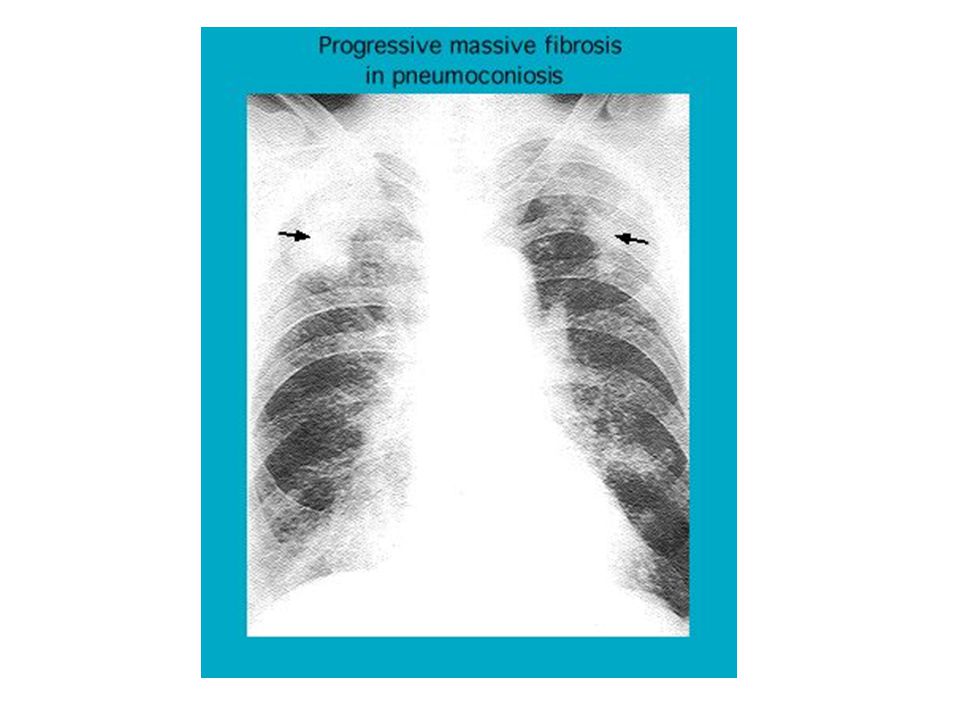


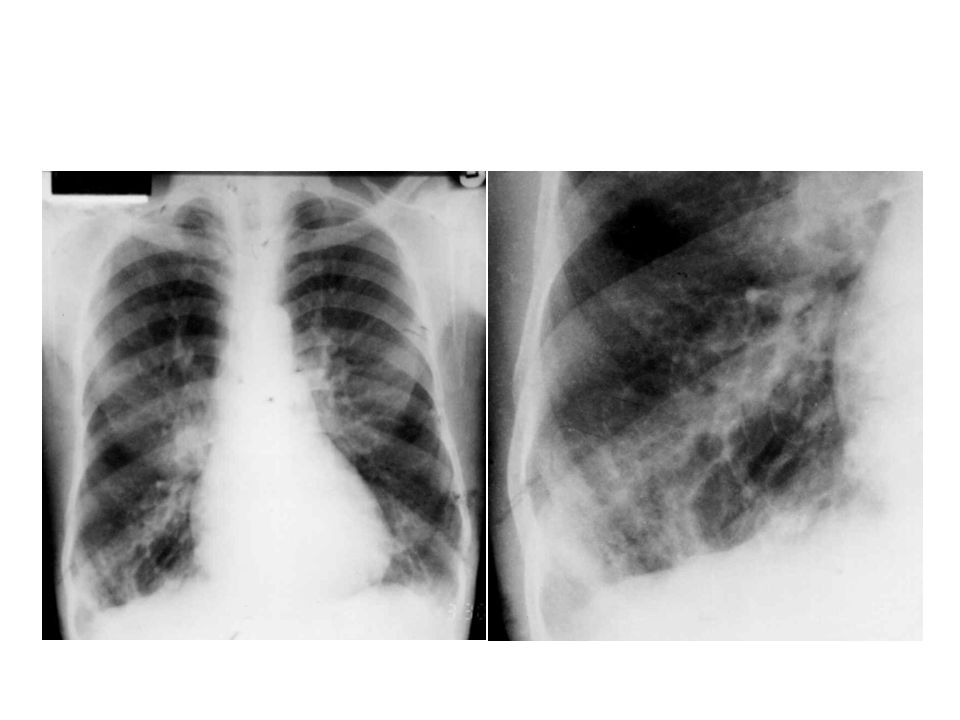






















 Definition: Rheumatic fever (RF) is an autoimmune disease affecting the heart and extra- cardiac.>")







 Ulcerative colitis is an inflammatory bowel disease (IBD) that causes chronic inflammation of the digestive tract It is.>")