Download presentation
Presentation is loading. Please wait.

1
MDT Lumbar Assessment Overview PMR Resident/Student Session Richard Rosedale PT Dip MDT

2
AA AA DTO

3
Lumbar Spine How do you treat? How do you classify? “T” “D”

4
Patho-anatomical “Facet” What’s your Rx? Derangement What’s your Rx?

5
Facet A D T ? ?

6
Refs… Laslett 2006 Laslett 2004 Dreyfuss 2003 Young 2003 Revel 1998 Dreyer 1996 Schwarzer 1994 Jackson 1988 etc

7
Big picture look at “evidence”. What is the best treatment for chest pain? What is the best study design to answer this question?

8
Chest Pain Outcome Measures Are the small benefits worth the additional costs? 20% Improved25% Improved NothingAnti-acidsNTG 80% Improved10% Improved 80% Improved10% Improved T O Cardiac Pain A D Esoph’l Pain Black Box RCT

9
“Symptoms” are poor candidate for RCTs Chest pain Abdominal pain Low back pain Leg pain “sciatica” Non-Specific LBP Black Box Model

10
Non-Specific LBP Black Box Model Black Box RCTs Non-specific results Our recent research reality…. No intervention is any better than “doing nothing”. Out- comes Treatment

11
Spratt (02): RCTs of non-specific LBP “are doomed”. By persisting with studies of non-specific LBP, “the results of RCTs will continue to be frustrating, meaningless, and even misleading.” Bouter, van Tulder, Koes (Spine 98): “There is urgent need for good ideas about how to identify homogeneous subgroups.” “The efficacy of interventions in the subgroups should be studied in RCTs.” Likewise our guidelines!!
: There is urgent need for good ideas about how to identify homogeneous subgroups. The efficacy of interventions in the subgroups should be studied in RCTs. Likewise our guidelines!!.")
12
Understanding the science behind the “evidence”. 25 years & approx 1,000 RCTs (black box) Systematic reviews – (dozens) International “evidence” based-guidelines What do we have?
 Systematic reviews – (dozens) International evidence based-guidelines What do we have .")
13
Not much. Screen for red flags Advice to remain active Reassurance Review psychosocial yellow flags Generic – “one size fits all” guidelines Is this the best we can do?

14
The best treatment for LBP? We have been asking the wrong questions! Testing questions in the wrong order!

15
Out- comes Treatment Assessment Diagnosis “The single most important thing: establishing the validity of any one link requires that all previous links have been established.” “Statistical Relevance” K. Spratt, Ph.D. Book: Orthopaedic Knowledge Update Spine ‘02, AAOS, p497-505 The ADTO Model

16
Out- comes Treatment Assessment Diagnosis RCTs of subgroups Reliability studies: test findings/results subgroup classification Prospective subgroup studies: outcome prediction, with or w/o treatment(s). Start by building the FOUNDATION:

17
How does MDT measure up? Treatment Outcomes Assessment Diagnosis

18
Reliability studies MDT Dionne ’06 Fritz 00, 06 Laslett 05, 03 Wilson 99 Clare 05, 04, 03 Donahue 96 Petersen 04, 03 Bruijne 03 Kilpikoski 02Riddle 94 Werneke 04, 03, 01 Spratt 93 Ramzjou 00Kilby 90 May 06 systematic review Assessment Diagnosis 14 + pain response studies

19
Prospective subgroup studies: (observational, case series, prognostic) George 05, Skytte 05, Werneke 05, 01, 99 Sufka 98, Donelson 97, 90 Karas 97, Kopp 86 Long 95, Erhard 94, Alexander 92 Aina 04 review Treatment Diagnosis 10+ centralization studies
 George 05, Skytte 05, Werneke 05, 01, 99 Sufka 98, Donelson 97, 90 Karas 97, Kopp 86 Long 95, Erhard 94, Alexander 92 Aina 04 review Treatment Diagnosis 10+ centralization studies")
20
RCT’s with subgroups:MDT Brennan 06 (Rasmussen 05) Delitto 93, Fritz 03, Larsen 02, Long 04, Schenk 03, Williams 91, Clare 04, Cook 05 Reviews Out- comes Treatment 7 studies
 Delitto 93, Fritz 03, Larsen 02, Long 04, Schenk 03, Williams 91, Clare 04, Cook 05 Reviews Out- comes Treatment 7 studies")
21
An example of how classification effects outcome

22
Long et al 2004 312 LBP patients – MDT assessment 230 (74%) had directional preference (DP) Randomised to: 1. Matched exercise 2. Opposite exercise 3. Evidence-based – active / fear reduction

23
Mechanical Assessment Directional Preference Extension Flexion Lateral Mechanical Assessment Directional PreferenceNo Directional Preference Random- ization Opposite MatchedEBG Directional Treatments Excluded Study Design

24
Outcomes 2 weeks – self-rated improvement (Long et al 2004) 0% 20% 40% 60% 80% 100% MatchedOppositeControl Worse No Change Better Resolved 95% 23% 42% p<.001
 0% 20% 40% 60% 80% 100% MatchedOppositeControl Worse No Change Better Resolved 95% 23% 42% p<.001")
25
Beck Depression Inventory p <.009 2 2.2 2.4 2.6 2.8 3 3.2 3.4 3.6 3.8 4 12 MatchedEBGOpposite Interference With Activity p <.001 Results:

26
Roland-Morris DQ 11 12 13 14 15 16 17 18 19 12 MatchedEBGOpposite Pills per Day for LBP 56% taking meds P =.016P =.009

27
Results: P <.001P =.003

28
If classification was the key…what would you need? Reliable assessment System to classify Valid classifications What about treatment?

29
Natural history of LBP Persistence is common - symptoms for several months Linton et al 1998 43% Hillman et al 1996 47% Waxman et al 2000 42% Szpalski et al 1995 36%

30
Natural history of LBP Relapse is common - more than one episode in a year Linton et al 1998 57% Brown et al 1998 55% Heliovaara et al 1989 45% Toroptsova et al 1995 65% Klenerman et al 1995 72%

31
What are the treatment implications of the epidemiological evidence?

32
Self Treatment How do we know the patient can treat themselves? Assessment based around patient generated forces

33
Patient generated forces assessment How do you do that?

34
Assessment Practical

35
How many LBP patients can be assessed and treated using self generated forces?

36
Hefford 2008 Cervical Thoracic Lumbar 81% Derangements 87% Derangements 75% Derangements

37
Directional Preference Mechanical loading examination including RMs Identification of specific directional exercise Symptoms centralize or decrease or range increases Confirms classification of Derangement

38
MDT Centralization

39
Contrast with other treatment approaches Repeated movements for assessment and management Emphasis on patient independence Avoidance of therapist dependency Use of minimal intervention Exercise and therapist intervention Exercises used for pain relief

45
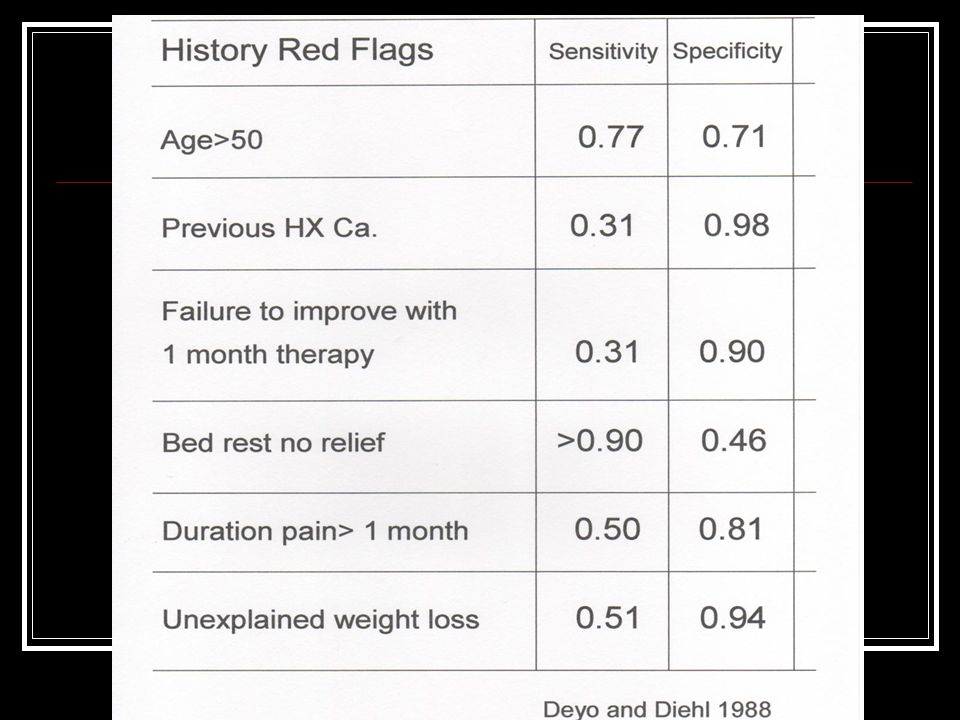
Red flag clues Age > 55 History of cancer Unexplained weight loss Constant, progressive, non-mechanical pain, worse at rest Systemically unwell Persisting severe restriction of lumbar flexion

46
Red flag clues Systemic steroids History of IV drug use History of significant trauma History of trivial trauma and severe pain in osteoporotic individual No movement or position centralises, decreases, or abolishes pain

47
Cancer “ A previous history of cancer has such high specificity (0.98) that such patients should be considered to have cancer until proven otherwise” Deyo 1992
 that such patients should be considered to have cancer until proven otherwise Deyo 1992")
49
If Age > 50 OR History of cancer OR Unexplained weight loss OR Failure to improve with conservative therapy THEN… sensitivity = 1.00

50
Aims of the Physical Examination Usual posture Symptomatic response to posture correction Any obvious deformities or asymmetries Baseline measures of mechanical presentation Neurological examination Symptomatic and mechanical response to repeated movements

51
Conclusion Syndrome classification Appropriate therapeutic loading strategy Appropriate testing loading strategy

52
Physical Examination Sitting posture and its effect of pain Posture correction Better Worse No Effect Standing posture

53
Physical Exam Lordosis Lateral shift

54
Movement loss: What are we looking for here? Range of movement Pain or stiffness that stops the movement Movement pathway deviation Confidence and willingness to move Curve reversal

55
Repeated movements Flexion in standing Extension in standing Flexion in lying Extension in lying Side gliding (as required)
")
56
BASELINES Symptomatic Mechanical

57
Other Tests SIJ Hip Be aware of false positives

58
Provisional Classification Derangement Dysfunction Posture Other……

59
Summary What is MDT? (McKenzie Method ® ) Diagnostic – Reliability Prognostic – Validity Therapeutic – Dx/Rx link Client centered – Patient empowerment Prophylactic – Prevent recurrences
 Diagnostic – Reliability Prognostic – Validity Therapeutic – Dx/Rx link Client centered – Patient empowerment Prophylactic – Prevent recurrences.")
Similar presentations









 Symposium 13 th May 2004 Carol Coole Occupational Therapist NOTTINGHAM BACK TEAM.>")













