Download presentation
Presentation is loading. Please wait.

1
Mobile Radiography Course Instructor: TAGELDIN ABUGROON 1304 RAD 1304

2
Work with Mobile Equipment in the Ward

3
General Concerns Examinations are normally complicated by a variety of situations, which include: The patient’s medical condition, degree of Consciousness & cooperation. The patient’ s treatment restrictions: (1). life support system. (2). Drips (I.V. line). (3). Chest or abdominal drains. (4). ECG leads location. (5). Traction apparatus. Physical restrictions: 1.Room size and layout. 2.Equipment size and shape. 3. Access to adequate power supply.
. life support system. (2). Drips (I.V. line). (3). Chest or abdominal drains. (4). ECG leads location. (5). Traction apparatus. Physical restrictions: 1.Room size and layout. 2.Equipment size and shape. 3. Access to adequate power supply..")
4
ECG Monitoring Electrode placement for ECG monitoring

5
Chest Radiograph with ECG electrode artifact.

6
Pulse Oximeter Pulse Oximeter Probe on finger

7
Neonatal Intensive Care Unit

9
Intensive Care Unit

10
(B) Special concerns: 1.Fully understanding of the received request, so that the exact nature of the x-ray examination & the reason for it are both understand. 2. Correct equipment & cassettes (cassette size, speed & Number) are obtained, to avoid unnecessary delay & disturbance. 3. With serious illness patient the radiographer should ask for in-charge nurse or medical staff help, to avoid unintentional patient’s injury or mistakes.
 are obtained, to avoid unnecessary delay & disturbance. 3. With serious illness patient the radiographer should ask for in-charge nurse or medical staff help, to avoid unintentional patient’s injury or mistakes..")
11
Standard Procedure for success Result: (1) When the technologist arrived to the patient ward he should first report to the nurse in-charge, this is not only courtesy to the person in charge but will enable the technologist to find out in which part of the ward is the patient to be x-rayed & examination to be done. This also enable the technologist to explain the procedure to the nurse & receive any special patient’s concerning information, which will help the technologist to assess any further help.

12
(2) It is kindness for technologist to go in to see the patient without the equipment & with smiling approach, to give the patient of what is to be the examination of what is to be undertaken. This few minutes has great effect on removing the patient’s fear & achieving full cooperation, this is also will enable the technologist to assess the patient’s capability for cooperation & any physical difficulties presence. (3)Now the technologist should place the equipment in an appropriate place, then the cassette should be placed with help & care. The tube should be positioned & a radiograph is taken. (4)The radiographer should preserve the patient’s privacy by pulling around the bed curtains.
Now the technologist should place the equipment in an appropriate place, then the cassette should be placed with help & care. The tube should be positioned & a radiograph is taken. (4)The radiographer should preserve the patient’s privacy by pulling around the bed curtains..")
13
(5) After the radiographer has finished, the patient should return back to his position & made him as comfortable as possible. (6) The equipment should be put away with tube column & tube head locked in a position, which prevent any dangers before it is taken from the ward. (7) We should separate the exposed film from unexposed one. (8) Most of the requests coming from the ward or ICU to the radiology department requesting a plain film of the chest for adult or baby.
 The equipment should be put away with tube column & tube head locked in a position, which prevent any dangers before it is taken from the ward. (7) We should separate the exposed film from unexposed one. (8) Most of the requests coming from the ward or ICU to the radiology department requesting a plain film of the chest for adult or baby..")
14
Patient special conditions and solution: Patient with Oxygen therapy. Patient with Intravenous infusion. Patient with Tracheostomy. Patient with Nasogastric tube. Patient with Drainage system. Patient with Traction.

15
Patient with Oxygen therapy The oxygen is supplied from cylinder or through a piped supply to the patient’s bedside. It is administered to patient in one of three ways: 1.By enclosing him in an oxygen tent. 2. By oxygen mask fitting over his mouth and nose.. 3. By tubes inserted up his nasal passage.

16
Oxygen Mask

17
Nasal Cannula for Oxygen administration

18
There are two important points to remember when doing radiography on patients who are having oxygen: 1. The risk of fire and explosion. So in order to avoid this risk the oxygen supply should be switched off. 2. In case of very ill patient who is oxygen dependent, the patient and positions should be ready before the oxygen supply cut off, so that this is done for the shortest possible time and avoid any harm to the patient. These should be done under the nurse supervision.

19
Oxygen flowmeter at wall outlet

20
Patient with Intravenous Infusion In some cases as part of the patient’s treatment it may be necessary to give him fluid or blood by a method other than oral administration. This is may be because of disability of the patient take any thing through his mouth or due to severe fluid loss. The radiological technologist has no responsibility for altering or sitting the rate of flow of an intravenous infusion set.

21
IV Fluids are packaged in bottles & in plastic bags

22
IV Infusion Set up Remove protective cover from access port. Avoid contamination With tube clamped off, insert drip Chamber firmly Into access port.

23
Invert bag or bottle & suspend from pole Setup is ready for attachment

24
IV Flow Control Practice improves Precise regulation of drip rate

25
IV pumps regulate infusions & permit self administration of IV medications

26
Veins used for venipuncture. A. Veins of anterior aspect of forearm. B. Superficial veins of dorsal aspect of hand

27
While the technologist dealing with the patient who has intravenous infusion, he should observe the following points: 1. If the needle become dislodge from its site in the vein & a swelling occur around the needle site this can indicate the needle is in the tissue then the in-charge nurse must be reported immediately. 2. If the infusion stops because of tubing kinked the radiological technologist should straight the tubing then call the in-charge nurse. 3. If the infusion stops then make sure that bandages &clothing on the limb are not tight, then call the in-charge nurse.

28
4. If the infusion stops because of the needle maybe against the vein wall, so the radiological technologist should straightening the limb then call the in-charge nurse. 5. If the infusion stops because of the head of the pressure is too low then the radiographer should raise the bottle, then call the in-charge nurse. 6. If the infusion stops because of blockage in the tube by a clot, this should be aspirated by a medical officer using sterile syringe.

29
During the x-ray equipment movement, the technologist must notice the position of the infusion stand & avoid any strike. This stand can be moved about a little if care is taken to see that no strain is put on tubing, but the bottle should not be lowered from it’s position. If the bottle is seen to be nearly empty the attention of the ward should be drawn to this fact.

30
Patient with Tracheostomy What is Tracheostomy? A tracheostomy is a surgical opening in the upper trachea and a tube is passed, keeping the patient’s airway open and having an easy access to the patient trachea to bypass his nose, mouth and pharynx. Tracheostomy is indicated for 1.To overcome any obstruction in the upper airway route (e.g. mouth obstruction). 2. To allow secretions to be removed from the trachea and bronchi easily by suction tube (in patient who can’t cough effectively). 3. To improve effective ventilation of the lung.
. 2. To allow secretions to be removed from the trachea and bronchi easily by suction tube (in patient who can’t cough effectively). 3. To improve effective ventilation of the lung..")
31
Tracheostomy OpenAttached to respirator

32
4.To prevent the inhalation of the food, fluid and secretions by a patient whom has paralysis of the muscles involved in swallowing (by separating the larynx and the pharynx). 5. In unconscious, paralyzed and traumatic injury patient. These patients can’t speak, so communication skills technique should be concerned with this kind of patient (pencil and a writing pad should be provided). These patients need regular suction of the accumulate lungs secretions by the nurse in charge. The patient should be positioned in semi-erect of his back, to avoid any uncomfortable position. The radiological technologist should avoid any obstruction of the tube airway.
. These patients need regular suction of the accumulate lungs secretions by the nurse in charge. The patient should be positioned in semi-erect of his back, to avoid any uncomfortable position. The radiological technologist should avoid any obstruction of the tube airway..")
33
Patient with Nasogastric tube What is Nasogastric Tube? It is a tube passed through the nose and reaches the stomach. What is the purpose of Nasogastric tube? This tube used for patient’s feeding. The radiological technologist should avoid any dislodge or tension on the tube.

34
Nasogastric Tube Placement

37
Nasogastric Tube in small bowel. Note that iodine Contrast Media has been injected through tube to outline intestine.

38
AP Abdomen radiograph demonstrates Nasogastric Tube feeding tube in the stomach (arrow)
")
39
Patient with Drainage system What is drainage system? It is a length of plastic tubing inserted into whichever cavity it is required to drain and has a plastic bag at the end to measure the draining fluid (e.g. urine drainage system). The radiological technologist should avoid striking it or compressing or kinking the tube during moving the X-ray equipment or during the movement of the patient.
. The radiological technologist should avoid striking it or compressing or kinking the tube during moving the X-ray equipment or during the movement of the patient..")
40
Chest Tube placed to drain fluid from pleural space

41
Disposable Commercial Drainage System

42
Measuring Urinary Output

43
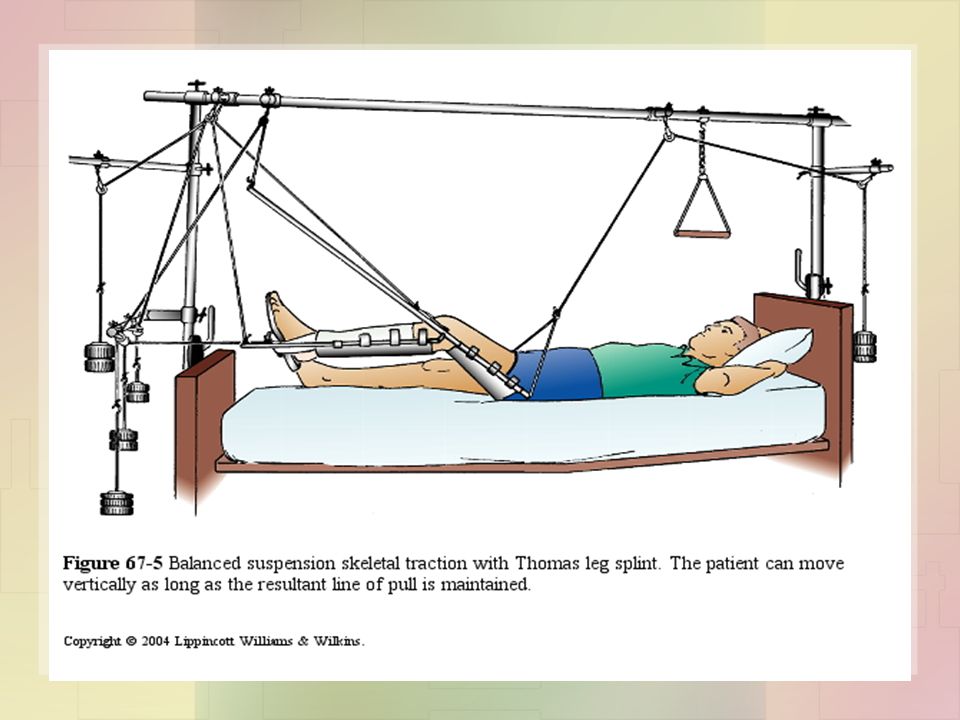
Patient with Traction What is the purpose of traction? It is used usually for fracture treatment (e.g. correct overriding bone fragment). This can be achieved by applying weight. The radiological technologist should avoid any releasing weight. He/She should be aware of the X-ray equipment position. The radiological technologist should avoid any movement of the effected limb.
. This can be achieved by applying weight. The radiological technologist should avoid any releasing weight. He/She should be aware of the X-ray equipment position. The radiological technologist should avoid any movement of the effected limb..")
Similar presentations






>")



 SUCTION.>")









 Infusion>")

