Download presentation
Presentation is loading. Please wait.

1
MENISCI

3
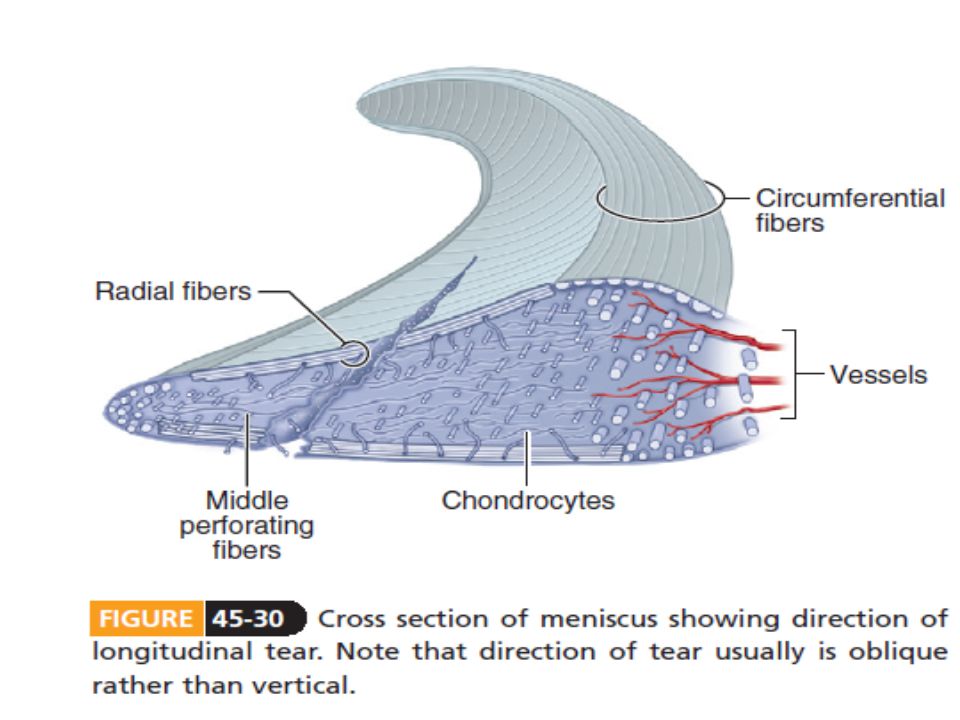
histology Water( 75%)Collagen type 1Proteoglycans elastin
Collagen type 1Proteoglycans elastin")
4
Collagen fibers Circumferential fibers(majority ) Radial fibers Perforating fibers
 Radial fibers Perforating fibers")
5
Role of hoop tension in menisci. Hoop tension developed in menisci acts to keep them between bones

6
Radial tear eliminates hoop tension and damages meniscus function

7
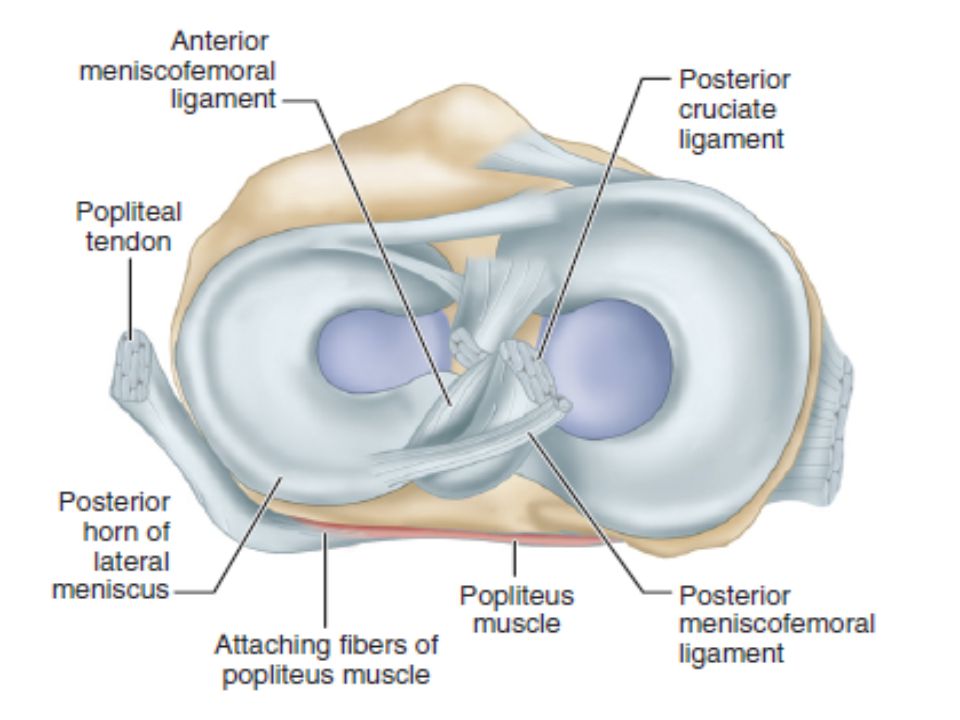
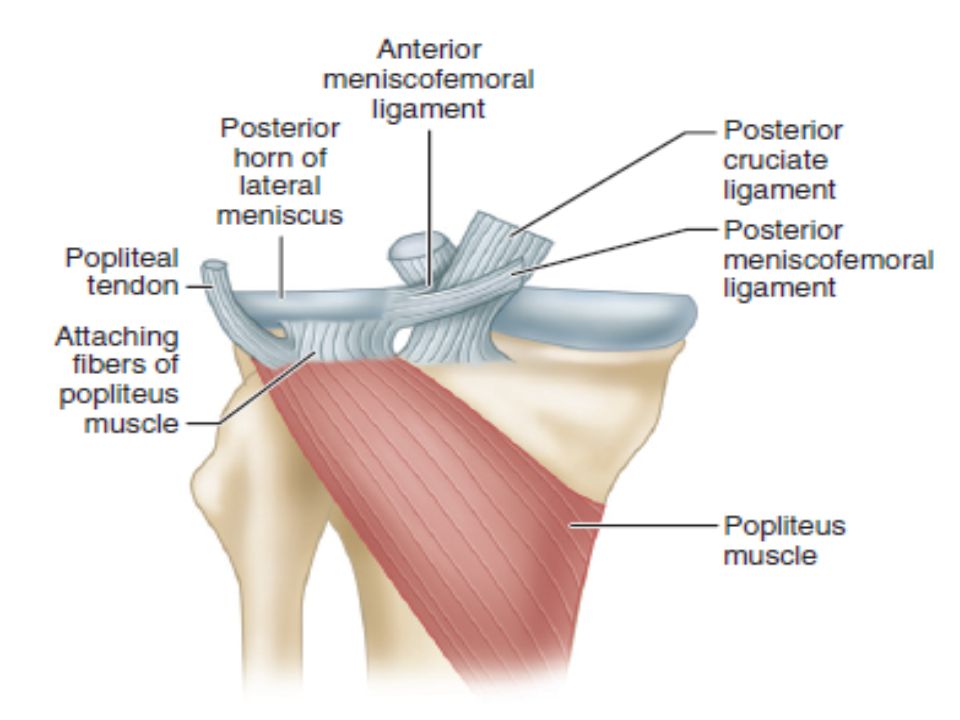
Anatomy Attached to the capsule except where the popliteus tendon is interposed laterally Loosely attached to the tibial plateaus by the coronary ligaments Avascular except near their peripheral attachments

13
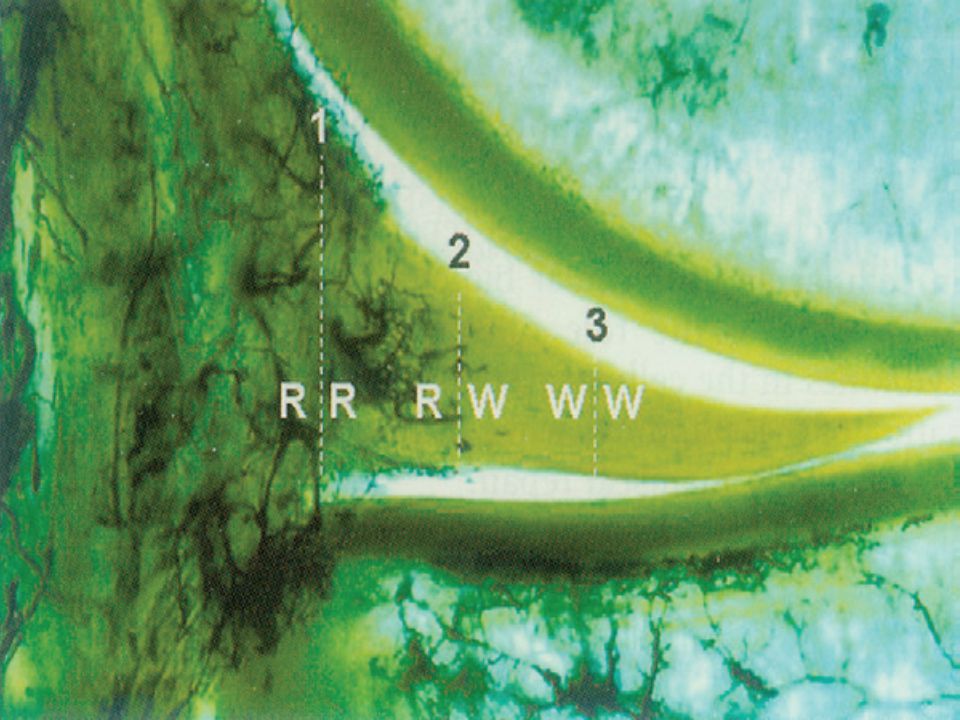
Vascular supply lateral and medial geniculate vessels depth of peripheral vascular penetration is 10% to 30% of the width of the medial meniscus and 10%to 25% of the width of the lateral meniscus

16
FUNCTION A.act as a joint filler, compensating for gross incongruity between femoral and tibial articulating surfaces B.prevent capsular and synovial impingement during flexion- extension

17
function joint lubrication helping to distribute synovial fluid nutrition of the articular cartilage Stability especially rotary stabilizer smooth transition from a pure hinge to a gliding or rotary motion as the knee moves from flexion to extension

19
Load bearing Cover 1/2-to 2/3 of the articular surface Carry40%-70% of weight force medial meniscus 50% Lateral meniscus 70%

21
Effects of meniscectomy Medial meniscectomy ↓contact area by 70% ↑contact stress by 100% Lateral meniscectomy ↓contact area by50% ↑contact stress by 300%

22
Meniscal movement The menisci follow the tibial condyles during flexion and extension during rotation they follow the femur and move on the tibia Medial meniscus:Ant /Post attachments follow the tibia, but its intervening part follows the femur and becomes distorted Lateral meniscus: is firmly attached posteriorly and less likely to be injured

24
Meniscectomy and joint laxity Intact ligaments →little joint laxity Ligamentus insufficiency→↑joint laxity ACL insufficiency→ forces in the medial meniscus increase significantly ACL insufficiency+medial meniscectomy:↑AP translation ACL insufficiency+lateral meniscectomy:↕AP translation

25
MECHANISM OF TEAR rotational force while the joint is partially flexed vigorous internal rotation of the femur on the tibia results in meniscal catching meniscus torn longitudinally when the joint is suddenly extended

29
meniscal tears Longitudinal: The most common type usually involve the posterior segment Most involve the inferior rather than.. the superior surface medial meniscus ≈ lateral meniscus Horizontal/oblique/radial usually lateral meniscus Usually between middle and anterior third

30
Predisposing factors Degeneration Cyst Discoid meniscus Ligament or muscle insufficiency Knee instability Abnormal mechanichal axes

32
DIAGNOSIS History: may not be obtained, especially when tears of abnormal or degenerative menisci in a middle age person Locking or no locking: may not be recognized consider absence of normal recurvatum Usually only with longitudinal bucket handle tear R/O pseudolocking

33
Giving way Is not especific Results from: Muscle(quadriceps) insufficiency Patellar problems Instability Loose body
 insufficiency Patellar problems Instability Loose body")
34
Giving way On rotary movements With a feeling of subluxation or knee jumping Giving way due to meniscal tear During flexion against resistance Walking down stairs Giving way due to other causes

35
Effusion Acute: usually denotes a hemarthrosis, and it can occur when the vascularized periphery of a meniscus is torn Late: Tears occurring within the body of a meniscus or in degenerative areas may not produce a hemarthrosis

36
signs Quadriceps atrophy Joint line tenderness localized to posterolateral or posteromedial(the most important physical finding) Tears of one meniscus can produce pain in the opposite compartment of the knee. This is most commonly seen with posterior tears of the lateral meniscus

37
Mc murray test Palpate posteromedial/ posterolateral Rotate leg external or internal Move knee from full flexion to extension Before 90 ˚→posterior horn After 90˚→mid/ant horn

38
Apley grind test Check menisci during compression

39
squat test Pain localized to joint line is more important than pain during ext/int rotation

40
Thessaly test Knee in 5 ˚ and 20˚ flexion Accuracy rate 95% Always done on the normal knee first to teach the pt

42
paraclinic X ray: routine AP/LAT/intercondylar/sky line views Arthrography MRI: sensitivity → 65% specificity →95% accuracy→85%

43
NONOPERATIVE MANAGEMENT cylinder cast or knee immobilizer worn for 4 to 6 weeks Strengthen muscles around the knee as well as the hip

44
criteria ZONE TEAR TYPE CHRONICITY SIZE(cm)
")
45
A suitable candidate NonChronic Stable( incomplete or could not be displaced more than 3 mm from the intact peripheral rim) Peripheral <5mm no other pathological condition
 Peripheral <5mm no other pathological condition")
47
Reparability of Meniscal Tears ZONE TEAR TYPE CHRONICITY SIZE(cm)
")
48
Ideal indication Acute 1- to 2-cm Longitudinal Peripheral young individual in conjunction with anterior cruciate ligament reconstruction

50
Open or arthroscopic repair Open: posterior horn peripheral tears if posteromedial or posterolateral capsular reconstructions are being done concurrently Arthroscopic: lateral meniscus necessary for tears at or near the junction of the vascular and avascular zones Medial menisci tears that extend deep to the collateral ligament

51
DO NOT FORGET For younger,active patients,ligamentous stabilizationshould accompany meniscal suture because of thedecreased likelihood of healing and increased risk of re-rupture in a knee with ligamentous laxity

53
MENISCECTOMY Increasing degenerative changes were noted, especially after total meniscectomy After subtotal excision degeneration is localized degenerative change directly proportional to the amount of meniscus removed

54
Complete or incomplete Complete removal of the meniscus is justified only when it is irreparably torn Total meniscectomy is no longer considered the treatment of choice in young athletes Subtotal excision is easier by arthroscopy

55
LATE CHANGES AFTER MENISCECTOMY meniscectomy often is followed by degenerative changes within the joint after partial medial meniscectomy 88% to 95% of patients reporting good to excellent results.

56
AUTOGRAFTS AND ALLOGRAFTS Indications: skeletally mature too young for TKA significant pain and limited function conservative therapy failed mechanical tear no synovial disease younger than 40 years normal mechanical alignment stable knee Outerbridge grade I or grade II articular cartilage changes pain localized to the affected compartment

57
AUTOGRAFTS AND ALLOGRAFTS Contraindications knee instability varus-valgus malalignment advanced osteoarthritis is an absolute contraindication

58
questions remain about their survivorship and function

59
THE END

Similar presentations
















>")











 Pelvic girdle.>")




