Download presentation
Presentation is loading. Please wait.

1
Faculty of nursing CHEM 203 Biochemistry UNIT VIII Diagnostic Enzymes Dr.Ola Fouad Talkhan

2
Enzymes in Clinical Diagnosis Plasma enzymes can be classified into two major groups: First, a relatively small group of enzymes are actively secreted into the blood by certain cell types. For example, the liver secretes zymogens (inactive precursors) of the enzymes involved in blood coagulation. Dr.Ola Fouad Talkhan
 of the enzymes involved in blood coagulation. Dr.Ola Fouad Talkhan.")
3
Second, a large number of enzyme species are released from cells during normal cell turnover These enzymes almost always function intracellularly, and have no physiological use in the plasma. In healthy individuals, the levels of these enzymes are fairly constant, and represent a steady state in which the rate of release from damaged cells into the plasma is balanced by an equal rate of removal of the enzyme protein from the plasma. Increased plasma levels of these enzyme may indicate tissue damage. Dr.Ola Fouad Talkhan

7
Different organs frequently contain characteristic properties of different isoenzymes. The pattern of isoenzymes found in the plasma may, therefore, serve as a means of identifying the site of tissue damage. For example, the plasma levels of creatine kinase (CK) are commonly determined in the diagnosis of myocardial infarction. They are particularly useful when the electrocardiogram is difficult to interpret, such as when there have been previous episodes of heart disease. Dr.Ola Fouad Talkhan
 are commonly determined in the diagnosis of myocardial infarction. They are particularly useful when the electrocardiogram is difficult to interpret, such as when there have been previous episodes of heart disease. Dr.Ola Fouad Talkhan.")
8
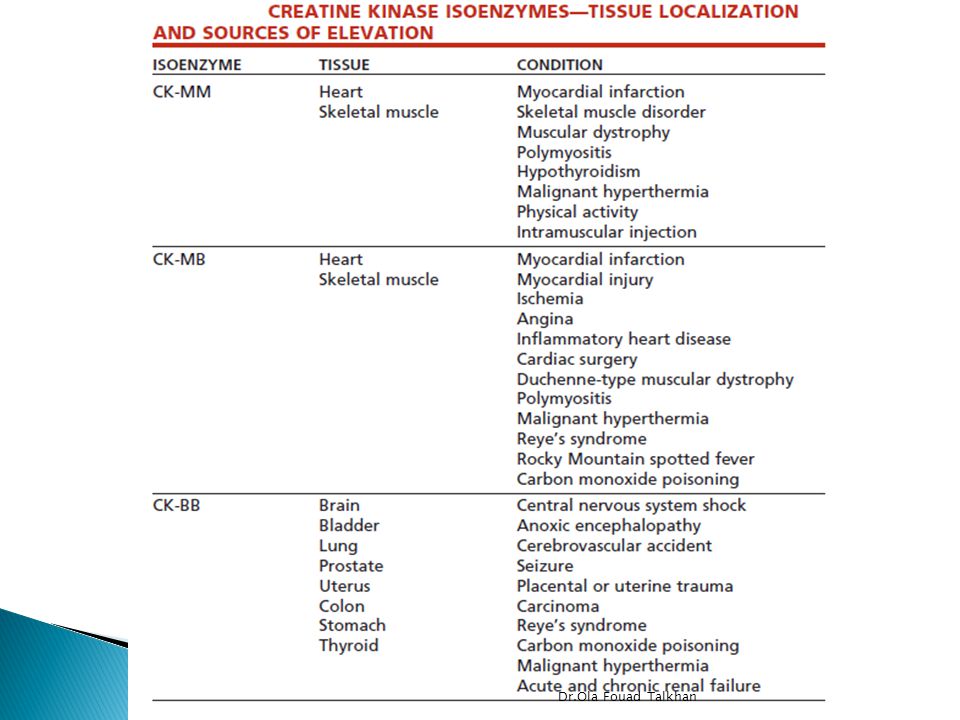
Quaternary structure of isoenzymes Many isoenzymes contain different subunits in various combinations. For example, creatine kinase (CK) occurs as three isoenzymes. Each isoenzyme is a dimer composed of two polypeptides (called B and M subunits) associated in one of three combinations: CK1 = BB, CK2 = MB, and CK3 = MM. Each CK isoenzyme shows a characteristic electrophoretic mobility. Note: Virtually all CK in the brain is the BB isoform, whereas in skeletal muscle it is MM. In cardiac muscle, about one-third is MB with the rest as MM Dr.Ola Fouad Talkhan
 occurs as three isoenzymes. Each isoenzyme is a dimer composed of two polypeptides (called B and M subunits) associated in one of three combinations: CK1 = BB, CK2 = MB, and CK3 = MM. Each CK isoenzyme shows a characteristic electrophoretic mobility. Note: Virtually all CK in the brain is the BB isoform, whereas in skeletal muscle it is MM. In cardiac muscle, about one-third is MB with the rest as MM Dr.Ola Fouad Talkhan.")
9
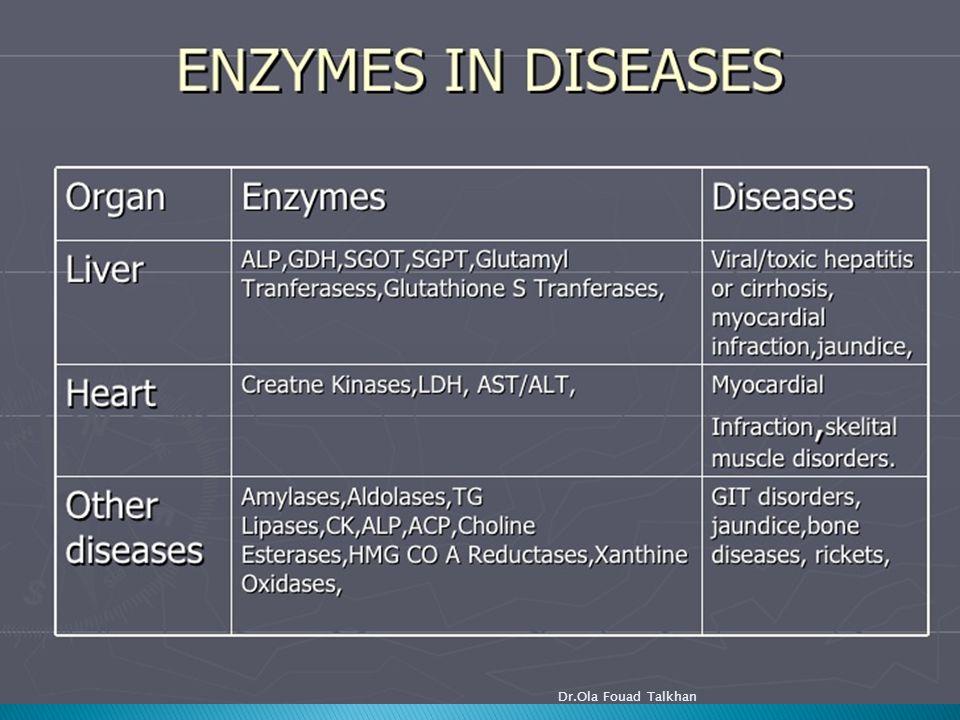
Serum enzymeMajor diagnostic use Aminotransferases aspartate aminotransferase AST,or SGOT alaninaminotransferase ALT,or SGPT Y-glutamyl transferase Amylase Creatin kinase Phosphatase,acid Phosphatase,alkaline Lipase Lactate dehydrogenase isozyme5 ceruloplasmin Myocardial infarction,liver dis. viral hepatitis Various Liver diseases Acute pancreatitis,GIT disorders Myocardial infarction, muscle disorders Metastatic carcinoma of the prostate Various bone disorders, obstructive liver diseases Acute pancreatitis Liver diseases Hepatolenticular degeneration( Wilson’s dis.) Dr.Ola Fouad Talkhan
 Dr.Ola Fouad Talkhan.")
11
Diagnosis of myocardial infarction Measurement of blood levels of proteins with cardiac specificity is used in diagnosis of myocardial infarction (MI) because myocardial muscle is the only tissue that contains more than 5% of the total CK activity as the CK2 (MB) isoenzyme. 1-Creatine Kinase a. Begins to rise 4-6 hours after MI; peak at 24 hrs; returns to normal in 3-5 days. b. Isoenzymes: i. CK-MM fraction = found in skeletal muscle ii. CK-MB fraction = found in heart muscle iii. CK-BB = found in the brain Dr.Ola Fouad Talkhan

12
c. May be increased in other conditions: physical exertion, postoperatively, convulsions, delirium tremens, etc; hence not diagnostic for MI unless the CK-MB fraction is being assayed: rises in 3- 4 hours after MI; peak 12-14 hrs later and returns to normal in 2 days. 2. Lactate Dehydrogenase a. Peak level about 36- 40 hrs after MI and thus of diagnostic value in patients admitted > 48 hrs after infarction. b. Levels return to normal in 5-14 days Dr.Ola Fouad Talkhan

15
Serum transaminases ALT AST Serum alkaline phosphatase ALP Dr.Ola Fouad Talkhan

16
In liver cell injury, damage to the membrane of cells and organelles allows intracellular enzymes to leak into the blood. Where their elevated concentrations can be measured Serum transaminasesSerum alkaline phosphatase Dr.Ola Fouad Talkhan

18
Serum transaminases AST or SGOT=<35U/L ALT or SGPT=<40U/L S. alkaline phosphatase ALP= 3-13KA units/dl ALP is normally excreted through bile ↑↑↑ In obstructive jaundice Dr.Ola Fouad Talkhan

19
EnzymePrehepatic Jaundice Hepatic Jaundice Obstructive Jaundice ALT or ASTUsually normalMarked increase 500-1500IU/L Increased 100-300IU/L ALPNormalIncreased slightly < 30KA/dl Marked increase >30KA/dl Dr.Ola Fouad Talkhan

20
Normal range: 10-47IU/L Serum γ -Glutamyl Transferase Normal range: 2-17IU/L Serum 5’-Nucleotidase Normal range: 70-240IU/L Serum Lactate Dehydrogenase Dr.Ola Fouad Talkhan

21
Alkaline phosphatases Alkaline phosphatase (ALP) belongs to a group of enzymes that catalyze the hydrolysis of various phosphomonoesters at an alkaline pH. Tissue Source ALP activity is present on cell surfaces in most human tissue. The highest concentrations are found in the intestine, liver, bone, spleen, placenta, and kidney. In the liver, the enzyme is located on both sinusoidal and bile canalicular membranes; activity in bone is confined to the osteoblasts, those cells involved in the production of bone matrix. The specific location of the enzyme within this tissue accounts for the more predominant elevations in certain disorders. Dr.Ola Fouad Talkhan

22
Elevated ALP levels may be observed in various bone disorders. Perhaps the highest elevations of ALP activity occur in Paget’s disease (osteitis deformans). Other bone disorders include osteomalacia, rickets, hyperparathyroidism, and osteogenic sarcoma. In addition, increased levels are observed in healing bone fractures and during periods of physiologic bone growth. Dr.Ola Fouad Talkhan
. Other bone disorders include osteomalacia, rickets, hyperparathyroidism, and osteogenic sarcoma. In addition, increased levels are observed in healing bone fractures and during periods of physiologic bone growth. Dr.Ola Fouad Talkhan.")
23
Acid Phosphatase Acid phosphatase (ACP) belongs to the same group of phosphatase enzymes as ALP and is a hydrolase that catalyzes the same type of reactions. The major difference between ACP and ALP is the pH of the reaction. ACP functions at an optimal pH of approximately 5.0. Tissue Source ACP activity is found in the prostate, bone, liver, spleen, kidney, erythrocytes, and platelets. The prostate is the richest source, with many times the activity found in other tissue. Dr.Ola Fouad Talkhan

24
Diagnostic Significance Historically, ACP measurement has been used as an aid in the detection of prostatic carcinoma, particularly metastatic carcinoma of the prostate. Total ACP determinations are relatively insensitive techniques, detecting elevated ACP levels resulting from prostatic carcinoma in the majority of cases only when the tumor has metastasized. Newer markers, such as prostate-specific antigen (PSA), are more useful screening and diagnostic tools Dr.Ola Fouad Talkhan
, are more useful screening and diagnostic tools Dr.Ola Fouad Talkhan.")
25
Amylase Amylase (AMS) is an enzyme belonging to the class of hydrolases that catalyze the breakdown of starch and glycogen. AMS requires calcium and chloride ions for its activation. Tissue Source The acinar cells of the pancreas and the salivary glands are the major tissue sources of serum AMS. Lesser concentrations are found in skeletal muscle and the small intestine and fallopian tubes. AMS is the smallest enzyme, Dr.Ola Fouad Talkhan

26
Other disorders causing an elevated serum AMS level include salivary gland lesions, such as mumps and parotitis, and other intra-abdominal diseases, such as perforated peptic ulcer, intestinal obstruction, cholecystitis, ruptured ectopic pregnancy, mesenteric infarction, and acute appendicitis. In addition, elevations have been reported in renal insufficiency and diabetic ketoacidosis. Dr.Ola Fouad Talkhan

Similar presentations








 are enzymes that differ in amino acid sequence but catalyze the same.>")







>")

 in Serum (Disodium phenyl phosphate Method)>")




 (EC 3.1.3.1) catalyzes the hydrolysis of phosphate esters in an alkaline environment, resulting in the formation.>")