Download presentation
Presentation is loading. Please wait.

1
Resistant Gram-negative Infections 21 st March 2013 Acute Medicine Study Day Dr Sarah Glover Consultant in Medical Microbiology and Infectious Diseases

2
Overview Resistance in Enterobacteriaceae (‘coliforms’ e.g. E coli, Klebsiella, Enterobacter) ESBLs – what they are ESBLs – why they matter Epidemiology Carbapenemases
 ESBLs – what they are ESBLs – why they matter Epidemiology Carbapenemases.")
3
Case 1 90M Background of DM, CRF, previous pneumonia Care home resident, bed bound fully dependent, long term urinary catheter Admitted SOB, CRP >250 WCC 35 ?LRTI Started cefuroxime plus clarithromycin as hx of penicillin allergy 24 hrs into admission, blood cultures flagged positive with Gram negative bacilli Looking at previous microbiology: MSU from a month earlier: ESBL-positive E coli Changed to meropenem

4
Case 1 Following day, BC isolate confirmed as ESBL producing E coli, resistant to trimethoprim, co-amoxiclav, cefuroxime, ciprofloxacin. Sensitive to meropenem and gentamicin CSU from admission, mixed growth of 3 organisms including ESBL-producing E coli with the same sensitivity pattern Good clinical response to carbanepenem treatment

5
β-lactams & β-lactamases β-lactam antibiotics: -penicillins -cephalosporins -carbapenems Inhibit cell wall formation β lactamases = bacterial enzymes that hydrolyse β lactam antibiotics rendering them inactive

6
β-lactams

7
β-lactamases Resistance to penicillins such as ampicillin or amoxicillin very common among coliforms, due to β lactamases (TEM or SHV) –E.g. 60% of invasive E coli isolates in UK are amp-/amoxicillin-resistant)
.")
8
β-lactamases Urine culture Auth 10^5 Escherichia coli /ml Amoxicillin R Nitrofurantoin S Cefalexin/cefradine SCiprofloxacin S Co-amoxiclav SGentamicin S Trimethoprim S

9
Extended-spectrum β-lactamases (ESBLs) ESBLs are a group of β lactamases which are capable of hydrolysing (and therefore causing resistance to) not only penicillins, but many other β lactams, including 2 nd and 3 rd generation cephalosporins Initially recognised in clinical isolates of Klebsiella pneumoniae in the 1980s, derived from TEM or SHV β lactamases by point mutation Until 2000, most were TEM/SHV
 ESBLs are a group of β lactamases which are capable of hydrolysing (and therefore causing resistance to) not only penicillins, but many other β lactams, including 2 nd and 3 rd generation cephalosporins Initially recognised in clinical isolates of Klebsiella pneumoniae in the 1980s, derived from TEM or SHV β lactamases by point mutation Until 2000, most were TEM/SHV")
10
ESBLs Since then, CTX-M increasingly prevalent – more than 50 distinct enzymes identified – transferred via plasmids from environmental bacteria (Kluyvera) Initially found in South America, now global problem, including in community acquired E coli Increasing due to plasmid spread plus clonal expansion eg CTX-M-15 in UK
 Initially found in South America, now global problem, including in community acquired E coli Increasing due to plasmid spread plus clonal expansion eg CTX-M-15 in UK")
11
ESBLs Urine culture Auth 10^5 Escherichia coli /ml Amoxycillin R Cefalexin/cefradine R Cefuroxime R Cefotaxime R Ceftazidime R

12
Clinical relevance – Antibiotic management Now present in the most common Gram- negative infector of humans (E.coli) Difficult to treat Resistant to most beta-lactams including 3 rd generation cephalosporins ESBL + isolates often display co-resistance to other classes of antibiotics e.g. trimethoprim, fluoroquinolones, aminoglycosides Penicillin-inhibitor combinations (e.g. co- amoxiclav, pip-tazo) may appear sensitive in vitro but often result in treatment failure
 may appear sensitive in vitro but often result in treatment failure.")
13
ESBLs Urine culture Auth 10^5 Escherichia coli /ml Amoxycillin R Trimethoprim R Cefuroxime R Ciprofloxacin R Cefalexin/cefradine RGentamicin R Cefotaxime R Augmentin (S) Ceftazidime R Tazocin (S)
 Ceftazidime R Tazocin (S)")
14
Clinical relevance – Antibiotic management Outpatient management of uncomplicated UTI – limited oral & once-daily IV options

15
Clinical relevance – Antibiotic management Surviving sepsis – early initiation of appropriate antimicrobials important factor in determining outcome Studies have shown that mortality from sepsis due to multi-resistant bacteria is double that of sensitive bacteria

16
Clinical relevance – Epidemiology E. coli and Klebsiella pneumoniae are the major ESBL producers worldwide E. coli is primary commensal of the human bowel and the commonest causes in community and hospital settings of: –UTI –Intra-abdominal sepsis –Bacteraemia

17
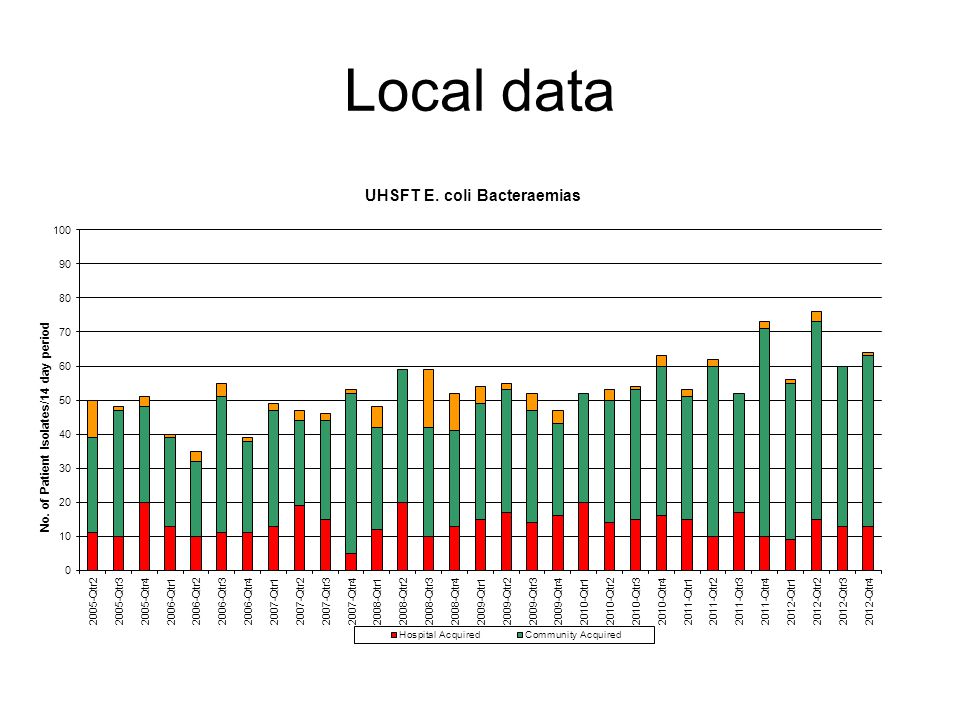
Clinical relevance – Epidemiology Gram negative infection is increasingly common Bacteraemia due to coliforms, particularly E coli, is increasing: E coli is the commonest cause of bacteraemia in England

18
Bacteraemia

19
35% increase in E coli bacteraemias in England, Wales and N Ireland between 2007-2011, compared with a 7% decrease in all bacteraemias

20
E coli bacteraemia by age HPA voluntary data Livermore, D. Tracing, tracking and tackling the big beasts of bacteraemia - Resistance and treatment issues in bloodstream infections ? E. coli. in Federation of Infection Societies (FIS) Scientific Meeting. 2012. Liverpool, UK, Abstract. SA62
 Scientific Meeting Liverpool, UK, Abstract. SA62.")
21
Local data

23
Resistance 10% of E coli bacteraemia isolates from UK were resistant to 3 rd generation cephalosporins in 2011

24
Resistance in E coli bacteraemia HPA voluntary data Livermore, D. Tracing, tracking and tackling the big beasts of bacteraemia - Resistance and treatment issues in bloodstream infections ? E. coli. in Federation of Infection Societies (FIS) Scientific Meeting. 2012. Liverpool, UK, Abstract. SA62
 Scientific Meeting Liverpool, UK, Abstract. SA62.")
25
Risk factors for resistance Elderly Antibiotic exposure (third generation cephalosporins, quinolones) Healthcare contact Travel from higher prevalence areas But many pts have no risk factors
 Healthcare contact Travel from higher prevalence areas But many pts have no risk factors")
26
2007 2011

27
Local data

28
ESBL-E.coli in urine (UHS, 2009-2012) Concomitant resistance to: Trimethoprim 83% Ciprofloxacin 69% Nitrofurantoin 5% Gentamicin 25% Local data
 Concomitant resistance to: Trimethoprim 83% Ciprofloxacin 69% Nitrofurantoin 5% Gentamicin 25% Local data")
29
Antibiotic options Carbapenems widely considered antibiotic of choice for severe ESBL infection: good clinical outcome data when compared with other agents with in-vitro susceptibility Aminoglycosides, if susceptible Quinolones, if susceptible Nitrofurantoin, if susceptible, for uncomplicated UTI only Other orals: fosfomycin, pivmecillinam Tigecycline

30
So why not give everyone meropenem?

31
Kieran Hand, Consultant pharmacist UHS

33
Case 2 28M with congenital biliary dilatation Presented Sept 2012 with biliary sepsis Recurrent sepsis with bacteraemia since then Not amenable to drainage, awaiting liver transplant Klebsiella pneumoniae recurrently isolated: sensitive only to ertapenem, meropenem, amikacin and colistin Repeated courses of carbapenem treatment Frequent relapses after standard courses therefore treated with 6 week course of ertapenem

34
During 6 th week of treatment, fever recurred with breakthrough bacteraemia Isolate now ertapenem resistant Treated with meropenem for 2 weeks Developed eosinophilia and itch, meropenem stopped Recurrent symptoms within 48 hours of stopping, with recurrent bacteraemia on admission 2 days later

35
Isolate showing reduced susceptibility to carbapenems: ref lab report suggests possible metallo-carbapenamase Pt is antibiotic dependent Source control impossible without transplant Very limited antibiotic options

38
Dangers of meropenem overuse Emergence of carbapenem resistance, esp. K. pneumoniae Carbapenemases: –E.g. KPC, NDM-1, VIM, OXA-48 Other mechanisms: –Accumulation of different β-lactamases –Hyper-production of β-lactamases –Cell membrane porin loss (loss of permeability) –Combinations of the above
 –Combinations of the above.")
39
Carbapenemase-producing Enterobacteriaceae referred to Health Protection Agency (Colindale) 2003 to 2011
 2003 to 2011")
40
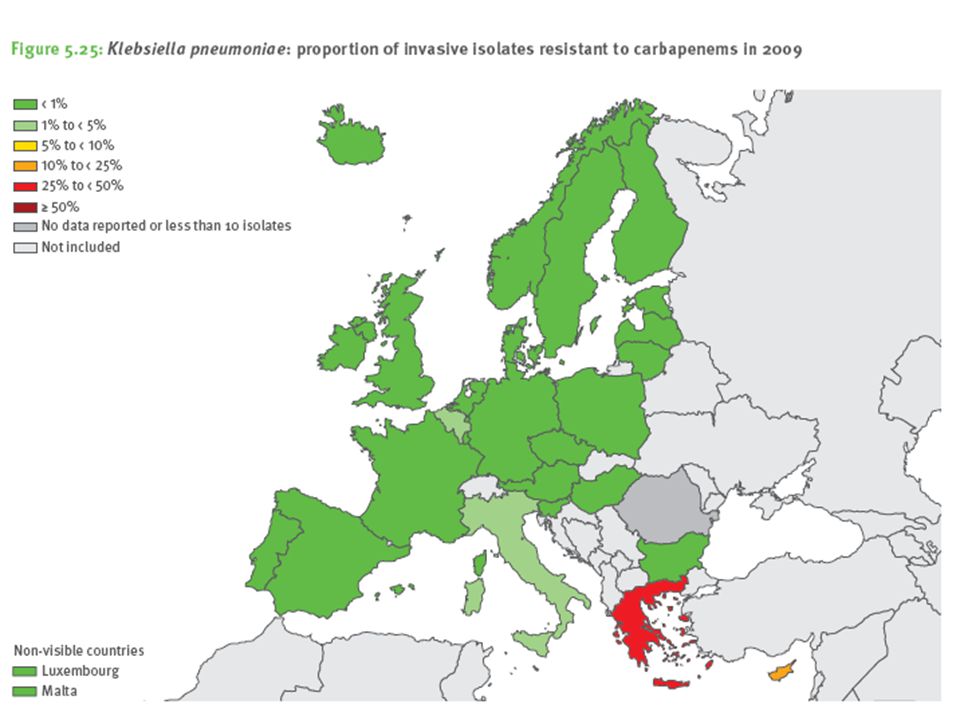
KPC most prominent – first reported in USA, since 2006 has spread across US, Israel, Greece, Italy with outbreaks in China, Brazil, other European countries. 40% prevalence in Klebsiella pneumoniae bacteraemia in Greece NDM occurs in 2-8% of Enterobacteriaceae in teaching hospitals in India, and 27% of inpatients at two military hospitals in Pakistan were carriers

41
Antibiotic suceptibilities of carbapenemase-producing Enterobacteriaceae from the UK Health Protection Agency

42
Colistin – nephrotoxic and neurotoxic Tigecycline – low blood concentrations, unsuitable for UTI as only 22% excreted in urine Fosfomycin – borderline susceptibility common in Klebsiella. Not marketed in UK but can import

43
Control Organisms present in gut Selected for by use of carbapenems, become predominant flora: judicious use of antibiotics Control spread: isolation (particularly diarrhoea), handwashing, identification of carriers, ANTT of drains, environmental cleaning Controlling source of infection – pts with undrainable abdominal sepsis present high risk for breeding resistance
, handwashing, identification of carriers, ANTT of drains, environmental cleaning Controlling source of infection – pts with undrainable abdominal sepsis present high risk for breeding resistance")
44
Take home points 1.E coli causing a rising number and proportion of bacteraemias 2.Resistance to carbapenems a genuine threat 3.Look at previous microbiology results when choosing empirical treatment regimens for sepsis 4.Carbapenems should be used judiciously

48
Health Protection Agency

49
Local data

Similar presentations




















 LTC Steven Mahlen, PhD, D(ABMM)>")


