Download presentation
Presentation is loading. Please wait.

1
Complications of Suppurative Otitis Media
Dr. Vishal Sharma

2
Definition Infection spreads beyond muco-periosteal lining of middle ear cleft to involve bone & neighboring structures like facial nerve, inner ear, dural venous sinuses, meninges, brain tissue & extra-temporal soft tissue.

3
Features of Complications
Severe otalgia, painful swelling around ear Vertigo, nausea, vomiting Headache + blurred vision + projectile vomiting Fever + neck rigidity + irritability / drowsiness Facial asymmetry Otorrhoea + Retro-orbital pain + diplopia Ataxia

4
Classification Intra-cranial Extra-cranial, Intra-temporal
Extra-cranial, Extra-temporal Systemic: septicemia, otogenic tetanus

5
Classification

6
Intra-cranial Complications
Extra-dural abscess Subdural abscess Meningitis Brain abscess Lateral Sinus thrombophlebitis Otitic hydrocephalus Brain fungus (fungus cerebri)
")
7
Intra-temporal Complications
Acute mastoiditis Coalescent mastoiditis Masked mastoiditis Facial nerve palsy Labyrinthitis Labyrinthine fistula Apex Petrositis (Gradenigo syndrome)
")
8
Extra-temporal Complications
Post-auricular abscess Bezold abscess Citelli abscess Luc abscess Zygomatic abscess Retro-mastoid abscess

9
Factors Affecting Pathogen Factors Patient Factors
High virulence bacteria Young age Antimicrobial resistance Poor immune status Chronic disease (DM, TB) Physician Factors Poor socio-economic status Non-availability Lack of health awareness Injudicious antibiotic use Error in recognizing dangerous symptoms & signs
 Physician Factors Poor socio-economic status. Non-availability Lack of health awareness. Injudicious antibiotic use. Error in recognizing dangerous symptoms & signs.")
10
Routes of entry 1. Bony erosion (cholesteatoma destruction, osteitis)
2. Retrograde Thrombophlebitis 3. Anatomical pathway: oval window, round window, internal auditory canal, suture line, cochlear & vestibular aqueduct 4. Congenital bony defects: facial canal, tegmen plate 5. Acquired bony defects: fracture, neoplasm, stapedectomy 6. Peri-arteriolar space of Virchow-Robin: spread into brain

11
Erosion of tegmen tympani

12
Coalescent Mastoiditis or Surgical Mastoiditis

13
Pathogenesis Aditus Blockage Failure of drainage
Stasis of secretions Hyperemic decalcification Resorption of bony septa of air cells Coalescence of small air cells to form cavity Empyema of mastoid cavity

14
Pathogenesis

15
Clinical Features & Investigation
Otorrhoea > 2 weeks, otalgia & deafness Mastoid reservoir sign: pus fills up on mopping Sagging of postero-superior canal wall due to peri-osteitis of bony wall b/w antrum & posterior E.A.C. Ironed out appearance of skin over mastoid due to thickened periosteum Mastoid tenderness present Mastoid cavity in X-ray & CT scan

16
Mastoid reservoir sign

17
Sagging of posterior wall

18
Ironed out appearance

19
Mastoid cavity

20
Mastoid cavity

21
Mastoiditis Furunculosis
H/o otitis media + - Deafness Position of pinna Down + outward + forward Forward Post-aural groove Deepened Obliterated Ear discharge Muco-purulent Serous / purulent Sagging of EAC wall TM congestion Tenderness Mastoid Tragal Post-aural lymph node X-ray Mastoid Coalescence of cells + cavity Normal

22
Treatment Urgent hospital admission Broad spectrum I.V. antibiotics
No response to medical treatment in 48 hrs Development of new complication Presence of sub-periosteal abscess Myringotomy to drain out painful pus Incision drainage of sub-periosteal abscess Cortical Mastoidectomy

23
Sub-periosteal abscess & fistula

24
Pathology Production of pus under tension
hyperaemic decalcification (halisteresis) + osteoclastic resorption of bone sub-periosteal abscess penetration of periosteum + skin fistula formation
 + osteoclastic resorption of bone. sub-periosteal abscess. penetration of periosteum + skin. fistula formation.")
25
Sub-periosteal abscess formation

26
Sub-periosteal fistula: dry

27
Sub-periosteal fistula: wet

28
Types of sub-periosteal abscess
Post-auricular Bezold Citelli Zygomatic Luc Retro-mastoid Parapharyngeal & Retropharyngeal

29
Types of sub-periosteal abscess

30
Post-auricular abscess
Commonest. Present behind the ear. Pinna pushed forward & downward.

31
Bezold & Citelli abscesses
Bezold: neck swelling over sternocleido- mastoid muscle Citelli: neck swelling over posterior belly of digastric muscle

32
D/D of Bezold’s abscess
Suppurative lymphadenopathy of upper deep cervical lymph node Para-pharyngeal abscess Parotid tail abscess Infected branchial cyst Internal jugular vein thrombosis

33
Luc: swelling in external auditory canal
Zygomatic: swelling antero-superior to pinna + upper eyelid oedema Retro-mastoid: swelling over occipital bone (? Citelli’s abscess) Parapharyngeal & Retropharyngeal: due to spread of pus along Eustachian tube
 Parapharyngeal & Retropharyngeal: due to spread. of pus along Eustachian tube.")
34
Retromastoid abscess

35
Incision drainage of abscess

36
Gradenigo syndrome Persistent otorrhoea: despite adequate
cortical mastoidectomy Retro-orbital pain: Trigeminal nv involvement Diplopia: convergent squint due to lateral rectus palsy by injury to abducent nv in Dorello’s canal under Gruber’s petro-sphenoid ligament, at petrous apex

37
Persistent otorrhoea + Retro-orbital pain +
Convergent squint

38
Right Convergent squint
Right gaze Central gaze Left gaze

39
Etiology: Coalescent mastoiditis involving petrous apex along postero-superior & antero-inferior tracts in relation to bony labyrinth Diagnosis: 1. C.T. scan temporal bone for bony details. 2. M.R.I. to differ b/w bone marrow & pus Treatment: Modified radical mastoidectomy & clearance of petrous apex cells

40
C.T. scan & M.R.I.

41
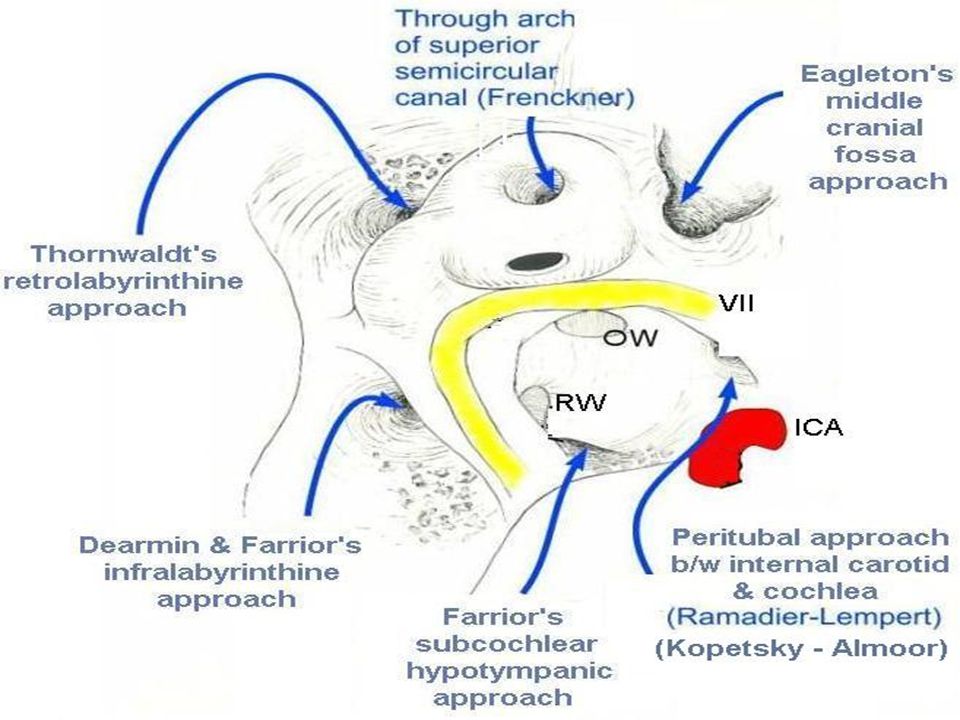
Hearing preserving approaches to petrous apex
Eagleton’s middle cranial fossa approach Frenckner’s subarcuate approach Thornwaldt’s retro-labyrinthine approach Dearmin & Farrior’s infra-labyrinthine approach Farrior’s hypotympanic sub-cochlear approach Lempert Ramadier’s peri-tubal approach Kopetsky Almoor’s peri-tubal approach

43
Hearing sacrificing approaches to petrous apex
Trans-cochlear approach Trans-labyrinthine approach

44
Spread of pus

45
Labyrinthitis

46
Introduction Inflammation of endosteal layer of bony labyrinth
Route of infection: Round window membrane Pre-formed opening (Stapedectomy) Retrograde spread of meningitis via IAC / aqueducts Clinical forms: 1. Circumscribed (labyrinthine fistula) 2. Diffuse serous 3. Diffuse suppurative
 Retrograde spread of meningitis via IAC / aqueducts. Clinical forms: 1. Circumscribed (labyrinthine fistula) 2. Diffuse serous 3. Diffuse suppurative.")
47
Circumscribed: Fistula commonly involves lateral SCC
Circumscribed: Fistula commonly involves lateral SCC. Presents with transient vertigo & positive fistula test I/L nystagmus with +ve pressure; C/L nystagmus with -ve pressure Serous: Reversible, non-purulent, mild vertigo, I/L nystagmus, mild sensori-neural hearing loss Purulent: Irreversible, purulent, severe vertigo, C/L nystagmus, severe / profound hearing loss

48
Treatment: Bed rest (affected ear up). Avoid head movement.
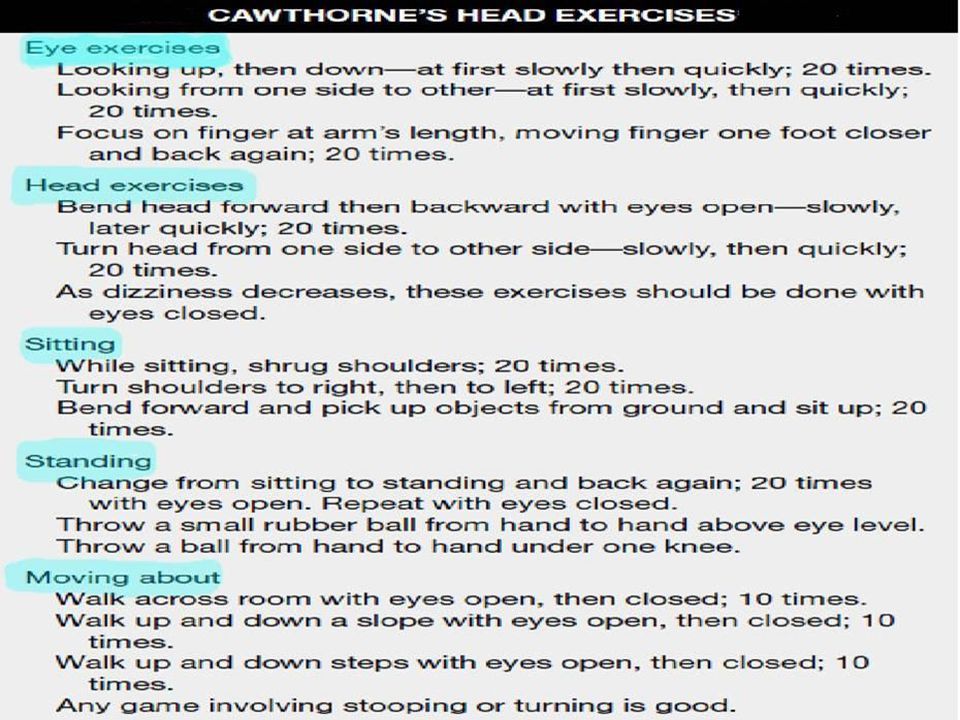
Labyrinthine sedative: Prochlorperazine, Cinnarizine Broad spectrum I.V. antibiotics Modified Radical Mastoidectomy: removes infection Open labyrinthine fistula: cover with temporalis fascia Fistula covered with cholesteatoma matrix < 2 mm: remove matrix & cover with temporalis fascia > 2 mm / multiple / over promontory: leave it Rehabilitation by Cawthorne-Cooksey Exercises

49
Lateral SSC Fistula

51
Facial nerve paralysis
Within 1st wk: due to nerve sheath edema After 2 wks: due to bone erosion Lower motor neuron palsy Common in tubercular otitis media Treatment: Modified Radical Mastoidectomy Facial nerve decompression seldom required

52
Meningitis

53
High grade persistent fever with rigors
Severe headache & neck stiffness Irritability drowsiness confusion coma Neck rigidity positive Kernig sign positive; Brudzinski sign positive Papilloedema Lumbar Puncture: cell count, protein, sugar I.V. Ceftriaxone + Metronidazole + Gentamicin Radical Mastoidectomy once patient is stable

54
Test for neck rigidity

55
Otogenic brain abscess

56
Introduction 50-75 % adult brain abscess & 25% in child = otogenic
Temporal abscess : Cerebellar abscess = 2:1 Route of infection: 1. Direct spread: via Tegmen plate: Temporal abscess via Trautmann’s triangle: Cerebellar abscess 2. Retrograde thrombophlebitis

57
Trautmann’s triangle Superiorly: superior petrosal sinus
Posteriorly: sigmoid sinus Anteriorly: solid angle (semi-circular canals) Pathway to posterior cranial fossa from mastoid cavity
 Pathway to posterior. cranial fossa from mastoid. cavity.")
58
Stages of brain abscess
1. Invasion or Encephalitis (1-10 days) 2. Localization or Latent Abscess (10-14 days) 3. Expansion or Manifest Abscess (> 14 days): leads to raised intracranial tension & focal signs 4. Termination or Abscess rupture: leads to fatal meningitis
 2. Localization or Latent Abscess (10-14 days) 3. Expansion or Manifest Abscess (> 14 days): leads to raised intracranial tension & focal signs. 4. Termination or Abscess rupture: leads to fatal meningitis.")
59
Stages of brain abscess

60
Clinical Features of ed I.C.T.
Seen more in cerebellar abscess Severe persistent headache, worse in morning Projectile vomiting Blurring of vision & Papilloedema Lethargy drowsiness confusion coma Bradycardia Subnormal temperature

61
Focal Clinical Features
Temporal Lobe Cerebellum Nominal aphasia I/L nystagmus Quadrantic homonymous I/L weakness hemianopia (C/L) I/L hypotonia Epileptic seizures I/L ataxia Pupillary dilatation Intention tremor Hallucination (smell & taste) Past-pointing C/L hemiplegia Dysdiadochokinesia
 I/L hypotonia. Epileptic seizures I/L ataxia. Pupillary dilatation Intention tremor. Hallucination (smell & taste) Past-pointing. C/L hemiplegia Dysdiadochokinesia.")
62
Bacteriology Anaerobic streptococci Streptococcus pneumoniae
Staphylococci Proteus E. coli Pseudomonas Bacteroidis fragilis

63
Investigations CT scan of brain & temporal bone with contrast
Site, size & staging of abscess Observe progression of brain abscess Associated intra-cranial complications MRI brain D/D: pus, abscess capsule, edema & normal brain Spread to ventricles & subarachnoid space Avoid lumbar puncture to prevent coning

64
Temporal abscess in CT scan

65
Cerebellar abscess

66
Medical Treatment High dose broad spectrum I.V. antibiotics: Ceftriaxone + Metronidazole + Gentamicin I.V. Dexamethasone 4mg Q6H: es oedema I.V. 20% Mannitol (0.5 gm/kg): es I.C.T. Anti-epileptics: Phenytoin sodium Antibiotic ear drops & aural toilet
: es I.C.T. Anti-epileptics: Phenytoin sodium. Antibiotic ear drops & aural toilet.")
67
Surgical Treatment Repeated burr hole aspirations
Excision of brain abscess with capsule: best Tx Open incision & evacuation of pus Radical mastoidectomy after pt becomes stable

68
Lateral sinus thrombophlebitis

69
Pathogenesis Lateral sinus = Sigmoid sinus + Transverse sinus
Erosion of sigmoid sinus plate peri-sinus abscess inflammation of outer wall endophlebitis mural thrombus occlusion of sinus lumen intra-sinus abscess propagating infected thrombus

71
Pathogenesis

72
Spread of thrombus Proximal: 1. To superior sagittal sinus via torcula Hirophili hydrocephalus 2. To cavernous sinus proptosis 3. To mastoid emissary vein Griesinger’s sign Distal: To internal jugular vein & subclavian vein pulmonary thrombo-embolism & septicaemia

73
Clinical Features Remittent high fever with rigors (picket fence)
Pitting edema over retro-mastoid area & occipital bone due to mastoid emissary vein thrombosis (Griesinger’s sign) Tenderness along Internal Jugular Vein Headache Anaemia
 Tenderness along Internal Jugular Vein. Headache. Anaemia.")
74
Fever charts in C.S.O.M. Brain abscess Meningitis
Lateral Sinus Thrombophlebitis

75
Picket fence fever High fever, swinging type Chills precedes fever
Temperature subsides with sweating Each fever spike due to release of fresh septic embolus

76
Special Tests Queckenstedt or Tobey-Ayer test: compression of I.J.V. rapid rise of C.S.F. pressure (50 – 100 mm water rapid fall on release of compression. In L.S.T. no rise / rise by only 10 – 20 mm water. Lillie – Crowe - Beck test: pressure on I.J.V. on normal side engorgement of retinal veins + papilloedema seen in fundoscopy due to L.S.T. on opposite side.

77
Tobey Ayer Test

78
Retinal vein dilation & optic disc edema

79
Investigations Lumbar puncture: to rule out meningitis
CT brain with contrast: Delta sign or MRI brain with contrast: Empty triangle sign MR angiography Blood culture Culture & sensitivity of ear discharge Peripheral blood smear: to rule out malaria

80
Delta sign

81
Treatment 1. Radical mastoidectomy: Removal of disease + needle aspiration to confirm diagnosis. Sinus wall incised. Infected clots removed & abscess drained. 2. I.V. Ceftriaxone + Metronidazole + Gentamicin 3. Anticoagulants: in cavernous sinus thrombosis 4. Internal jugular vein ligation: for embolism not responding to antibiotics & surgery 5. Blood transfusion: for anaemia

82
Extra-dural abscess

83
Extra-dural abscess

84
Commonest otogenic intra-cranial complication
Collection of pus b/w skull bone & dura of middle or posterior cranial fossa Majority asymptomatic. Suspected in case of: Profuse, intermittent, pulsatile, purulent, otorrhoea Low grade fever I/L Persistent headache Recurring meningococcal meningitis CT scan brain shows extra-dural abscess Tx: I.V. Ceftriaxone + Metronidazole + Gentamicin Modified Radical mastoidectomy Drill tegmen or sinus plate pus drained

85
Extra-dural abscess

86
Subdural abscess

87
Subdural abscess

88
Collection of pus b/w dura & arachnoid by erosion of bone & dura mater or by retrograde thrombophlebitis Due to rapid spread of pus, symptoms of raised intra-cranial tension & meningeal irritation develop quickly CT scan brain shows subdural abscess Tx: I.V. Ceftriaxone + Metronidazole + Gentamicin Burr hole evacuation of pus Radical mastoidectomy after pt becomes stable

89
Subdural abscess

90
Otitic Hydrocephalus

91
Synonym: Benign intra-cranial hypertension Symond’s syndrome
Etiology: 1. Associated L.S.T. obstruction of cerebral venous return Superior sagittal sinus thrombosis ed C.S.F. absorption Clinical Features: 1. Severe headache, vomiting 2. Blurred vision, papilloedema, optic atrophy 3. Abducens palsy & diplopia due to raised intra-cranial tension (False localizing sign)
")
92
Investigations: 1. Lumbar puncture: ed CSF pressure (> 300 mm H2O). Biochemistry & bacteriology normal 2. CT scan brain: normal ventricles Treatment: 1. Tx of L.S.T.: I.V. antibiotics & MRM 2. se CSF pressure (prevents optic atrophy) by: I.V. Dexamethasone 4mg Q6H I.V. 20% Mannitol 0.5 gm/kg Repeated lumbar puncture / lumbar drain Ventriculo-peritoneal shunt
 by: I.V. Dexamethasone 4mg Q6H. I.V. 20% Mannitol 0.5 gm/kg. Repeated lumbar puncture / lumbar drain. Ventriculo-peritoneal shunt.")
93
Brain Fungus Prolapse of brain into middle ear cavity / mastoid cavity due to erosion of dural plate. Common in pre-antibiotic era. Rarely seen now in resistant infections. Diagnosis: C.T. scan temporal bone. Treatment: Removal of necrotic tissue, replacement of healthy prolapsed brain into cranial cavity & repair of bone defect.

94
Fungus Cerebri

95
Thank You

Similar presentations



 Intracranial (15-20%) Bony (5-10%) Radiography – Computed tomography (CT) best for.>")
















