Download presentation
Presentation is loading. Please wait.

1
Clinical Update on childhood obesity Dr Helen Vickerstaff Consultant Community Paediatrician, RCHT

2
Outline Define obesity in children Be able to assess for aetiology and comorbidity Understand principles of intervention Know local referral routes Not dread that consultation!

3
Definition

4
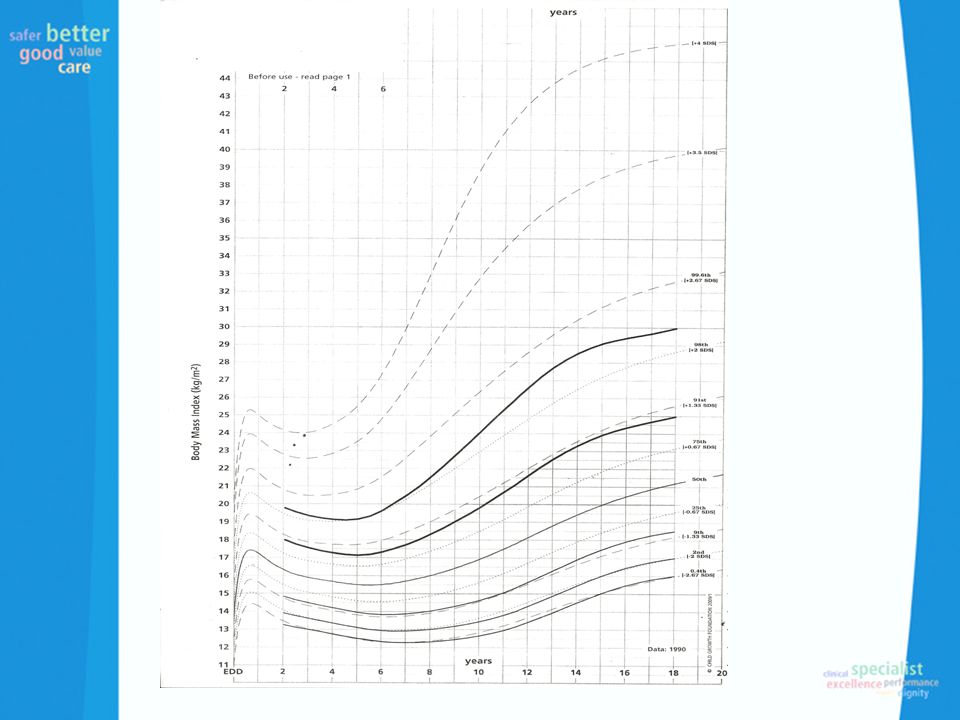
Definition/Standards Obesity is an abnormal accumulation of body fat, usually 20% or more over an individual’s ideal body weight. Clinical BMI >91 st centile overweight BMI >98 th centile obese BMI >3.5 SD extremely obese

6
Definition/standards Differs according to clinical or population monitoring UK90 data BMI centile –85 th and 95 th centile for population –91 st and 98 th clinical assessment

7
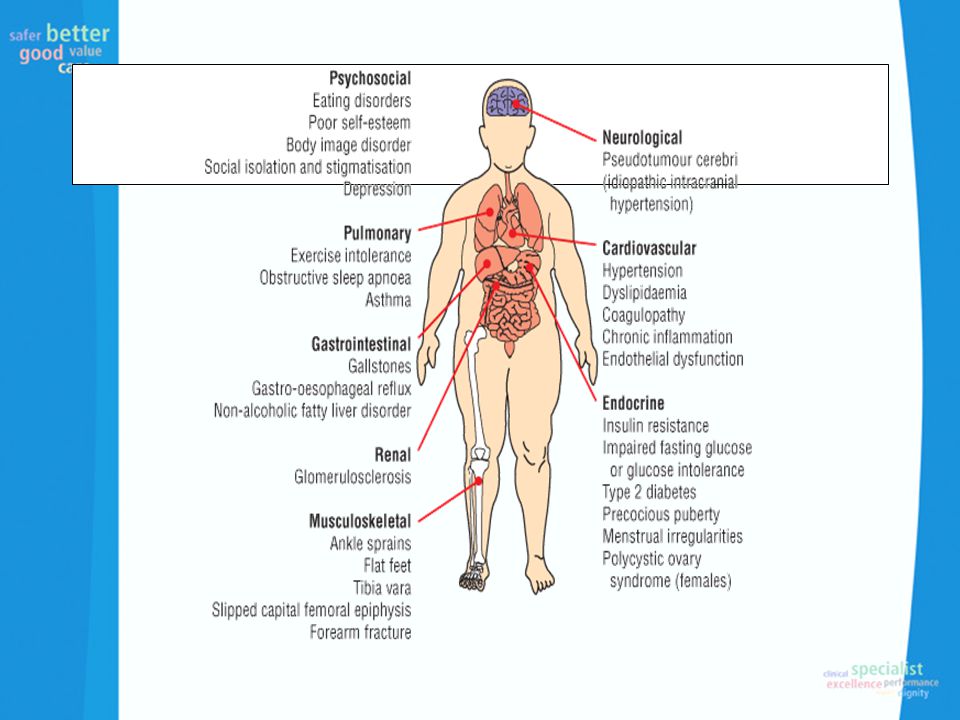
Why should we be worried?

9
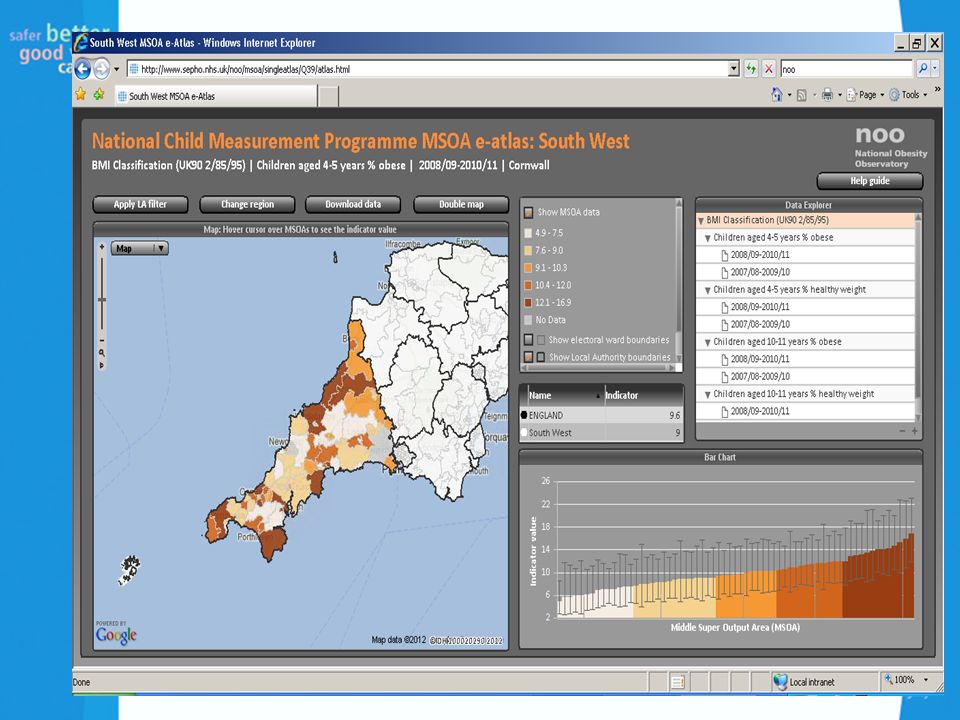
Prevalence Great data sources National Child Measurement Programme (NCMP) National Obesity Observatory (NOO) Chi MAT
 National Obesity Observatory (NOO) Chi MAT")
10
Child prevalence by BMI status National Child Measurement Programme 2010/11 This analysis uses the 2 nd, 85 th and 95 th centiles of the British 1990 growth reference (UK90) for BMI to classify children as underweight, healthy weight, overweight and obese. These thresholds are the most frequently used for population monitoring within England. © NOO 2012

11
Prevalence of obesity among children by school year and sex National Child Measurement Programme 2006/07 – 2010/11 Child obesity: BMI ≥ 95 th centile of the UK90 growth reference © NOO 2012

13
Prevalence Reception age 22.6% –overweight(13.2), obese(9.4) Year 6 33.4% –Overweight (14.4) obese (19.0) South West above national average in reception overweight/obese Cornwall figures similar but below SW average for Year 6 Relatively poor uptake rate 71% vs national 93%
, obese(9.4) Year % –Overweight (14.4) obese (19.0) South West above national average in reception overweight/obese Cornwall figures similar but below SW average for Year 6 Relatively poor uptake rate 71% vs national 93%")
14
Risk Factors

15
Parental obesity Very early (by 43months) adiposity rebound Obese children go on to become obese adults >8 hours screen time/week at 3 years Catch up growth SD score at 8 months and 18 months in top quarter, weight gain in first year Birth weight Short (<10.5 hours) sleep duration at 3 years ALSPAC
 adiposity rebound Obese children go on to become obese adults >8 hours screen time/week at 3 years Catch up growth SD score at 8 months and 18 months in top quarter, weight gain in first year Birth weight Short (<10.5 hours) sleep duration at 3 years ALSPAC")
17
When to worry Over 2 years –BMI > 91 st centile – overweight (tailored intervention) –BMI >98 th centile – assess for co-morbidities Under 2 years –Weight >2 centiles above length –Weight >99.6 th centile –Weight increases across 2 centiles –Severe progressive obesity
 –BMI >98 th centile – assess for co-morbidities Under 2 years –Weight >2 centiles above length –Weight >99.6 th centile –Weight increases across 2 centiles –Severe progressive obesity")
18
Underlying Causes Short for midparental centile Static growth Severe progressive obesity Dysmorphic features Significant learning difficulties Endocrinopathy Cushing’s features

19
Initial assessment – risk factors Family history (sex related) Physical disability Lack of regular physical activity and/or sedentary lifestyle Poor dietary habits Lower socio- economic status Learning disability Syndromes Medications –Corticosteriods –Diabetes mellitus –Psychoactive agents –Antidepressant –ALL treatment –Anti-migraine e.g. pizotifen –Anti-epileptics

21
Syndromes associated Prader Willi sydrome Down’s syndrome Biemond syndrome Alstrom sydrome Bardet-Biedl syndrome Carpenter syndrome Cohen syndrome Borjeson-Forssman-Lehman syndrome

22
Clinical features of concern Severe unremitting obesity Abnormal facies Disorders of eyes Retinal problems Narrow palpebral fissures Abnormal position palpebral fissures Severe squint Skeletal abnormalities polydactyly Syndactyly Kyphoscoliosis Sensorineural deafness Microcephaly and/or abnormal skull shape Learning difficulties Hypotonia Hypogonadism Cryptorchidism Micropenis Delayed puberty

23
Single Gene Abnormalities Congenital leptin deficiency Leptin receptor mutation Pro-hormone convertase 1 mutation Melanocortin 4 receptor mutation

24
Examination

25
Calculate and plot BMI centile or z-score (Waist circumference) Pattern of adiposity BP Pubertal assessment Acanthosis nigricans (insulin resistance) Obstructive sleep apnoea Drug use – glucocorticoids, atypical antipsychotics Genetic obesity syndromes –Early onset –LD –Dysmorphism –Epilepsy –Retinitis –Genitalia –Skeletal –Red hair Endocrinopathy –Hypothyroidism –Cushings – striae, central, rapid progressive
 Pattern of adiposity BP Pubertal assessment Acanthosis nigricans (insulin resistance) Obstructive sleep apnoea Drug use – glucocorticoids, atypical antipsychotics Genetic obesity syndromes –Early onset –LD –Dysmorphism –Epilepsy –Retinitis –Genitalia –Skeletal –Red hair Endocrinopathy –Hypothyroidism –Cushings – striae, central, rapid progressive")
27
Other concerns Family History –Early onset type 2 diabetes < 40 years –CV disease < 60 years

28
Investigation – co-morbidity Routine –Fasting glucose and insulin –Fasting lipid profile (full) –ALT –Urinanalysis –TFT’s Additional –Oral glucose tolerance test –PCOS investigation –Sleep investigation
 –ALT –Urinanalysis –TFT’s Additional –Oral glucose tolerance test –PCOS investigation –Sleep investigation")
29
Investigation - aetiology Genetic studies –Syndromes –Genetics referral is significant concern –Offer inclusion in GOOS (genetics of obesity study) –Thyroid antibodies –Ca/PO4 (pseudohypoparathyr oidism Suspicion of secondary obesity –Height deceleration –Short duration obesity or rapid weight gain –Severe hypertension,acne or hirsuitism
 –Thyroid antibodies –Ca/PO4 (pseudohypoparathyr oidism Suspicion of secondary obesity –Height deceleration –Short duration obesity or rapid weight gain –Severe hypertension,acne or hirsuitism")
30
GOOS Study Research study Look at monogenic causes and also measure leptin levels May provide future treatments Parents like to have a cause Management is the same 10ml clotted blood or buccal swabs for young children

33
Management If no suspected underlying cause established then frequent follow up usually in primary care Multi-strategy approach to healthy weight –Diet, lifestyle and behavioural change –Long term risks –SMART goals –Weight maintenance

34
Management Primary Care – GP, school nurses and health visitors regular training to support via Rachael Brandreth (specialist dietitian) 3 monthly follow up Reduction in BMI SDS or z score by 0.5 reduces atherogenic profile and insulin resistance, inflammatory markers Consider re-referral if develop or worsening co-morbidities or progressive obesity despite intervention
 3 monthly follow up Reduction in BMI SDS or z score by 0.5 reduces atherogenic profile and insulin resistance, inflammatory markers Consider re-referral if develop or worsening co-morbidities or progressive obesity despite intervention")
35
Secondary Care Investigation of aetiology and co-morbidity Multi-component weight management programme Consideration of Orlistat –lipase inhibitor –>12 years with extreme obesity or significant co- morbidities –

36
Surgical Intervention Last possible option in obese adolescents with co-morbidity Not recommended in children Exceptional circumstances close to physiological maturity MDT with full assessment

37
Local Pathways Obesity pathway Assessment in primary care and recognition of co-morbidites/possible underlying aetiology Centralised referral number for weight management strategies (healthy weight team) Tier 1/2 programmes –health visitor HENRY- under 5’s –Keep It in the Family (MEND) – 7-13 years (>91 st centile)
 Tier 1/2 programmes –health visitor HENRY- under 5’s –Keep It in the Family (MEND) – 7-13 years (>91 st centile)")
38
LEAF Programme Fits into NICE and SIGN guidance of behaviour change components, family based, aim to change whole family behaviour. Target decreasing overall dietary intake, increase levels of activity and decrease time spent on sedentary behaviour Evaluation Solution focused

39
Weight Management Programmes in Cornwall Tier 1 and 2 – refer to health visitor or school nurse Tier 2-3 Age 0-6 LEAF programme 7-13 MEND programme (call healthy weight team 01209 310062) 14+ current training SHINE programme (as above)
 14+ current training SHINE programme (as above)")
40
GAPS Special schools – looking at work of programme with school nurses and possibly behavioural team Psychology support Concerns – identify co-morbidities but no guidance on management

41
Child Protection Issue? Childhood obesity alone is not a child protection issue Failure to reduce overweight alone is not a child protection concern (very difficult to treat) Consistent failure to change lifestyle and engage with outside support indicates neglect, particularly in younger children Obesity may be part of wider concerns about neglect or emotional abuse (1/3 adult bariatric report SA) Assessment should include systemic (family and environmental) factors
 Consistent failure to change lifestyle and engage with outside support indicates neglect, particularly in younger children Obesity may be part of wider concerns about neglect or emotional abuse (1/3 adult bariatric report SA) Assessment should include systemic (family and environmental) factors.")
42
Sources of information National Obesity Observatory (NOO) Website NICE guideline (2006) SIGN guideline Map of Medicine OSCA statement (RCPCH) Obesity Services for Children and Adolescent Network Group
 Website NICE guideline (2006) SIGN guideline Map of Medicine OSCA statement (RCPCH) Obesity Services for Children and Adolescent Network Group")
43
Any questions? www.cornwallhealthyweight.org.uk Contact the team on LEAF.programme@cornwall.nhs.uk LEAF.programme@cornwall.nhs.uk

44
‘Katie’ – age 6 BMI 31.9 Mild sleep apnoea Fatty liver Behavioural problems, including stealing Social services involved Joint custody – spends half the week with Mum, other half with Dad Both parents have struggled with their weight Dad has type II diabetes (since 15 yrs) Mum has admitted to having an unhealthy relationship with food Mum has also acknowledged that her relationship with Susie is “too adult”
 Mum has admitted to having an unhealthy relationship with food Mum has also acknowledged that her relationship with Susie is too adult")
Similar presentations











 Heather Donald September 2011.>")









 is a measure used to determine childhood overweight.>")



