Download presentation
Presentation is loading. Please wait.

1
STOMA CARE

2
DEFINITION

3
A stoma is an opening that is created to allow stool or urine to pass out of the body. Although more common in adults, it is not unusual for a child to have ostomy surgery. For some the stoma is carried out as a temporary measure, to allow the gut a period of rest and recovery, whilst for others it may be permanent, having been carried out as a life-saving measure

4
INDICATIONS FOR OSTOMY

5
Some of the most common conditions that might necessitate a stoma are:
Imperforate anus: where there is no exit for the bowel or its contents. Hirschsprungs disease: where nerves called the ganglion nerves are missing and waste matter cannot easily pass. Inflammatory bowel disease: this includes Crohns Disease and Ulcerative Colitis, both inflammatory diseases of the intestines.

6
Neonatal necrotising enterocolitis: this occurs when a portion of the bowel is dead and cannot function and is most common in premature babies who weight less than 3 pounds at birth. In this case a stoma can mean life to a baby. Spina bifida: where part of the spine fails to develop properly and in more severe forms of the disease, the spinal nerves that control the muscles of the legs, bladder and bowels may be affected and a stoma needed.

7
Stomach Large Bowel (colon) Small Bowel (ileum) Rectum
 Small Bowel (ileum) Rectum")
8
Accident, injury and other causes: these include cancer and also injuries to the bowel or bladder
caused by car accidents, etc After surgery, your child will pass stool/ urine through the stoma instead and will not be able to control when this occurs. To help with this a pouch is worn to collect the waste.

9
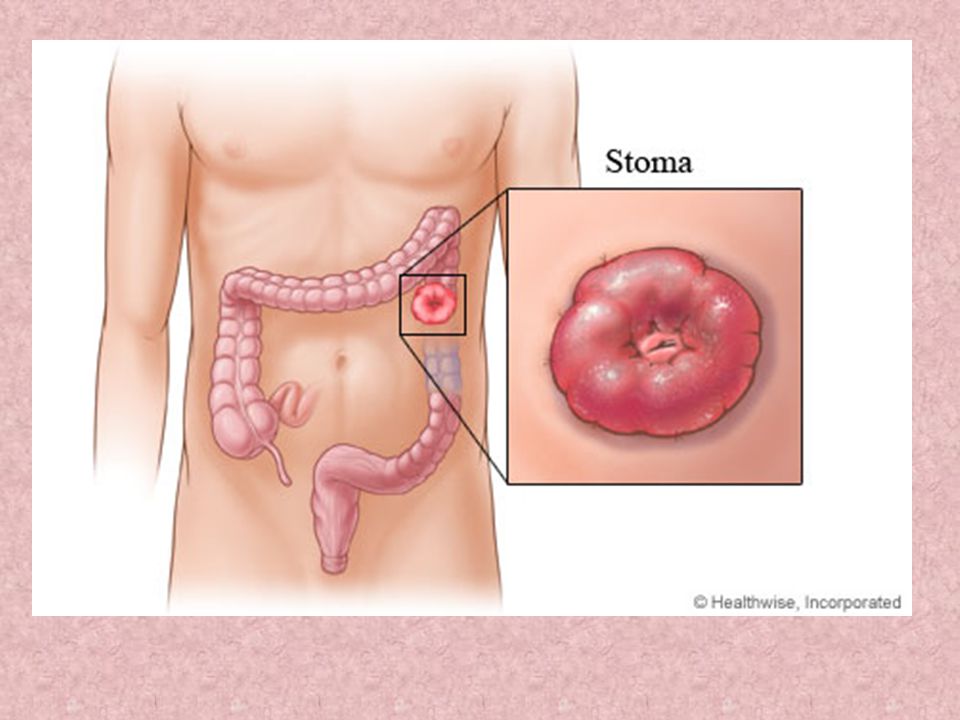
COMMON APPEARANCE OF STOMA

10
Stomas will be a pinkish red in colour, similar to the inside of your mouth, and will be soft and moist. Do not be alarmed if your child’s stoma looks different from other pictures you may have seen as the appearance of the stoma will be unique. It is also common for the stoma and the area around it to be slightly swollen for around 6-8 weeks after surgery, after which the swelling will subside. Sometimes the stoma may bleed a little, for instance if brushed by a towel or dressing. This is entirely normal as stomas have a lot of blood vessels and the bleeding usually stops very quickly.

11
Stomas have no nerve endings and therefore no feeling so it will not hurt when touched.
Dependent on the type of stoma, it can be located on different parts of the body. Dependent on the type of stoma, the output will be different. The stoma may sit out above or be slightly below the skin level.

12
The stoma may grow with your child, especially if it is permanent
The stoma may grow with your child, especially if it is permanent. It is important, therefore to re-measure the stoma from time to time to ensure that the pouch still fits correctly. At times when your child is crying you may notice a change in the colour of the stoma. However, the normal colour will return when the crying stops.

13
TYPES OF STOMA

14
There are 3 types of stoma and the type of stoma your child has will be determined by the reason for the surgery. Colostomy This is the most common stoma type for a baby or child. A colostomy is an opening made into the large intestine or colon. The stool can then pass from the stoma out of your child’s body which tends to be solid in consistency but can sometimes be liquid.

16
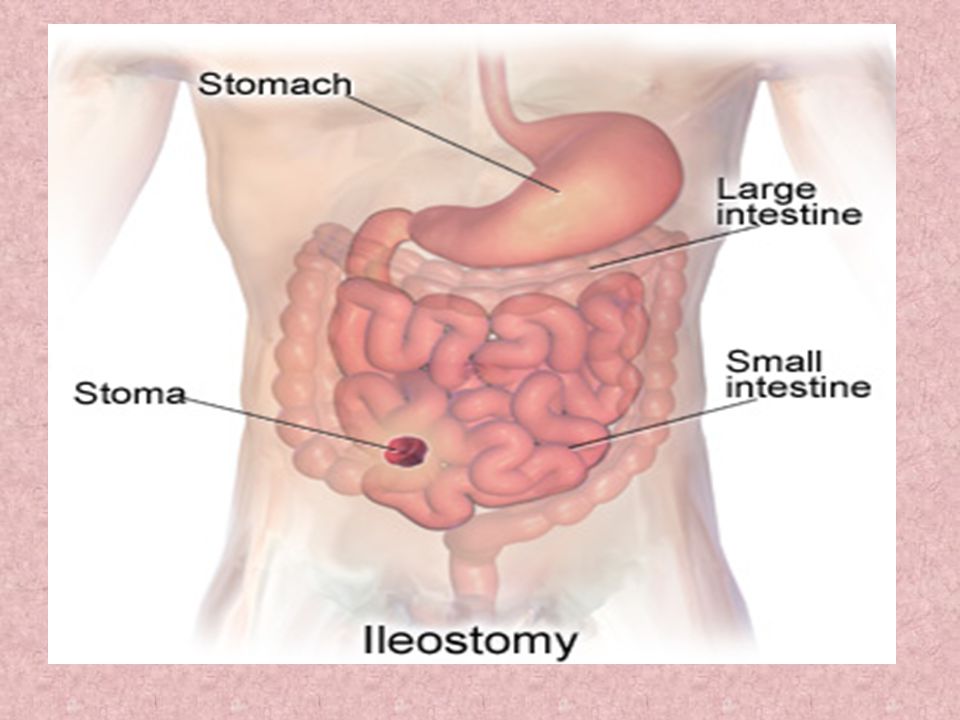
Ileostomy In an ileostomy the opening is made in the small intestine – the ileum. An end or loop of the small intestine is brought through the skin’s surface on your child’s abdomen and the output then passes out through the stoma. The ileostomy will resemble a ‘spout’ because the waste is more liquid. Due to the fact that ileostomy output contains digestive enzymes, this can be harmful to the skin and so requires extra care when pouching.

18
Urostomy A urostomy is an opening made to divert urine from the bladder and also resembles a ‘spout’ as the output is urine.

19
SELECTING YOUR CHILD’S APPLIANCES

20
Before leaving hospital with your child, your Stoma Care Nurse will be able to answer any queries that you may have. Be sure to ask them any questions that might be concerning you and also ensure that you are prepared for the pouch changing regime. You should have the opportunity to help the nurse out with pouch changes to build your own confidence.

21
A hypo-allergenic skin protector that is kind and gentle on young skin
A hypo-allergenic skin protector that is kind and gentle on young skin. This skin protector is also ultra-thin and moulds to create a secure fit. • A soft, skin-tone fabric that is cool and comfortable against the skin. The Pelican Pouch range all have teddy bear printed fabric with a split backing to allow easy viewing of the stoma without removing the pouch and enables easier pouch fitting. • A waterproof filter system to allow controlled deodorized airflow. • Where the waste is fairly runny (e.g. with an ileostomy or some colostomies) a drainable pouch should be used. Our range of Pelican Pouches with their Clip less Closure System ensures the pouch is very quick and easy to empty and clean.
 a drainable pouch should be used. Our range of Pelican Pouches with their Clip less Closure System ensures the pouch is very quick and easy to empty and clean.")
24
What types of products are used for colostomies?
Pouch: There are a variety of sizes and styles of colostomy pouches. Pouches are lightweight and odor-proof. Pouches have a special covering that prevents the pouch from sticking to the body. Some pouches also have charcoal filters which release gas slowly and help to decrease gas odor. The following is general information about types of colostomy pouches: Open-ended pouch: This type of pouch allows you to open the bottom of the pouch to drain the output. The open end is usually closed with a clamp. The open-ended pouch is usually used by people with ascending or transverse colostomies. The output from these colostomies is looser and is unpredictable (does not drain at regular times).
.")
25
Close-ended pouch: This type of pouch is removed and thrown away when the pouch is filled. Close-ended pouches are usually used by people with a descending or sigmoid colostomy. The output from these types of colostomies is firm and does not need to be drained . One-piece: A one-piece pouch contains the pouch and adhesive skin barrier together as one unit. The adhesive skin barrier is the part of the pouch system that is placed around the stoma and attached to skin. When the pouch is removed and replaced with a new one, the new pouch must be reattached to the skin.

26
Two-piece: The two-piece pouch has two parts: an adhesive flange and pouch. The adhesive flange stays in place while the pouch is removed and new pouch is attached to the flange. The pouch does not need to be reattached to the skin each time. The two-piece system can be helpful for patients with sensitive skin. Pre-cut or cut-to-fit pouches: Some pouches have pre-cut holes so you do not have to cut the opening yourself. Other pouches can be cut to fit the size and shape of your stoma. Cut-to-fit pouches are especially useful right after your surgery because your stoma decreases in size for about eight weeks.

27
Stoma covers and caps: Stoma caps or covers can be placed on the stoma when the stoma is not active (draining). People with descending or sigmoid colostomies who irrigate may use stoma covers or caps. The cover or cap is attached to the skin in the same way as a pouch. Skin protection: Film: A film can be placed on the skin to protect against damage from the adhesive material. Films are helpful for people with sensitive, dry, or oily skin. Pectin-based paste or paste strips/rings: These products are helpful for protecting skin against output that contains digestive enzymes (proteins that break down foods). Ascending or transverse colostomies can produce output that contains digestive enzymes, which can irritate or damage the skin. The paste is also used to create a flat pouch surface by filling in small skin creases
. Ascending or transverse colostomies can produce output that contains digestive enzymes, which can irritate or damage the skin. The paste is also used to create a flat pouch surface by filling in small skin creases.")
28
HOW TO CHANGE POUCH

29
The way in which you should change your colostomy pouch depends on the type of pouch you use. Your caregiver will give you specific instructions on how to change your colostomy pouch. The following is general information about how to change your pouch: Ask your caregiver about how often to change your colostomy pouch. The amount of time that you should leave your pouch on your abdomen depends on many things. The type of pouch you wear affects the amount of time you can wear a pouch. The kind and amount of stool you have also affects how long the pouch stays on. If you are wearing an open-ended pouch, empty the contents from pouch into the toilet. Gently remove the pouch by pushing the skin down and away from the adhesive skin barrier with one hand. With the other hand, pull the pouch up and away from the stoma.

30
Clean the skin around the stoma with warm water
Clean the skin around the stoma with warm water. You may also use soap but do not use soaps that have oil or perfumes. Pat your skin dry. Use a pouch that has an opening that is one-eighth of an inch larger than the stoma. Use skin protection products if you have irritated skin around the stoma. The skin can be treated with these products to protect your skin and create a dry surface. Center the pouch over the stoma and press it firmly into place on clean, dry skin. It may be helpful to hold your hand over the newly applied pouch for 30 seconds. The warmth of your hand can help to mold the adhesive skin barrier into place. Place the old pouch in another plastic bag to be thrown away if the pouch is disposable. If you use a reusable pouch, talk to your caregiver about how to clean the reusable pouch.

31
HOW TO EMPTY POUCH

32
Empty the pouch when it is one-third to one-half full
Empty the pouch when it is one-third to one-half full. Do not wait until the pouch is completely full because this could put pressure on the seal, causing a leak. The pouch may also detach, causing all of the pouch contents to spill. Place toilet paper into the toilet to reduce splash back and noise. Take the end of the pouch and hold it up. Remove the clamp (if the pouch has a clamp system).
.")
33
You may need to make a cuff at the end of the pouch to keep it from getting soiled.
Drain the pouch by squeezing the pouch contents into the toilet. Clean the cuffed end of the pouch with toilet paper or a moist paper towel. You may also rinse the pouch but it is not necessary. Make sure and keep the end of the pouch clean. Undo the cuff at the end of the pouch. Replace the clamp or close the end of the pouch according to your caregiver's instructions.

34
IRRIGATION

35
People with descending or sigmoid colostomies may be able to irrigate their colostomies on a regular basis. Irrigating the stoma means putting a fluid into the stoma to empty the bowel. This may also be called an enema. Irrigation allows a person to have timed bowel movements. Irrigation can allow a person to be free from stool output for about 24 to 48 hours. Once stool output is regular, a stoma cap can be used between irrigations instead of using a drainable pouch. The stoma cap will absorb mucus and deodorize and vent gas. Irrigation may be right for you if you had regular bowel movements before the colostomy. You should also be physically able to perform the irrigation procedure. It is also important to have a lifestyle that will allow regular irrigation. For example, you should have a daily schedule in which you can schedule enough time to regularly irrigate. You should also be free from certain colostomy problems. People with problems such as a prolapse or a hernia should not irrigate. Irrigation could make a prolapse worse or create a hole in the bowel. Irrigation could also cause leakage of stools between irrigations or make it hard to control bowel movements.

36
HOW TO IRRIGATE COLOSTOMY

37
You will need a plastic irrigating container with a long tube and a cone to introduce water into the colostomy. You will also need an irrigation sleeve that will direct the output into the toilet. You will need an adjustable belt to attach the irrigation sleeve and a tail closure for the end of the sleeve. Choose the same time each day when you will not be interrupted to irrigate your colostomy. Fill the irrigating container with about 16 to 50 ounces (500 to 1500 mL) of lukewarm water. The water should not be cold or hot. The amount of water each person needs to put in the irrigating container varies. Ask your caregiver how much water you will need to irrigate. Hang the irrigation container at a height in which the bottom of the container is level with your shoulder. Sit up straight on the toilet or on a chair next to the toilet.
 of lukewarm water. The water should not be cold or hot. The amount of water each person needs to put in the irrigating container varies. Ask your caregiver how much water you will need to irrigate. Hang the irrigation container at a height in which the bottom of the container is level with your shoulder. Sit up straight on the toilet or on a chair next to the toilet.")
39
Take the adjustable belt and attach it to the irrigation sleeve
Take the adjustable belt and attach it to the irrigation sleeve. Place the belt around your waist and place the sleeve over your stoma. Place the end of the irrigation sleeve into the toilet bowel. Release air bubbles from the tubing on the plastic irrigating container by releasing the clamp. Allow a small amount of water to be released into the sleeve. Clamp the tubing again. Moisten the end of the cone with water or lubricate it with water-soluble lubricant.

40
Place the tip of the cone about three inches deep into the stoma
Place the tip of the cone about three inches deep into the stoma. Make sure there is a snug fit but do not place the cone too deeply or forcefully into the stoma. Release the clamp on the tubing again and allow the water to flow into the stoma. The water must go in slowly and takes about five to ten minutes. Keep the cone in place for another 10 seconds. Remove the cone from the stoma. Allow the output to drain into the irrigation sleeve for about 10 to 15 minutes. Dry the end of the irrigation sleeve. Clip the bottom of the sleeve to the top with a clasp or close the end of the sleeve with the tail closure. You may move around for about 30 to 45 minutes until all the water and stool has drained. Drain the output from the sleeve into the toilet. Clean the area around the stoma with mild soap and water and pat dry

42
COMPLICATIONS

43
Most stoma problems happen during the first year after surgery.
Stoma retraction: Retraction happens when the height of the stoma goes down to the skin level or below the skin level. Retraction may happen soon after surgery because the colon does not become active soon enough. Retraction may also happen because of weight gain. The pouching system must be changed to match the change in stoma shape. Peristomal hernia: Peristomal hernias occur when part of the bowel (colon) bulges into the area around the stoma. Hernias are most obvious during times when there is pressure on the abdomen. For example, the hernia may be more obvious when sitting, coughing, or straining. Hernias may make it difficult to create a proper pouch seal or to irrigate. The hernia may be managed with a hernia belt. Changes may also need to be made to the pouching system to create a proper seal. Surgery may also be done in some people.
 bulges into the area around the stoma. Hernias are most obvious during times when there is pressure on the abdomen. For example, the hernia may be more obvious when sitting, coughing, or straining. Hernias may make it difficult to create a proper pouch seal or to irrigate. The hernia may be managed with a hernia belt. Changes may also need to be made to the pouching system to create a proper seal. Surgery may also be done in some people.")
44
Prolapse: A prolapse means the bowel becomes longer and protrudes out of the stoma and above the abdomen surface. The stomal prolapse may be caused by increased abdominal pressure. Surgery may be done to fix the prolapse in some people. Stenosis: A stenosis is a narrowing or tightening of the stoma at or below the skin level. The stenosis may be mild or severe. A mild stenosis can cause noise as stool and gas is passed. Severe stenosis can cause obstruction (blockage) of stool. If the stoma is mild, a caregiver may enlarge it by stretching it with his finger. If the stenosis is severe, surgery is usually needed.
 of stool. If the stoma is mild, a caregiver may enlarge it by stretching it with his finger. If the stenosis is severe, surgery is usually needed.")
Similar presentations