Download presentation
Presentation is loading. Please wait.

1
Nail Disorders: Clues to Systemic Disease
Lianne Beck, MD Assistant Professor Emory Family Medicine Nail Disorders: Clues to Systemic Disease

2
Nail Anatomy The nail plate is the hard keratin cover of the dorsal portion of the distal phalanx. The nail plate is generated by the nail matrix at the proximal portion of the nail bed (Figure 1). As the nail grows, the distal part of the matrix produces the deeper layers of the nail plate, while the proximal portion makes the superficial layers. This production is important, because a disruption of function in the proximal matrix (as may occur in patients with psoriasis) results in more superficial nail problems (e.g., pitting). A disruption of the distal matrix may cause problems with the deeper layers, resulting in ridging or splitting. A transient problem causing growth disturbance may lead to the formation of transverse lines across the nail plate, as in Mees’, Muehrcke’s, and Beau’s lines The nail is bound proximally by the eponychium (the skin just proximal to the cuticle), laterally by the nail folds, and distally by the distal nail fold (defined by the separation created by the anterior ligament between the distal nail bed and the nail plate; 3 different layers: The nail plate (the nail). This is the keratinized structure, which grows throughout life; The nail bed (ventral matrix, sterile matrix). This is the vascular bed that is responsible for nail growth and support. It lies protected between the lunula (the "half moon" seen through the nail) and the hyponychium (the posterior part of the nail bed epithelium); and The eponychium (cuticle). The epidermal layer between the proximal nail fold and the dorsal aspect of the nail plate.
. As the nail grows, the distal part of the matrix produces the deeper layers of the nail plate, while the proximal portion makes the superficial layers. This production is important, because a disruption of function in the proximal matrix (as may occur in patients with psoriasis) results in more superficial nail problems (e.g., pitting). A disruption of the distal matrix may cause problems with the deeper layers, resulting in ridging or splitting. A transient problem causing growth disturbance may lead to the formation of transverse lines across the nail plate, as in Mees’, Muehrcke’s, and Beau’s lines. The nail is bound proximally by the eponychium (the skin just proximal to the cuticle), laterally by the nail folds, and distally by the distal nail fold (defined by the separation created by the anterior ligament between the distal nail bed and the nail plate; 3 different layers: The nail plate (the nail). This is the keratinized structure, which grows throughout life; The nail bed (ventral matrix, sterile matrix). This is the vascular bed that is responsible for nail growth and support. It lies protected between the lunula (the half moon seen through the nail) and the hyponychium (the posterior part of the nail bed epithelium); and. The eponychium (cuticle). The epidermal layer between the proximal nail fold and the dorsal aspect of the nail plate.")
3
Nail Anatomy Fingernails grow 2 -3 mm a month or 0.1 – 0.15 mm a day
Toenails grow 1 mm a month Growth rate (about 6 months from cuticle to free edge). Time of events can be estimated from location
. Time of events can be estimated from location.")
4
Beau's lines

5
Nail Shape and Surface Beau's lines
Transverse depression across the nail plate Occurs when growth at the nail root (matrix) is interrupted by trauma OR any severe acute illness e.g. heart attack, measles, pneumonia, or fever. These lines emerge from under the nail folds weeks later, and allow us to estimate when the patient was sick. Transverse depression across the nail plate. • Etiology: Temporary cessation of nail growth in the matrix. •Cause: Trauma to the proximal nail fold. Nonspecific finding in systemic disease
 is interrupted by trauma OR any severe acute illness e.g. heart attack, measles, pneumonia, or fever. These lines emerge from under the nail folds weeks later, and allow us to estimate when the patient was sick. Transverse depression across the nail plate. • Etiology: Temporary cessation of nail. growth in the matrix. •Cause: Trauma to the proximal nail fold. Nonspecific finding in systemic disease.")
6
Thin Brittle Nails Repetitive trauma particularly with long nails, repetitive wetting and drying, detergents, harsh solvent Metabolic bone disease (nail thinness is correlated with osteopenia) Thyroid disorder, anemia Systemic amyloidosis (indicated by yellow waxy flaking) Severe malnutrition More common in women Nails that chip, peel, crack, or break easily - suggest a nutritional deficiency, lacking hydrochloric acid, protein or minerals. Brittle Nails • • Causes: Repetitive trauma particularly with long nails, repetitive wetting and drying, detergents, harsh solvents e.g. nail polish remover, and artificial nails. Check for anemia & thyroid problems • Not caused by low calcium • Diffusion constant of water of the nail is 100x that of the skin. • Clinical: Longitudinal & horizontal cracking of the nail plate & splitting of the free distal end (Hang Nail) • Tx: Avoid the causes. Moisturize the nails with petrolatum 3 to 4x qd & after washing. Keep nails cut short. Biotin 2.5 to 5 mg qd
 Thyroid disorder, anemia. Systemic amyloidosis (indicated by yellow waxy flaking) Severe malnutrition. More common in women. Nails that chip, peel, crack, or break easily - suggest a nutritional deficiency, lacking hydrochloric acid, protein or minerals. Brittle Nails. • • Causes: Repetitive trauma particularly with long. nails, repetitive wetting and drying, detergents, harsh solvents e.g. nail polish remover, and. artificial nails. Check for anemia & thyroid. problems. • Not caused by low calcium. • Diffusion constant of water of the nail is 100x that. of the skin. • Clinical: Longitudinal & horizontal cracking of the. nail plate & splitting of the free distal end. (Hang Nail) • Tx: Avoid the causes. Moisturize the nails. with petrolatum 3 to 4x qd & after washing. Keep nails cut short. Biotin 2.5 to 5 mg qd.")
7
Onychorrhexis

8
Onychorrhexis Presence of longitudinal striations or ridges
A sign of advanced age but it can also occur with the following: Rheumatoid arthritis Peripheral vascular disease Lichen planus Darier's disease (striations are red/white). Central ridges can be caused by iron , folic acid or protein deficiency.
. Central ridges can be caused by iron , folic acid or protein deficiency.")
9
Central Nail Canal (Median Nail Dystrophy)
Associated with severe arterial disease ("Heller's fir tree deformity" -- a central canal with a fir tree appearance -- may occur with peripheral artery disease Severe malnutrition Repetitive trauma

10
Nail Beading The beads seem to drip down the nail like wax.
Associated with endocrine conditions, including the following: Diabetes mellitus Thyroid disorders Addison's disease Vitamin B deficiency

11
Clubbing

12
Clubbing Thickening of the soft tissue beneath the proximal nail plate resulting in sponginess of the proximal plate and thickening in that area of the digit. Occurs in patients with neoplastic diseases, particularly those of the lung and pleura. Associated with other pulmonary diseases, including bronchiectasis, lung abscess, empyema, pulmonary fibrosis, and cystic fibrosis. Others: AVM or fistulas, celiac disease, cirrhosis, and inflammatory bowel disease, congenital heart disease and endocarditis Changes in the configuration of the capillaries in the proximal nail bed are responsible for some of the alterations that occur in patients with connective tissue disorders, while abnormalities in the periosteal vessels contribute to clubbing.2 Clubbing may result from megakaryocytes and platelet clumps that have escaped filtration in the pulmonary bed and have entered the systemic circulation. Platelets then may release platelet-derived growth factor at the nail bed, causing periosteal changes The finding of clubbing without an obvious associated disease should prompt a search for bronchogenic carcinoma or another occult reason for the finding.

13
Clubbing • The angle of the base of the nail is greater than the normal 160°. The proximal nail fold has a spongy feel. • Classification: Idiopathic, Congenital, & Acquired • Cause Acquired bilateral: Respiratory disease 80% Cardiovascular extrathoracic 10% Acquired unilateral: Lymphadenitis or a Vascular lesion in the extremity e.g. av fistula • When a single nail is involved consider trauma or a congenital cause

14
Nails affected by psoriasis can have small pinpoint pits or large yellowish separations of the nail plate called "oil spots." Pitting

15
Pitting Punctate depressions in the nail plate caused by defective layering of the superficial nail plate by the proximal nail matrix. Usually associated with psoriasis, affecting 10 to 50 % of patients Also caused by systemic diseases, including Reiter’s syndrome and other connective tissue disorders, sarcoidosis, pemphigus, alopecia areata, and incontinentia pigmenti. Any localized dermatitis (atopic or chemical dermatitis) that disrupts orderly growth in proximal nail fold also can cause pitting.
 that disrupts orderly growth in proximal nail fold also can cause pitting.")
16
Oil Spot Sign or Salmon Patch
80% of psoriatic arthritis patients have nail involvement. • Clinical Random large deep pits on the surface of the nail. Red brown discoloration of the nail bed (oil spot sign, salmon patch) Leukonychia, splinter hemorrhages, subungual hyperkeratosis, and/or onycholysis. May have complete crumbling of nail plate. Nail Psoriasis • Ddx: Tinea unguium Patients with negative cultures & no skin findings for psoriasis refer. • Tx: Refer. Topical class 1 steroids, calcipotriol ointment, fluorouracil solution, topical retinoid ( Tazarotene gel) and intralesional steroids, very painful. Pitting Oil Spot Sign or Salmon Patch
 Leukonychia, splinter hemorrhages, subungual hyperkeratosis, and/or onycholysis. May have complete crumbling of nail plate. Nail Psoriasis. • Ddx: Tinea unguium. Patients with negative cultures & no skin. findings for psoriasis refer. • Tx: Refer. Topical class 1 steroids, calcipotriol ointment, fluorouracil solution, topical retinoid ( Tazarotene gel) and. intralesional steroids, very painful. Pitting. Oil Spot Sign or Salmon Patch.")
17
Koilonychia

18
Koilonychia Transverse and longitudinal concavity of the nail, resulting in a “spoon-shaped” nail. Normal nail variant in infants, but corrects itself within the first few years of life. Causes by iron deficiency anemia, hemochromatosis, Raynaud’s disease, SLE, trauma, occupational exposure of the hands to petroleum-based solvents, nail-patella syndrome Nail-Patella Syndrome: autosomal-dominant condition that includes hypoplastic, easily dislocated patellas, renal and skeletal abnormalities, and glaucoma

19
Onycholysis

20
Onycholysis Lifting of the nail plate from the nail bed. Causes:
Trauma Psoriasis Drug reactions (tetracycline) Bacterial/fungal/viral infection Contact dermatitis from using nail hardeners Thyroid disease (“Plummer’s nails”) Iron deficiency anemia Syphilis Eczema Porphyria cutanea tarda Amyloidosis, connective tissue disorders
 Bacterial/fungal/viral infection. Contact dermatitis from using nail hardeners. Thyroid disease ( Plummer’s nails ) Iron deficiency anemia. Syphilis. Eczema. Porphyria cutanea tarda. Amyloidosis, connective tissue disorders.")
21
Onycholysis

22
Nail hypertrophy Causes Onychomycosis Chronic eczema
Peripheral vascular disease Yellow nail syndrome Psoriasis Not cutting the nails, trauma Slow nail growth produces thickness

23
Onychomycosis • Treatment
Terbinafine ( Lamisil) 250mg po qd 6 wks for fingernails and 3mos for toenails. If one or two nails are thick and • Treatment symptomatic may surgically or chemically avulse ( 40% urea) Ciclopirox lacquer (Penlac) Topical medthat can be used for patients who cannot take oral meds. Mycologic cure rate 29% to 36% Distal Lateral Subungual Infection • Terbinafine well tolerated. Occasional GI upsets. • Rare hepatotoxicity so cannot be used in pts with history of liver disease. Check baseline LFTs and repeat in 4 to 6weeks or if clinically indicated. • Drug interactions not as common as azoles. • Cost: Walmart $4 for 30 pills, $10 for 90! Drug Interactions With Terbinafine Contraindicated with: Patients hypersensitive to terbinafine or to any other ingredients of the formulation Inhibits the CYP2D6 isoenzyme. May affect metabolism of Tricyclics, Serotonin reuptake inhibitors, beta- blockers & monoamine oxidase inhibitors May increase or decrease prothrombin times in patients concomitantly taking terbinafine and warfarin Decrease plasma concentration of terbinafine -Terbinafine clearance is increased 100% by rifampin Increase plasma concentration of terbinafine -Terbinafine clearance is decreased 33% by cimetidine Drug plasma concentration increased by terbinafine -Decreases caffeine clearance by 19% -Decreases theophylline clearance by 14% Drug plasma concentration decreased by terbinafine -Increases clearance of cyclosporine by 15% 40% urea Chemical Avulsion Regrowing New Nail Onychomycosis
 250mg po qd 6 wks for fingernails and 3mos for toenails. If one or two nails are thick and. • Treatment. symptomatic may surgically or chemically avulse ( 40% urea) Ciclopirox lacquer (Penlac) Topical medthat can be used for patients who cannot take oral meds. Mycologic cure rate 29% to 36% Distal Lateral Subungual Infection. • Terbinafine well tolerated. Occasional GI upsets. • Rare hepatotoxicity so cannot be used in pts. with history of liver disease. Check baseline LFTs and repeat in 4 to 6weeks or if clinically indicated. • Drug interactions not as common as azoles. • Cost: Walmart $4 for 30 pills, $10 for 90! Drug Interactions With Terbinafine. Contraindicated with: Patients hypersensitive to terbinafine or to any other ingredients of the formulation. Inhibits the CYP2D6 isoenzyme. May affect metabolism of Tricyclics, Serotonin reuptake inhibitors, beta- blockers & monoamine oxidase inhibitors May increase or decrease prothrombin times in patients. concomitantly taking terbinafine and warfarin Decrease plasma concentration of terbinafine. -Terbinafine clearance is increased 100% by rifampin. Increase plasma concentration of terbinafine. -Terbinafine clearance is decreased 33% by cimetidine. Drug plasma concentration increased by terbinafine. -Decreases caffeine clearance by 19% -Decreases theophylline clearance by 14% Drug plasma concentration decreased by terbinafine. -Increases clearance of cyclosporine by 15% 40% urea. Chemical Avulsion Regrowing New Nail. Onychomycosis.")
24
Onychomycosis Trichophyton Rubrum most common dermatophyte
Toenails more commonly affected than fingernails and often associated with tinea pedis Causes Age, M>F, immunosuppression, HIV, DM, chronic trauma, PVD, hyperhydrosis Uncommon in children

25
Reasons for Relapse 23% relapse rate w/ terbinafine
Old age and slow nail growth Immunosuppression Reinfection from surrounding skin Preventing Relapse Avoid barefeet in public places Keep feet dry Apply antifungal cream to feet weekly Apply antifungal powder or spray to shoes weekly Discard old shoes

26
Nail atrophy The nail becomes thin, rudimentary and smaller size congenital or acquired. Causes: Lichen planus Epidermolysis bullosa Darier‘s disease Vascular disturbances Leprosy Darier's is characterized by dark crusty patches on the skin, sometimes containing pus. The crusty patches are also known as keratotic papules, keratosis follicularis or dyskeratosis follicularis.[4]

27
Pigmentation Abnormalities
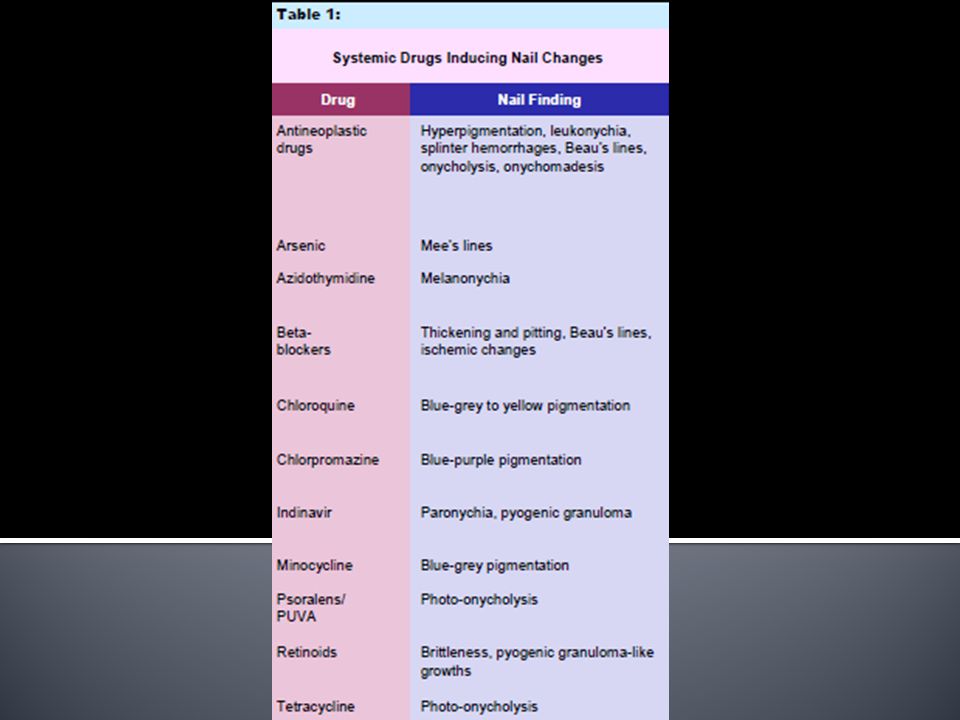
Categories Derm conditions: Psoriasis oil spot Systemic drugs or ingestants: AZT, Minocin, Chemotherapy drugs Systemic Disease: Mees Lines (Leukonychia) Local agents: Cosmetics, physical agents
 Local agents: Cosmetics, physical agents.")
28
Diagnostic Pearls If the discoloration follows the shape of the lunula and effects multiple nails think of a systemic cause. If the discoloration corresponds to the shape of the proximal nail fold and effects only a few nails think of an external cause. If scraping the nail surface or using acetone removes the color then the cause is a topical substance.

29
Abnormalities of the Lunula
If the lunula is absent, consider anemia or malnutrition A pyramidal lunula might indicate excessive manicure or trauma A pale blue lunula suggests diabetes mellitus If the lunula has red discoloration, consider the following causes among others: cardiovascular disease; collagen vascular disease; and hematologic malignancy.

31
Argyria Argyria occurs in people who ingest or inhale silver in large quantities over a long period (several months to many years). Stan Jones of Montana, a Libertarian candidate for the United States Senate in 2002 and Jones acquired argyria through consumption of a home-made silver product that he made due to fears that the Year 2000 problem would make antibiotics unavailable

34
Leukonychia (White Nails)
Originates in matrix and involves nail plate Causes Trauma Systemic disease Drugs Heredity Sporadic Can be total, subtotal or partial (punctate or transverse)
")
35
Mee's lines

36
Mee's lines Transverse type of true leukonychia caused by systemic disease. Clinical: Single or multiple transverse lines that involve multiple nails. The pigment is in the nail plate. Causes: Arsenic poisoning, Hodgkin’s disease, CHF, leprosy, malaria, chemotherapy, carbon monoxide poisoning, other systemic insults

37
Leukonychia Striae caused by trauma to the matrix from aggressive manicuring, involves only a few nails & does not extend across the entire nail plate.

38
Muehrcke's Lines

39
Muehrcke's Lines Confined to the nail bed. Will disappear when distal digit is squeezed. Clinical: Double white transverse lines affecting numerous nails. Causes: Chemotherapy and Hypoalbuminemia secondary to nephrotic syndrome, liver disease, or glomerulonephritis.

40
Terry’s Nails

41
Terry's Nails Clinical: Proximal white nail with narrow distal pink or brown band (0.5 to 3mm) The nail looks opaque and white, but the nail tip has a dark pink to brown band. Causes: cirrhosis, CHF, DM, cancer, hyperthyroidism, malnutrition, ageing

42
Half and Half Nails

43
Half and Half Nails Clinical: Proximal half of nail plate is white & distal half is red brown. Cause: Present in 9 to 15 % of chronic renal failure patients. (Lindsay's nails) — Look for an arc of brownish discoloration.
 — Look for an arc of brownish discoloration.")
44
Splinter Hemorrhages

45
Splinter Hemorrhages Longitudinal hemorrhagic streaks involving the nail bed. Causes: Trauma (most common), Derm disease (psoriasis), Idiopathic, and Systemic disease (subacute bacterial endocarditis ) Diagnostic Pearls If multiple nails are involved simultaneously and they occur near the lunula think of systemic disease. If one or a few nails are involved and they occur near the end of the nail plate think of trauma Looks like a splinter underneath the nail, virtually 100% diagnostic of Sub-acute Bacterial Endocarditis (SBE). Occasionally caused by Trichinosis, a parasitic infection caused by eating raw or undercooked Pork.
, Derm disease (psoriasis), Idiopathic, and Systemic disease (subacute bacterial endocarditis ) Diagnostic Pearls. If multiple nails are involved simultaneously and they occur near the lunula think of systemic disease. If one or a few nails are involved and they occur near the end of the nail plate think of trauma. Looks like a splinter underneath the nail, virtually 100% diagnostic of Sub-acute Bacterial Endocarditis (SBE). Occasionally caused by Trichinosis, a parasitic infection caused by eating raw or undercooked Pork.")
47
White Nails Causes: Anemia Renal failure Cirrhosis Diabetes mellitus
Chemotherapy Hereditary (rare).
.")
48
Pink or Red Nails Causes: Polycythemia (dark)
Systemic lupus erythematosus Carbon monoxide (cherry red) Angioma Malnutrition
 Angioma. Malnutrition.")
49
Brown-Gray Nails Causes: Cardiovascular disease Diabetes mellitus
Vitamin B12 deficiency Breast cancer Malignant melanoma Lichen planus Syphilis Topical agents, including hair dyes, solvents for false nails, varnish, and formaldehyde (among many others)
")
50
Yellow Nails Diabetes mellitus Amyloidosis Median/ulnar nerve injury
Thermal injury Jaundice

51
Yellow Nail Syndrome Arrest in nail growth with yellow or green nails, absence of cuticle, thick nail plate. Usually all nails affected Can indicate internal disorders long before other symptoms appear. Associated with pulmonary disease (COPD, TB, asthma, chronic bronchitis), chronic lymphedema, and thyroid disease, diabetes, liver disorders. Consider yellow nail syndrome if a patient has lymphedema and bronchiectasis
, chronic lymphedema, and thyroid disease, diabetes, liver disorders. Consider yellow nail syndrome if a patient has lymphedema and bronchiectasis.")
52
Green or Black Nails Causes:
Topical preparations, including chlorophyll derivations, methyl green, and silver nitrate (among others) Chronic Pseudomonas spp infection Trauma
 Chronic Pseudomonas spp infection. Trauma.")
53
Melanonychia

54
Melanonychia Longitudinal Pigmented Bands (LPB)
Cause: Pigmented band appearing in the distal matrix and extending to the tip of the nail. Clinical: Tan, brown or black longitudinal streaks within the nail plate. May be single or multiple bands. Causes: Melanocytic activation No increase in melanocyte number Responsible for 73% of single LPB in adults. Melanocytic hyperplasia Increase in melanocyte number Responsible for 77% of single LPB in children

55
Melanonychia Common in darkly pigmented persons
African Americans: 77% by age 20, 100% by age 50 Asian: 10-20% Hispanic, Indian common Unusual in Caucasians Thumb & index finger most commonly affected

56
Causes of Longitudinal Melanonychia
Melanocyte activation Racial, pregnancy Trauma, post inflammatory (lichen plannus, pustular psoriasis, onychomycosis, chronic radiodermatitis) Drugs (doxyrubicin, 5-FU, AZT, psoralens) Laugler-Hunziker/Putz Jeger Syndromes Addison’s Disease HIV
 Drugs (doxyrubicin, 5-FU, AZT, psoralens) Laugler-Hunziker/Putz Jeger Syndromes. Addison’s Disease. HIV.")
57
Causes of Longitudinal Melanonychia
Non-melanocytic tumors (Bowen’s Disease, Verrucae, Basal cell carcinoma, Subungual keratosis, Myxoid cyst) Melanocyte hyperplasia Nail matrix nevus Nail matrix melanoma
 Melanocyte hyperplasia. Nail matrix nevus. Nail matrix melanoma.")
58
Subungual Melanoma

59
Subungual Melanoma Rare in caucasians 1 to 4% of all melanomas
African Americans 25% Asians 17 to 23% Peak age 50 to 80 but can occur at any age Rare in children LPB is first sign in 38 to 76 % of nail melanoma 45-60% on hand 40%-55% on foot Thumb, index finger, great toe most common sites

60
Be Suspicious of Melanoma if LPB:
Develops in a single digit in adult life especially in 6th decade or later Develops abruptly in previously normal nail Becomes suddenly darker or wider Preceding history of digital trauma

61
Subungual Melanoma Occurs as a single band in the thumb, index finger or great toe in a dark skinned patient Demonstrates blurred lateral margin Occurs in a patient with a personal history of melanoma Occurs in a patient with a family history of melanoma Presence of partial or complete nail dystrophy

62
Modified ABCDEF Rule Age: Peak incidence 5th to 7th decade
Band: Brown – black band, Breadth > 3mm, Border irregular/ blurred Change: Rapid change in growth and/or color or lack of change: Failure of nail dystrophy to improve with adequate treatment Digit involved: Thumb > great toe > index finger, Single > multiple digits, Dominant hand Extension: Of pigment to proximal or lateral nail fold Family or personal history: Previous melanoma or dysplastic nevus syndrome

63
pigmentation of periungual tissues

65
Presenting Signs of Subungual Melanoma
Mass below nail with partial or complete nail destruction - 50% Periungual infection/ulceration of nail bed/granulation tissue - 33% Discoloration of nail area - 33% Amelanotic - 25% Some begin as LPB: 38% -76% Hutchinson's sign less frequent Frequent delay in diagnosis: Mistaken for traumatic, infected, or inflamed lesion

66
Subungual Melanoma Most patients present with late disease
5 year survival % 25% nodal spread

67
Amelanotic Melanoma 25% of nail melanomas Misdiagnoses
Pyogenic granuloma Chronic granulation tissue Paronychia

69
Subungual Hematoma

70
Subungual Hematoma Acute lesions are red and painful
Older lesions are purple or black and nontender DDx: Melanoma is a concern especially in an older patient A pigmented lesion will persist as the nail grows Hemorrhage will be replaced proximally by a normal nail plate as the nail grows Melanomas can produce hemorrhage Biopsy if unsure or concerned Tx: If painful, decompress an acute lesion

71
Mucous or Myxoid Cyst

72
Mucous or Myxoid Cyst Smooth flesh colored semi-translucent nodule between the DIP joint & proximal nail fold Contains a viscous clear fluid Exerts pressure on the matrix resulting in a longitudinal groove Usually associated with osteoarthritis & may connect with the joint space TX: A cyst that does not connect with the joint space, I&D and intralesional steroids or cryotherapy A cyst that connects with joint space may require surgical removal

73
Pyogenic Granuloma

74
Pyogenic Granuloma Clinical: Over growth of vascular tissue involving the paronychia. Bleeds easily. Causes: Trauma, infection, ingrown nail Tx: Biopsy to rule out amelanotic melanoma Treat underlying cause

75
Bowens Disease Squamous Cell Carcinoma in Situ
Common in males on the fingernails. Causes: UV light, HPV, chronic infection, trauma, X ray exposure. Clinical: Long standing scaly or wart like growth involving the lateral nail fold. May see onycholysis & nail plate deformity. Biopsy all recalcitrant warts in older patients. Tx: Mohs micrographic surgery.

77
Autoimmune and Arthritic Diseases
All have nail findings that for the most part are nonspecific. Periungual erythema and telangiectasias are specific & can be an early finding that may help make the diagnosis in difficult cases.

79
Eczema Causes: Atopic dermatitis, dyshidrotic eczema, irritant or contact dermatitis e.g. acrylates in sculptured nails. Clinical: Paronychium -Acute or chronic paronychia, Beau's lines, and pits. Hyponychium -Subungual hyperkeratosis onycolysis & finger tip scaling. Tx: Remove cause & medium strength topical steroids.

81
Acute Paronychia Inflammation of the nail folds, which appear red, swollen and tender. Non bacterial causes: contact irritant dermatitis, dyshidrotic eczema, & drugs, fungal Acute bacterial paronychia most common infection of the hand. (Staph, strep & pseudomonas) Caused by aggressive manicuring or nail biting Tx: I&D when necessary and culture when possible Antistaphylococcal antibiotic for 7 to 10 days. For unresponsive cases r/oosteomyelitis and Bx to r/o malignancy.
 Caused by aggressive manicuring or nail biting. Tx: I&D when necessary and culture when possible. Antistaphylococcal antibiotic for 7 to 10 days. For unresponsive cases r/oosteomyelitis and Bx to r/o malignancy.")
83
Simple Chronic Paronychia
Inflammation involving the nail folds lasting > 6 wks. Causes: Aggressive manicuring, chronic exposure to water, contact irritants, & in children finger sucking Bakers, bartenders, waitresses, food handlers, maids, mothers with children Candida & bacteria are secondarily present Chronic swelling of the nail folds & loss of the cuticle Tx: Eliminate cause & minimize water contact. Mid or high potency topical steroids & ciclopirox ( Loprox suspension).
.")
84
Due to Candida

88
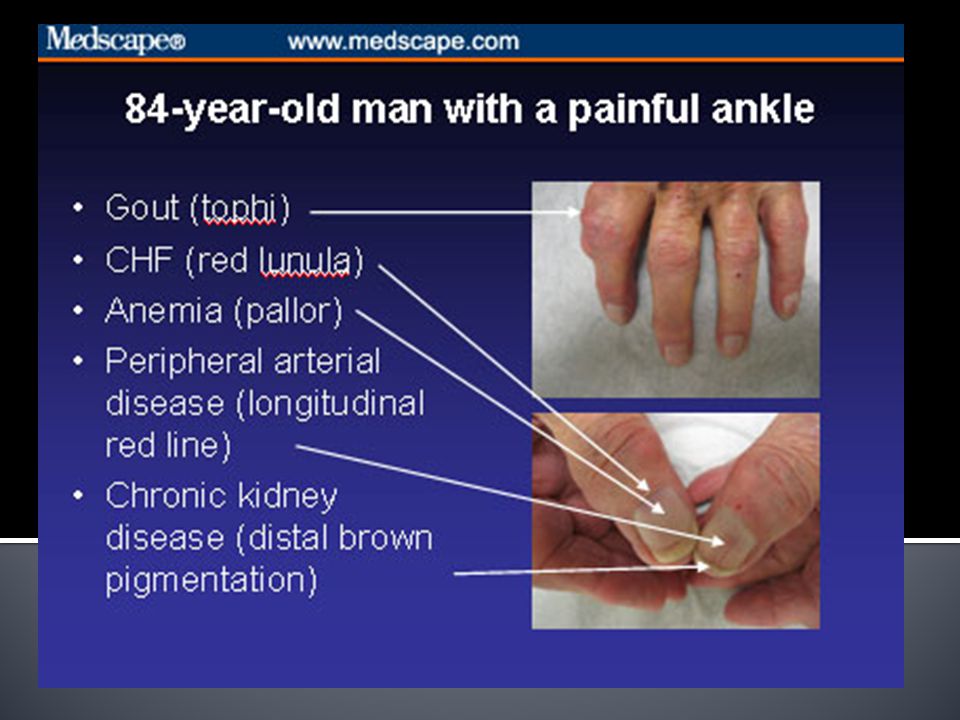
References Fawcett L, Linford S. Nail Abnormalities: Clues to Systemic Disease. American Family Physician. March 15, 2004. Williams M. Examining the Fingernails When Evaluating Presenting Symptoms in Elderly Patients. Medscape. 11/23/2009.

Similar presentations