Download presentation
Presentation is loading. Please wait.

1
Lymphadenopathy M.JARI.MD.

2
Objectives Define lymphadenopathy Develop a systematic approach to the evaluation and management of lymphadenopathy Discuss the differential diagnosis of localize and generalized lymphadenopathy

3
Lymphatic System

4
Lymphtic system Lymph nodes Lymphatic Vessels Spleen Thymus Adenoid Tonsils

5
Lymphatic capillaries: L.capillaries are in all organs except : Brain Heart Epiderm Nails

6
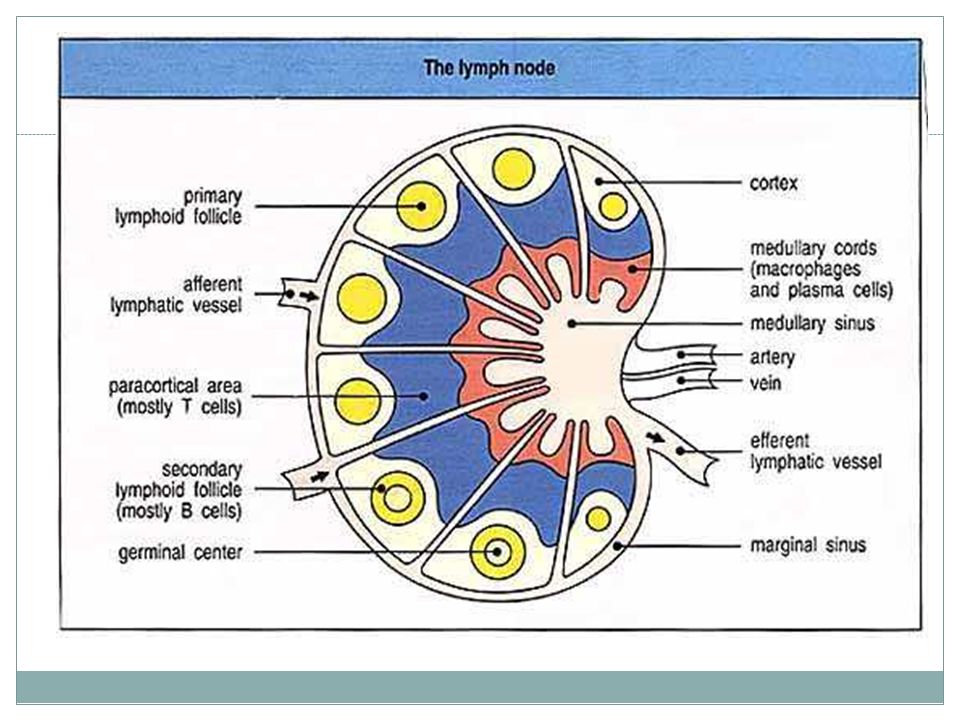
Physiology & Anatomy Lymph nodes are populated by: dendritic cells, B and T lymphocytes,macrophage B Lymphocytes T Lymphocytes

8
Approach to Patient Lymphadenopathy – refers to lymph nodes that are abnormal in size, number or consistency Consider: Age of Patient Size of Nodes Location of Nodes Quality of Nodes Localized or generalized Time course of the lymphadenopathy

9
Size of Lymph Nodes Rules of thumb: Axillary and cervical nodes < 1 cm Inguinal <1.5 cm Epitrochlear <0.5 cm Nodes tend to be larger in young children Odds of malignancy is higher in larger nodes especially those > 2 cm

10
Location of Lymph Nodes Node Groups Occipital Postauriclular Preauricular Parotid Submandibular Submental Superficial cervical Deep cervical Supraclavicular Deltopectoral Axillary Epitrochlear Inguinal Popliteal Region Drained Posterior Scalp Temporal & parietal scalp Scalp, ear canal, conjunctiva Scalp, midface, ear canal and ear, parotid Cheek, nose, lips, tongue, subman. gland Lower lip, floor of mouth Lower larynx, lower ear canal, parotid Tonsils, adenoids, scalp, larynx, sinuses Mediastinum, lungs, abdomen Arm Arm, breast, thorax, neck Medial arm below elbow Lower extremities, genitalia, abdomen Lower leg

11
Quality of Lymph Nodes Painful Usually infection, especially if erythema, warmth, or fluctance Malignancy can cause node tenderness because of hemorrhage into node and stretching of capsule Hard Found in cancers because of fibrosis Nonmobile Become fixed from invasive cancers of inflammation in tissue surrounding nodes (ie TB or sarcoidosis) SOFT, COMPRESSIBLE = NORMAL
 SOFT, COMPRESSIBLE = NORMAL")
12
Localized Lymphadenopathy

13
Differential Diagnosis - Infection Bacterial Localized: Staph aureus, GAS, cat-scratch, tularemia, diphtheria Generalized : Brucellosis, leptospirosis, typhoid Viral EBV, CMV, HSV, HIV, Hep B, Measles, Mumps, Rubella, Dengue Fever Myocobacterial TB, Atypical mycobacteria Fungal Coccidiomycosis, Cryptococcosis, Histoplasmosis Protozoal Toxoplamosis, Leishmaniasis Spirochetal Lyme disease, symphilis

14
Differential Diagnosis - Other Malignancy leukemia, lymphoma, metastasis from solid tumor Immunologic SLE, serum sickness, Langerhans cell histiocytosis, RA, Drug Reaction, dermatomyositis, CGD Endocrine Addison disease, hypothyroidism Other Amyloidosis, Kawasaki disease, Sarcoidosis, Churg-Strauss syndrome, Kikuchi disease, Castleman disease

15
Time Course of Lymphadenopathy When to biopsy Many advocate biopsy of concerning nodes that have not decreased after 4-6 weeks or have not normalized in 8-12 weeks Lymph nodes present for long time are not likely to be malignant except for Hodgkins Exposure medications, animals, uncooked meats, unpasteurized milk Associated constitutional symptoms Fever, night sweats, weight loss, pruritus, arthralgias, fatigue

16
Lymphadenitis Lymphadenitis – enlarged, inflamed, tender lymph nodes Organisms: Staph aureus, GAS (80%) Usually submandibular Southwest US Yersinia pestis = Bubonic plague Bartonella henselae = cat scratch TB and atypical mycobacteria (M. avium and M. scrofulaceum) Management Culture drainage or of pharyngeal exudate Treatment 1 st /2 nd generation cephalosporin or dicloxacillin Clindamycin or Augmentin if anaerobe suspected (oral) Ultrasound to determine if abscess I&D indicated if abscess present
 Management Culture drainage or of pharyngeal exudate Treatment 1 st /2 nd generation cephalosporin or dicloxacillin Clindamycin or Augmentin if anaerobe suspected (oral) Ultrasound to determine if abscess I&D indicated if abscess present.")
17
Diagnostic Testing to Consider Blood CBC, ESR, LDH Specific Serologic testing (EBV, CMV, Bartonella) Tuberculin Skin Testing Chest X-ray Biopsy
 Tuberculin Skin Testing Chest X-ray Biopsy")
Similar presentations





One-way drainage system. 2) Lipid Absorption from Small Intestine. 3) Produce & circulates Immune.>")








 Spleen Thymus Thoracic duct Lymphatic vessels Palatine tonsil Bone marrow Lymph nodes Functions of the lymph system 1.Fluid recovery.>")


One-way drainage system 2) Lipid Absorption from Small Intestine 3) Produce & circulates Immune.>")
![Lymphatic System. Functions of the Lymphatic System Fluid Balance - returns interstitial fluid to the blood Fat [and fat soluble vitamins] Absorption.](/16/5226115/big_thumb.jpg "Lymphatic System. Functions of the Lymphatic System Fluid Balance - returns interstitial fluid to the blood Fat [and fat soluble vitamins] Absorption.>")
