Download presentation
Presentation is loading. Please wait.

1
In the Name of God

2
Dr. Mirdamadi Cardiologist,Fellowship of Echocardiography
Pericardial disease Dr. Mirdamadi Cardiologist,Fellowship of Echocardiography

3
Pericardium The normal pericardium is a double-layered sac
the visceral and parietal pericardium that is separated by a small quantity (15–50 cc) of fluid.
 of fluid.")
4
pericardial functions
1. Prevents sudden dilation of the cardiac chambers, especially the right atrium and ventricle, during exercise and with hypervolemia. 2.Restricts the anatomic position of the heart 3.Minimizes friction between the heart and surrounding structures 4. Prevents displacement of the heart and kinking of the great vessels 5. Retards the spread of infections from the lungs and pleural cavities to the heart.

5
Acute Pericarditis

6
Clinical Classification
I. Acute pericarditis (<6 weeks) A. Fibrinous B. Effusive (serous or sanguineous) II. Subacute pericarditis (6 weeks to 6 months) A. Effusive-constrictive B. Constrictive III. Chronic pericarditis (>6 months) A. Constrictive B. Effusive C. Adhesive (nonconstrictive)
 A. Fibrinous B. Effusive (serous or sanguineous) II. Subacute pericarditis (6 weeks to 6 months) A. Effusive-constrictive B. Constrictive III. Chronic pericarditis (>6 months) A. Constrictive B. Effusive C. Adhesive (nonconstrictive)")
7
Etiologic Classification
I. Infectious pericarditis A. Viral (coxsackievirus A and B, echovirus, mumps, adenovirus, hepatitis, HIV) B. Pyogenic (pneumococcus, streptococcus, staphylococcus, Neisseria, Legionella) C. Tuberculous D. Fungal (histoplasmosis, coccidioidomycosis, Candida, blastomycosis) E. Other infections (syphilitic, protozoal, parasitic)
 B. Pyogenic (pneumococcus, streptococcus, staphylococcus, Neisseria, Legionella) C. Tuberculous. D. Fungal (histoplasmosis, coccidioidomycosis, Candida, blastomycosis) E. Other infections (syphilitic, protozoal, parasitic)")
8
II. Noninfectious pericarditis
A. Acute myocardial infarction B. Uremia C. Neoplasia 1. Primary tumors (benign or malignant, mesothelioma) 2. Tumors metastatic to pericardium (lung and breast cancer, lymphoma, leukemia) D. Myxedema E. Cholesterol F. Chylopericardium
 2. Tumors metastatic to pericardium. (lung and breast cancer, lymphoma, leukemia) D. Myxedema. E. Cholesterol. F. Chylopericardium.")
9
G. Trauma 1. Penetrating chest wall 2. Nonpenetrating H
G. Trauma 1. Penetrating chest wall 2. Nonpenetrating H. Aortic dissection (with leakage into pericardial sac) I. Postirradiation J. Familial Mediterranean fever K. Familial pericarditis L. Acute idiopathic M. Whipple's disease N. Sarcoidosis
 I. Postirradiation J. Familial Mediterranean fever K. Familial pericarditis L. Acute idiopathic M. Whipple s disease N. Sarcoidosis")
10
III. Pericarditis related to hypersensitivity or autoimmunity
A. Rheumatic fever B. Collagen vascular disease C. Drug-induced D. Post-cardiac injury 1. Postmyocardial infarction (Dressler's syn.) 2. Postpericardiotomy 3. Posttraumatic
 2. Postpericardiotomy. 3. Posttraumatic.")
11
Definition Acute Pericarditis defined as symptoms or signs resulting from pericardial inflammation of no more than 1-2 weeks The majority of causes is idiopathic Most cases of acute idiopathic pericarditis are viral but testing for specific virus is not routine

12
Acute pericarditis almost always presents with chest pain
The pain can be severe. It is almost always pleuritic. It is not similar to myocardial ischemia. Pericardial pain typically has a relatively rapid onset It is most commonly substernal but can be centered in the left anterior chest or epigastrium. Left arm radiation is not unusual. The radiation is to the trapezius ridge, which is highly specific for pericarditis. Pericardial pain is relieved by sitting forward and worsened by lying down.

13
Associated symptoms : dyspnea, cough, and hiccoughs.
history of symptoms suggesting a viral syndrome is common. It is important to review the past medical history for clues to specific diagnoses. A history of cancer or an autoimmune disorder, high fevers with shaking chills, rash, or weight loss should alert the physician to specific diseases that can cause pericarditis.

14
Differential Diagnosis
pneumonia or pneumonitis with pleurisy (which may coexist with pericarditis), pulmonary embolus or infarction, costochondritis, gastroesophageal reflux disease. myocardial ischemia or infarction aortic dissection intraabdominal processes pneumothorax herpes zoster pain before skin lesions appear. Acute pericarditis due to recent silent MI.
, pulmonary embolus or infarction, costochondritis, gastroesophageal reflux disease. myocardial ischemia or infarction. aortic dissection. intraabdominal processes. pneumothorax. herpes zoster pain before skin lesions appear. Acute pericarditis due to recent silent MI.")
15
Physical Examination Patient is uncomfortable and anxious and may have low grade fever and sinus tachycardia. The only abnormal physical finding is the friction rub caused by contact between visceral and parietal pericardium. It consists of three components corresponding to ventricular systole, early diastolic filling, and atrial contraction . The rub is usually loudest at the LSB and is best heard with the patient leaning forward.

16
It is often dynamic, disappearing and returning during short periods.
Thus, it is often rewarding to listen frequently to a patient with suspected pericarditis who does not have an audible rub initially.

17
Laboratory Testing

18
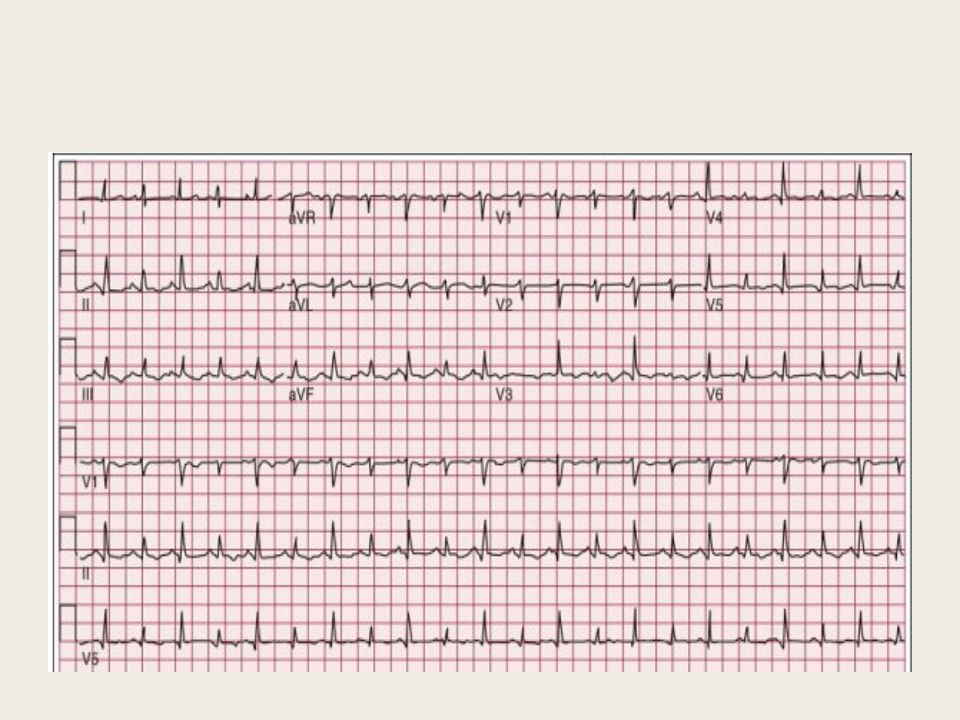
Electrocardiography ST-segment elevation in all leads except aVR and often V1. The ST segment is usually coved upward and resembles the hyper acute MI(differentiation with more extensive lead involvement in pericarditis and the presence of reciprocal ST depression in ischemia.) However, ST elevation in pericarditis sometimes involves a smaller number of leads Somtimes, the ST segment is similar to early repolarization. Here again, pericarditis usually involves more leads than typical early repolarization
 However, ST elevation in pericarditis sometimes involves a smaller number of leads. Somtimes, the ST segment is similar to early repolarization. Here again, pericarditis usually involves more leads than typical early repolarization.")
19
As with the rub, electrocardiographic changes can be dynamic.

20
PR segment depression is also common .
PR depression can occur without ST elevation and be the initial or sole ECG manifestation of acute pericarditis.

21
In some, the ECG reverts to normal during days or weeks.
In others, the elevated ST segment progresses to ST-segment depression and T wave inversions in leads with upright QRS complexes. These changes can persist for weeks or even months .

22
In patients presenting late after the onset of symptoms, these findings can be difficult to distinguish from ischemia

24
Laboratory Data Modest elevations of the white blood cell count with mild lymphocytosis Elevated creatine kinase MB fraction or troponin I values Serum ANA evaluation in young woman is recommended.

25
The CXR is usually normal in uncomplicated acute idiopathic pericarditis but pulmonary disease,TB,malignancy or pericardial effusion may be detected by CXR

26
Echocardiography Echo is normal in the most patients .
The main reason for it is to exclude silent effusion. Most patients do not have effusions, but small ones are fairly common . Moderate or larger effusions are unusual and may signal a diagnosis other than idiopathic pericarditis. Echo is also useful to rule out associated myocarditis.

27
Treatment Acute idiopathic pericarditis is a self-limited disease without significant complications or recurrence in 70% to 90% of patients.

28
Treatment with NSAIDs should be initiated
Ibuprofen (600 to 800 mg orally three times daily) with discontinuation if pain is no longer present after 2 weeks.
 with discontinuation if pain is no longer present after 2 weeks.")
29
Patients who respond slowly or inadequately to NSAIDs may require supplementary narcotic analgesics to allow time for a full response or a course of colchicine. Colchicine is administered as a 2- to 3-mg oral loading dose followed by 1 mg daily for 10 to 14 days

30
Poorly responding patients have typically been treated with short courses of corticosteroids.
However, corticosteroids should be avoided as they appear to encourage recurrences. Prednisone 60 mg orally daily for 2 days with tapering to zero during a week.

32
Cardiac Tamponade

33
The accumulation of fluid in the pericardial space in a quantity sufficient to cause serious obstruction to the inflow of blood to the ventricles results in cardiac tamponade. This complication may be fatal if it is not recognized and treated promptly.

34
The most common causes of tamponade :
neoplastic disease idiopathic pericarditis renal failure. Tamponade may also result from bleeding into the pericardial space after cardiac operations, trauma, and treatment of patients with acute pericarditis with anticoagulants.

35
The three principal features of tamponade (Beck's triad) :
Hypotension Soft or absent heart sounds Jugular venous distention with a prominent x descent but an absent y descent

36
The quantity of fluid necessary to produce tamponae may be as small as 200 mL when the fluid develops rapidly or >2000 mL in slowly developing effusions . Tamponade may also develop more slowly, and in these circumstances the clinical manifestations may resemble those of heart failure, including dyspnea, orthopnea, and hepatic engorgement

37
Paradoxical Pulse

38
presence of cardiac tamponade consists of a greater than normal (10 mmHg) inspiratory decline in systolic arterial pressure
 inspiratory decline in systolic arterial pressure")
39
Since both ventricles share a tight incompressible covering, the inspiratory enlargement of the right ventricle in cardiac tamponade compresses and reduces left ventricular volume leftward bulging of the IVS further reduces the left ventricular cavity as well.

40
Thus, the normal inspiratory augmentation of right ventricular volume causes an exaggerated reciprocal reduction in left ventricular volume.

41
respiratory distress increases the fluctuations in intrathoracic pressure, which exaggerates the mechanism just described. RV MI may resemble cardiac tamponade with hypotension, elevated JVP, an absent y descent in the JVP, and, occasionally, pulsus paradoxus.

42
Differential Diagnosis of Paradoxical Pulse
constrictive pericarditis hypovolemic shock, acute and chronic obstructive airway disease pulmonary embolus. RV MI

43
Electrocardiographic abnormalities
1.reduced voltage 2.electrical alternans Electrical alternans caused by anterior-posterior swinging of the heart with each heart beat.

45
Treatment Patients with acute pericarditis should be observed frequently for the development of an effusion if a large effusion is present, the patient should be hospitalized and pericardiocentesis carried out or the patient should be watched closely for signs of tamponade

46
Chronic Constrictive Pericarditis

47
Constrictive Pericarditis(CP)results of healing a fibrinous or serofibrinous pericarditis or the resorption of a chronic pericardial effusion The latter gradually contracts and forms a firm scar, which may be calcified, encasing the heart and interfering with filling of the ventricles

48
Etiologies CP may follow acute or relapsing viral or idiopathic pericarditis Trauma with organized blood clot Cardiac surgery of any type Mediastinal irradiation Purulent infection,TB Histoplasmosis Neoplastic disease (especially breast cancer, lung cancer, and lymphoma) Rheumatoid arthritis, SLE Chronic renal failure with uremia treated by dialysis.
 Rheumatoid arthritis, SLE. Chronic renal failure with uremia treated by dialysis.")
49
The basic abnormality in this patients is the inability of the ventricles to fill because of the limitations imposed by the rigid, thickened pericardium myocardial function is normal or only slightly impaired However, the fibrotic process may extend into the myocardium and cause myocardial scarring and atrophy

50
In constrictive pericarditis, JVP display an M-shaped contour, with prominent x and y descents.
The y descent, which is absent or diminished in cardiac tamponade, is the most prominent deflection in constrictive pericarditis

51
The usual presentation consists of signs and symptoms of right-sided heart failure.
Include lower extremity edema, vague abdominal complaints, and passive hepatic congestion. As the disease progresses, hepatic congestion worsens and can progress to ascites, anasarca, and jaundice due to cardiac cirrhosis.

52
In end-stage , the effects of a chronically low cardiac output are prominent, including severe fatigue, muscle wasting, and cachexia. Other findings include recurrent pleural effusions and syncope.

53
CP can be mistaken for any cause of right-sided heart failure
As well as end-stage primary hepatic disease. venous pressure is not elevated in the latter circumstance.

54
Physical Examination markedly elevated JVP with a prominent, rapidly collapsing y descent. This, combined with a normal x descent, results in an M- or W-shaped contour

55
The cervical veins are distended and may remain so even after intensive diuretic treatment, and venous pressure may fail to decline during inspiration (Kussmaul's sign). The latter may occur in chronic pericarditis , tricuspid stenosis, right ventricular infarction, and restrictive cardiomyopathy.

56
The pulse pressure is normal or reduced.
In 1/3 of cases, a paradoxical pulse can be detected. Congestive hepatomegaly is pronounced and may impair hepatic function and cause jaundice ascites is common and is usually more prominent than dependent edema

57
The apical pulse is reduced and may retract in systole (Broadbent's sign).
The heart sounds may be distant Pericardial knock, in early diastole occurs with the abrupt cessation of ventricular filling. A systolic murmur of tricuspid regurgitation may be present.

58
The ECG frequently displays :
Low voltage of the QRS complexes Diffuse flattening or inversion of the T waves. Atrial fibrillation is present in about one-third of patients.

59
The CXR shows a normal or slightly enlarged heart
Pericardial calcification is most common in tuberculous pericarditis. Pericardial calcification may,occur in the absence of constriction.

61
More accurate modalities
Echocardiography MRI CT-scan

62
Treatment Pericardial resection is the only definitive treatment of constrictive pericarditis and should be as complete as possible. Dietary sodium restriction and diuretics are useful during preoperative preparation.

63
Thanks for your Attention

Similar presentations












 Occurs when the right ventricle fails as an effective forward pump, causing back-pressure of blood into the systemic.>")







 Definition: Rheumatic fever (RF) is an autoimmune disease affecting the heart and extra- cardiac.>")

