Download presentation
Presentation is loading. Please wait.

1
WAEL TANTAWY MD CONSTRECTIVE PERICARDITIS CASE PRESENTATION

2
Etiology Historically, the most common cause of conestrictive pericarditis was TB pericarditis, however, now it is rare. Other causes include recurrent episodes of viral or purulent pericarditis. post-cardiac injury/surgery. Neoplastic pericarditis, mediastinal radiation, chronic uremia, or Collagen vascular disease.

3
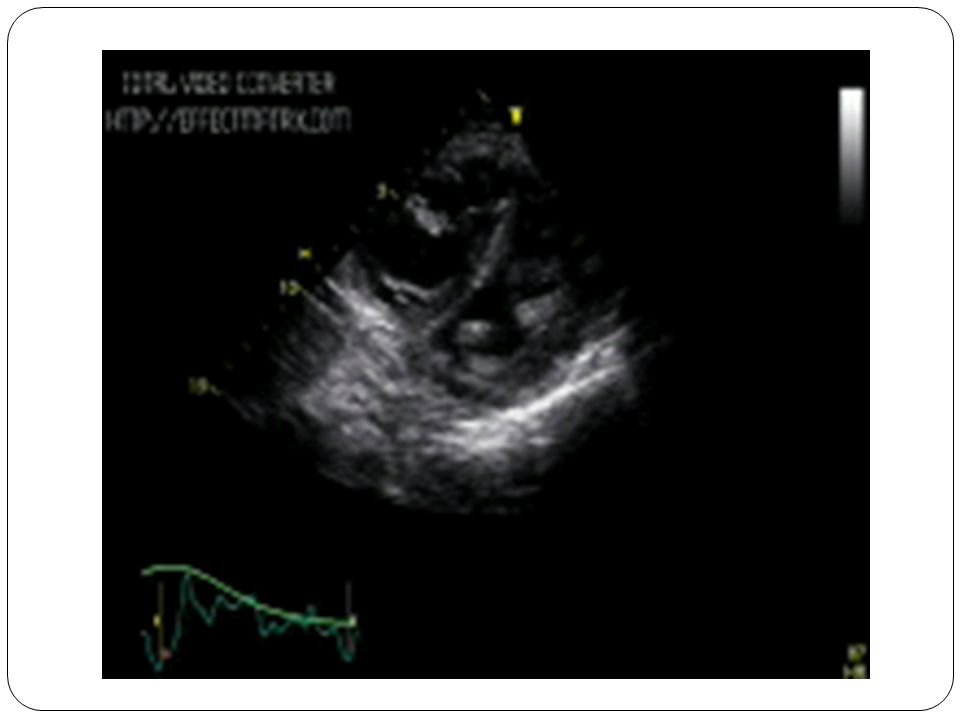
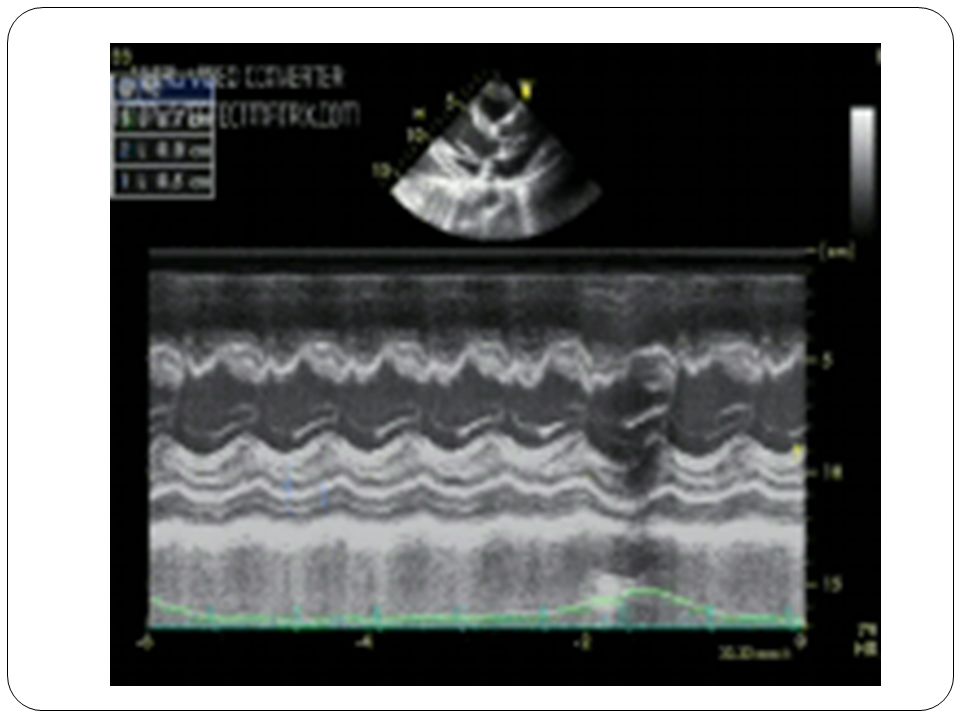
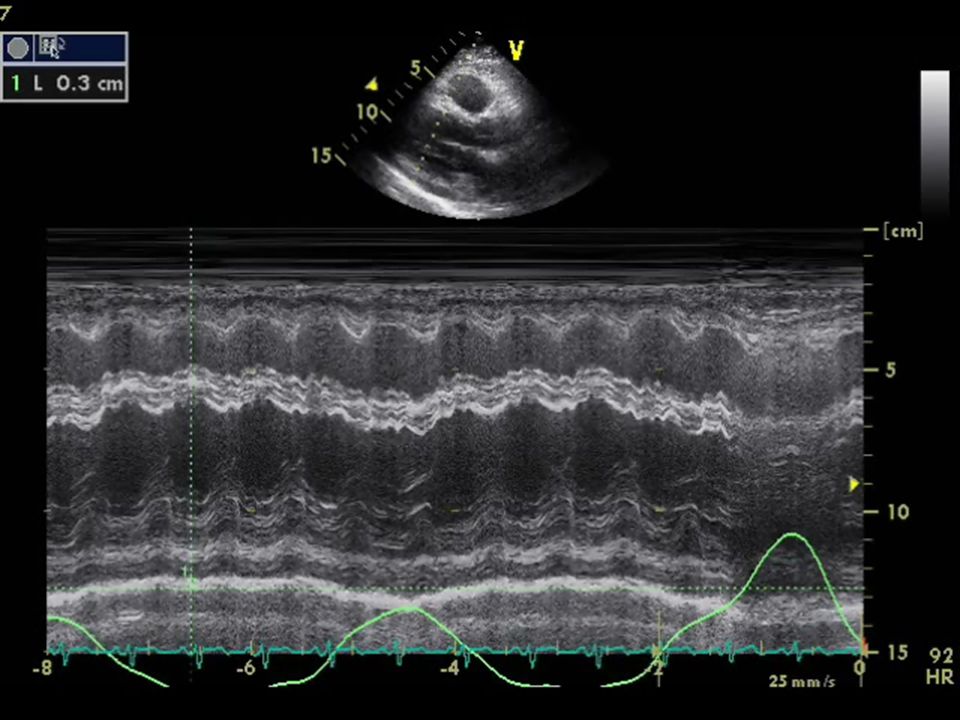
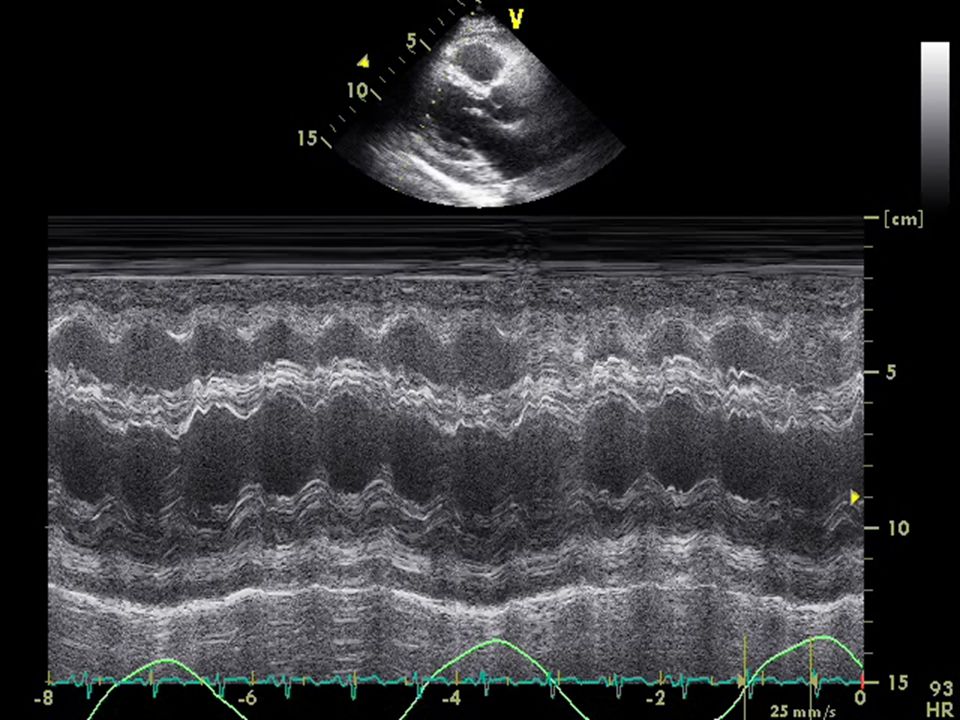
Echo in Constrictive pericarditis Certain echo findings are consistent with the diagnosis of constrictive pericarditis Pericardial effusion ± fibrinous adhesions. Pericardial thickening ± calcification which may appear as multiple linear & parallel echoes posterior to the LV by M-mode Abnormal septal motion: septal “bounce” diastolic “checking,” septal “shudder” “Flattening,” of the LV during mid- to late diastole, due to stiff pericardium(in 85% of pts

5
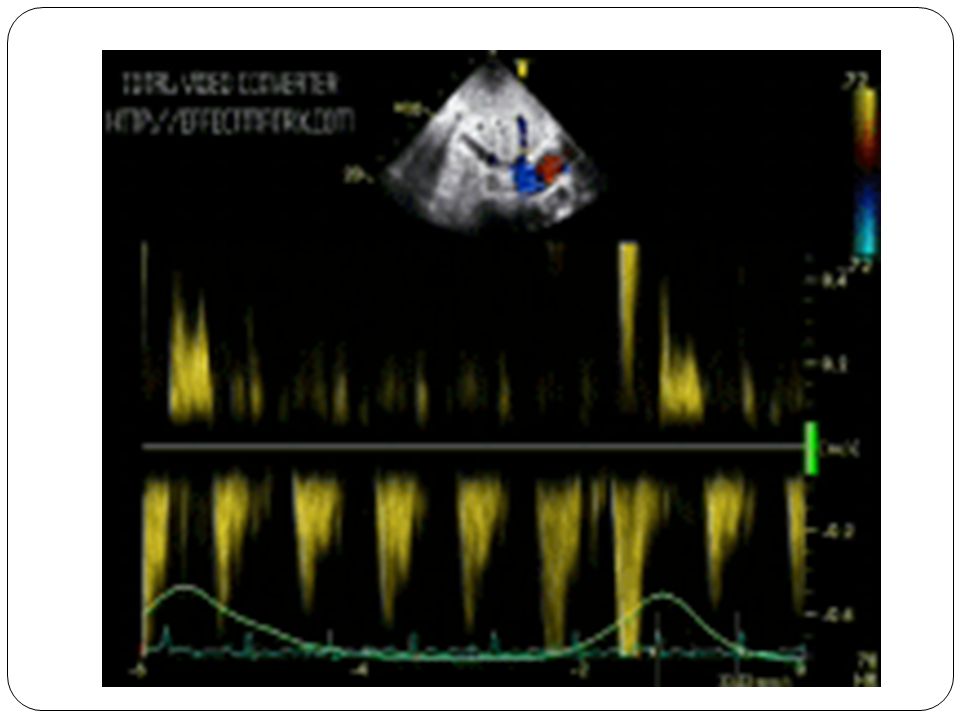
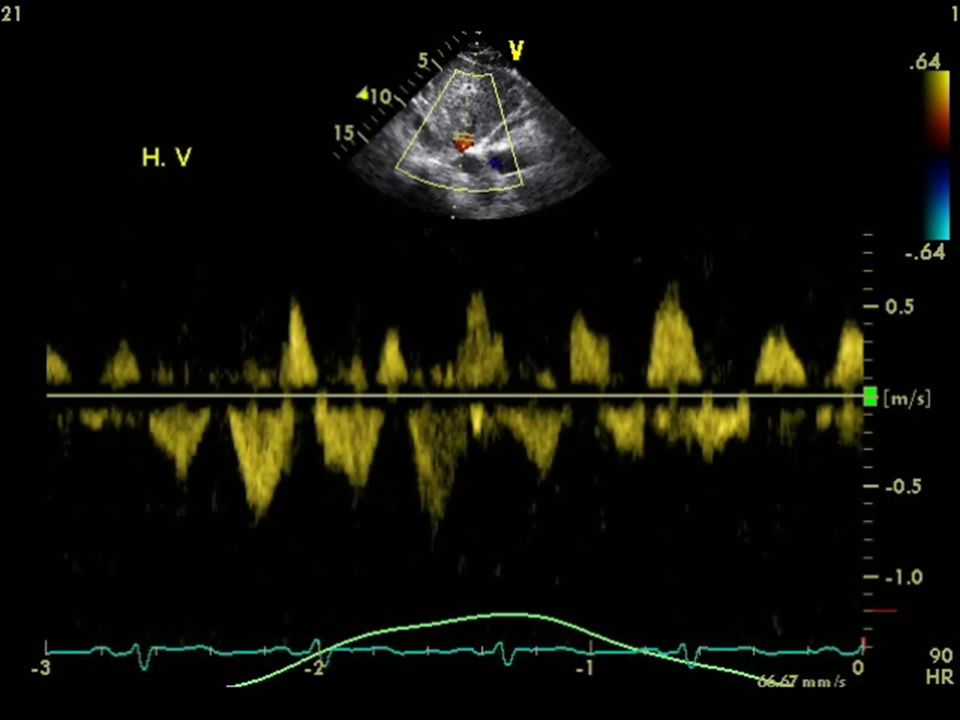
Echo in Constrictive pericarditis CONT Doppler provides further evidence of constrictive physiology. Transmitral Pulsed Doppler shows increased E velocity & reduced A-wave velocity, due to impaired late diastolic filling. Marked respiratory variation may be noted in early diastolic filling, with >25% increase of TV flow & >25% decrease of MV flow during inspiration

8
clinical presentation The clinical presentation of constrictive pericarditis is usually subtle and gradual. The Patients may C/O weakness, fatigue, & anorexia exertional dyspnea and peripheral edema. Physical findings reflect the consequences of chronically elevated heart pressures,

9
Case ICase I 40 y S/M 40 y S/M K/C of ESRD on dialysis & sever osteoprosis. K/C of ESRD on dialysis & sever osteoprosis. Presented with hypotension & SOB. Presented with hypotension & SOB. TTE done showed pericardial effusion (managed medically by increased dialysis cession) TTE done showed pericardial effusion (managed medically by increased dialysis cession) 2 months later he presented by recurrent attacks of tachy arrhythmia (S.tachycardia & SVT) 2 months later he presented by recurrent attacks of tachy arrhythmia (S.tachycardia & SVT)
 TTE done showed pericardial effusion (managed medically by increased dialysis cession) 2 months later he presented by recurrent attacks of tachy arrhythmia (S.tachycardia & SVT) 2 months later he presented by recurrent attacks of tachy arrhythmia (S.tachycardia & SVT).")
16
Case II 27y male History of RTA 2y ago complicated by haemopericardium and pericardiocentesis was done twice in Rhyad. Presented with 3 months history of exertional SOB, abdomenal distention & LL oedema.

29
Case III 38Y FEMALE Exertional SOB FC II-III/IV History of flue like symptoms two weeks before Diagnosed as viral pericarditis with moderate pericardial effusion, ttt medically 6 monthes later started to have progressive exertional SOB with paroxysmal attacks of irrigular palpitation 48 h holter revealed PAF

Similar presentations